
Abstract
Despite hernias being one of the most common surgical problems in low and middle income countries, very little is known about the impact that having a hernia has on the quality of life of patients in these settings. We performed a pilot study to understand how living with a hernia impacts on the quality of life. Twelve semistructured interviews were performed. A number of themes were identified. These demonstrated the significant impact on physical health, ability to work, psychological health and social relationships. Further work is required to better understand the patient perspective and ensure that hernia operations improve quality of life in these settings.
Dear Editor,
Health-related decisions should be made in dialogue with the patient, building on the patient’s perception of their health status and the impact of the condition on their quality of life.1,2 However, in order to enhance the quality of life by procedures such as hernia repair, it could be argued that we need first to understand how the untreated problem impacts on quality of life. Little has been done to document the quality of life and ability to work both before and following surgery.
No studies exploring experiences of living with hernia and how it impacts life in sub-Saharan Africa currently exist in the literature even though abdominal wall hernia repair is one of the most common surgical procedures performed globally3–5 with the greatest burden of unmet need located in resource-poor settings. 3
A pilot study was conducted at Ndola Teaching Hospital in Ndola, Zambia, aiming to study how the experience of living with a hernia affects the quality of life through qualitative semi-structured interviews. Data collection was performed in May and June 2019.
Twelve interviews were conducted. Patients were invited to participate if they were aged 18 years old or over, planned for elective hernia surgery and were able to give informed consent. The frequency of themes is shown in Table 1.
Physical symptoms leading to pain and discomfort which limited daily function was the most commonly reported experience of living with a hernia. The consequences of this impacted on the ability to perform basic manoeuvres like bending over or sitting to strenuous activities like walking long distances or picking up or carrying heavy items.
Psychological problems were also described. Participants worried about the future if not cured by the operation because the hernia had such a significant impact on them. They reported that they had been forced to turn down jobs, lose business and income, had not been able to grow crops as planned and had not been able to manage their business as before due to their symptoms. They were also concerned about their ability to support their family. Income could be affected even in the absence of symptoms. One participant had been denied a certificate of being physically fit. As this was mandated to be eligible to work in the mine, he was unable to work without an operation even though he had few symptoms. One participant had been forced to give up playing football, which to him was a great loss both socially and psychologically.
Frequency of themes.
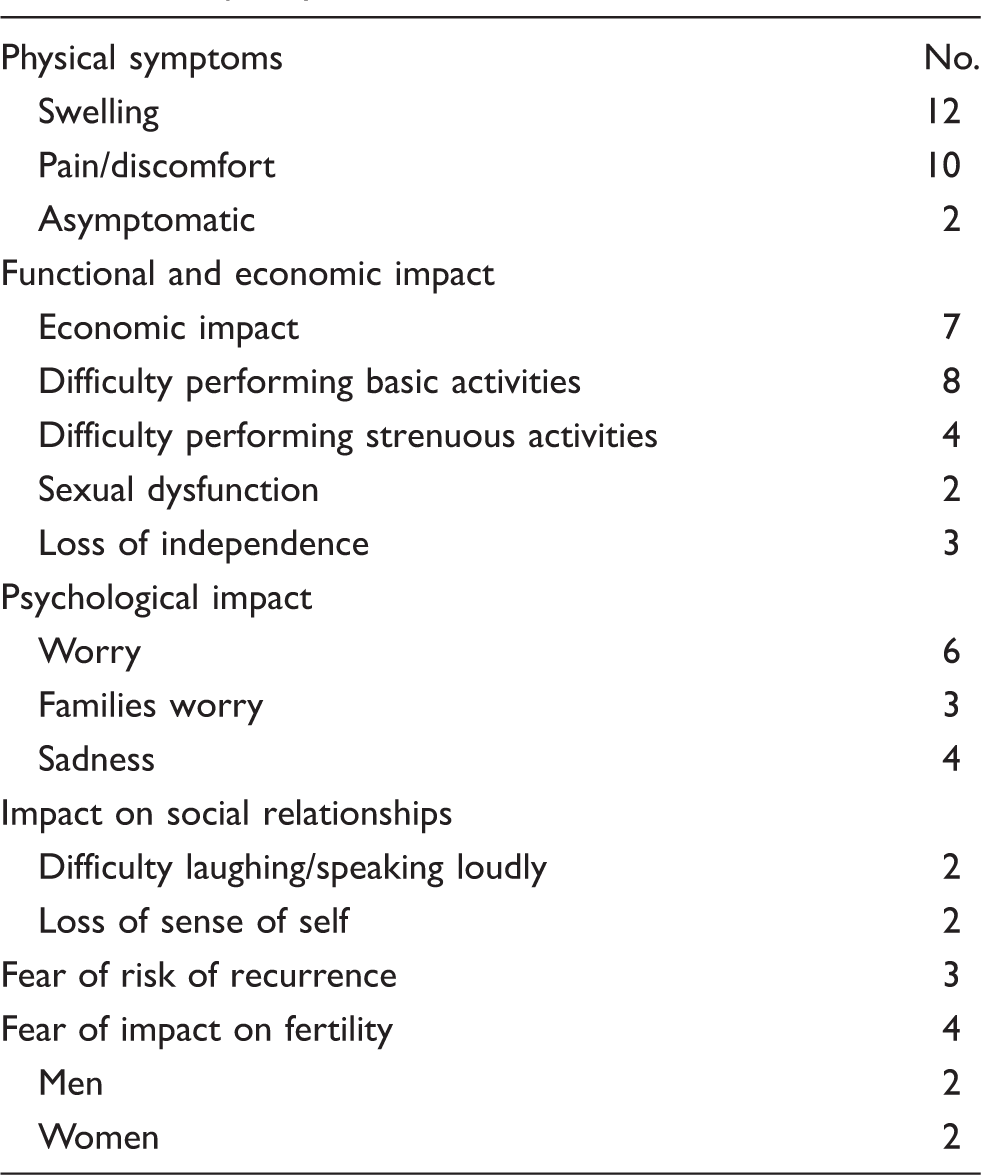
Sexual dysfunction was also noted by two participants who were struggling to engage as they wished in their sex life and they attributed this to the hernia.
Loss of independence from the hernia caused distress. For example, in one interview, having to depend on other family members for economic support resulted in the patient feeling sad.
Most participants expressed the expectation that they would return to their previous health and function after the operation even though some expressed concerns about the risk of recurrence. Both men and women expressed concerns about how the operation may affect their chances of conceiving post-operatively.
Our findings demonstrate that adults admitted for elective hernia repair suffer with physical, economic, psychological and social impact on their quality of life as a result of the hernia. But our data also suggest that individuals risk severe consequences when not being able to provide for themselves and their families due to their impairment.
Footnotes
Availability of data
All data relevant to the study are included in the article.
Authors’ contributions
EL and CG conceptualised the study. EL, FC, CG and JM developed the protocol and survey tools; EL, FC and CO collected the data. EL, FC and CG analysed the data; all authors contributed to the interpretation of the results and write up of the manuscript; all authors approved the manuscript for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.