
Abstract
Self-inflicted injury, the most common form of intentional injury, disproportionately affects low-income countries, but is poorly described in this setting. This retrospective review of the 2008–2018 trauma registry at a referral hospital in Malawi included all victims of intentional injury ≥10 years. Self-inflicted injuries were compared to assaults. The primary outcome was in-hospital mortality. Common mechanisms of self-inflicted injuries were fall from height, poisoning, and penetrating injury. In-hospital mortality from self-inflicted injury was 8.8% vs. 1.9% for assault. Those who died from self-inflicted injury were more often older (median 34 vs. 26 years, p < 0.001), male (91.9% vs. 67.8%, p < 0.001), unemployed (32.8% vs. 6.4%, p < 0.001), and most commonly died by hanging (60%). The odds of in-hospital mortality after self-inflicted injury was four times assault (OR 4.0 [95% CI 1.4–11.5], p = 0.01). The trauma registry proved useful for describing self-inflicted injury in this setting.
Introduction
Injury is a leading cause of death and disability worldwide. While injury-related mortality has emerged as a growing global public health priority, unintentional injuries, such as road traffic injuries, drowning, and falls, have remained the focus of such efforts. 1 However, intentional injuries account for one-third of all injuries worldwide. 2 Furthermore, the burden of intentional injuries is disproportionately borne by those living in low- and middle-income countries (LMICs). 3 Intentional injuries are classified as self-inflicted, including self-harm and suicide; interpersonal violence, such as family and intimate partner violence; and collective violence, such as armed conflict. 4 Despite being primarily underreported, self-inflicted injuries account for over half of all intentional trauma worldwide. 5
Suicide is responsible for an estimated 800,000 global deaths annually and is the second leading cause of death in young people aged 15–29 years. 6 In high-income countries (HICs), firearms are the most common method of suicide, whereas hanging and poisoning are more frequent in LMICs. 3 Even more common than suicide is non-fatal self-inflicted injury, with incidence rates of 20–30 fold higher than suicide. 7 Self-inflicted injury results from a complex interrelationship between biological, psychological, and socioeconomic factors. Mental health disorders, particularly depression, psychosis, and substance use disorders, are well-documented risk factors for self-injurious behaviour.8,9 In addition to psychiatric disorders, socioeconomic and cultural factors play a prominent role in self-inflicted injury. In sub-Saharan Africa (SSA), social and cultural factors such as displacement in times of conflict, prior experiences of violence or abuse, and feelings of oppression due to stringent societal and religious norms are risk factors cited for self-injurious behaviour in this setting. 10
There is a lack of data from SSA regarding the epidemiology and outcomes of self-inflicted injury. There is a common perception that suicide rates are low in SSA; however, the true magnitude of self-inflicted injury in this region is unknown owing to the lack of reliable data collection and stigma surrounding reporting. While there are several barriers to systematic data collection on mental health in resource-limited settings, self-inflicted injury in the context of trauma provides a unique opportunity for leverage of existing resources. To fill the gap in knowledge on suicide and suicidal behaviour in a resource-limited setting, we evaluated self-harm through the lens of traumatic injury. The aims of our study were to evaluate the demographic and clinical characteristics, outcomes, and predicted in-hospital mortality associated with self-inflicted injury at a tertiary care centre in Lilongwe, Malawi.
Methods
We performed a retrospective analysis of prospectively collected data in the trauma registry at Kamuzu Central Hospital (KCH) from February 2008 to May 2018. KCH is a 900-bed tertiary care centre that serves eight districts in Malawi’s central region, with a catchment population of approximately 6 million persons. Its facilities include a 4-bed 24-h emergency department (ED), a 4-bed high dependency unit, a 6-bed intensive care unit (ICU), and a 31-bed burn unit. There is no formal prehospital care system; only limited basic life support is available before hospital admission.
We collected demographic and injury-related data of all patients ≥10 years of age presenting to the ED at KCH with a traumatic injury. We classified injuries as intentional if the intent was documented as self-inflicted or assault. Those with unintentional injury (64,491 [67.2%]), missing intent (679 [0.7%]), or missing mortality data (3835 [3.8%]) were excluded from further analysis (Figure 1).
Study inclusion flow diagram.
We performed bivariate analyses comparing the demographic and clinical characteristics of self-inflicted injuries, assault and fatal, and non-fatal self-inflicted injuries. The variables analysed included demographics, mechanism, the most severely injured anatomic location, admission disposition, interventions, length of stay, and crude in-hospital mortality. We calculated the median, interquartile range, and shape of the distribution for each continuous variable and tabulated frequencies for categorical variables. We compared continuous variables using the Kruskal-Wallis test and categorical variables using Pearson’s χ 2 test. We considered a value p < 0.05 as statistically significant.
We performed a multivariate logistic regression analysis to determine the relative odds of mortality following intentional injury, comparing self-inflicted injury to assault. The odds of mortality were adjusted for injury severity using the Malawi Trauma Score (MTS), a predictive tool for assessing injury severity that ranges from 2 to 32 and incorporates age, sex, anatomic location of injury, level of consciousness, and absence or presence of a radial pulse on arrival. 11 We utilised STATA V.16 (StataCorp, College Park, TX) to perform all statistical analyses.
Results
Bivariate analysis of assault vs. self-inflicted intentional injuries.

The mechanism of self-inflicted injury was most commonly a fall from height (323 [45.9%]), poisoning (101 [14.4%]), or penetrating injury (109 [15.5%]), including 8 gunshot wounds, 4 bites, and 97 stabbings (Table 1). The vast majority committed their act of self-injury at home (417 [60.4%]). The extremities were most commonly the most severely injured anatomic location (431 [62.1%]) followed by the head and neck (172 [24.8%]). Upon arrival to KCH, most patients with self-inflicted injuries were able to be treated in the ED and discharged home (546 [77.2%]). A total of 57 (8.1%) were brought in dead and 2 (0.3%) died in the ED. Twenty-four (3.6%) patients underwent at least one procedure, including 5 laparotomies (0.7%), 12 laceration repairs (1.7%), 4 orthopaedic procedures (0.6%), 1 burn procedure (0.1%), and 1 amputation (0.1%). Crude in-hospital mortality for self-inflicted injuries was 8.8% compared to only 1.9% following assault, p < 0.001.
Bivariate analysis of non-fatal vs. fatal self-inflicted injuries.
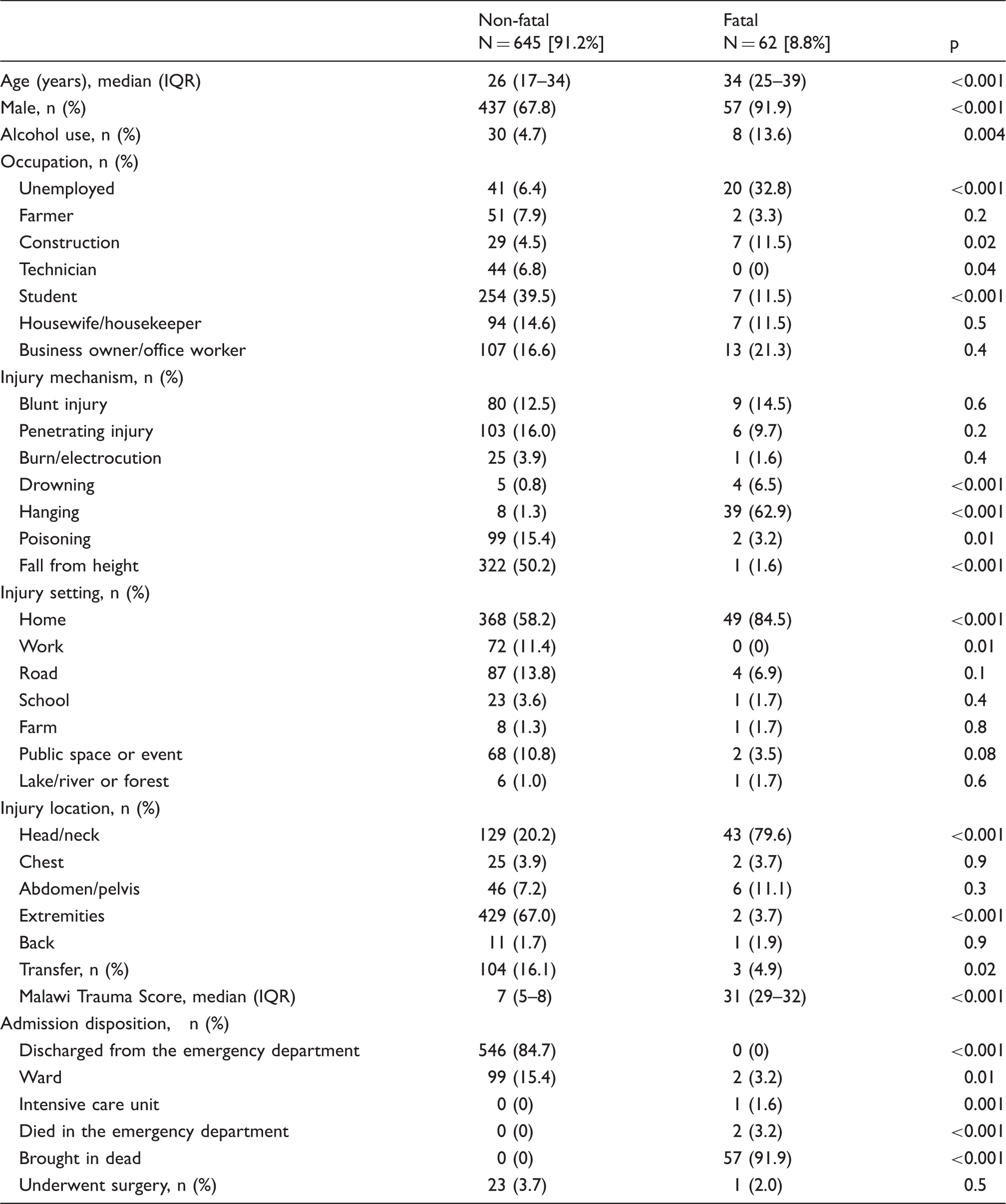
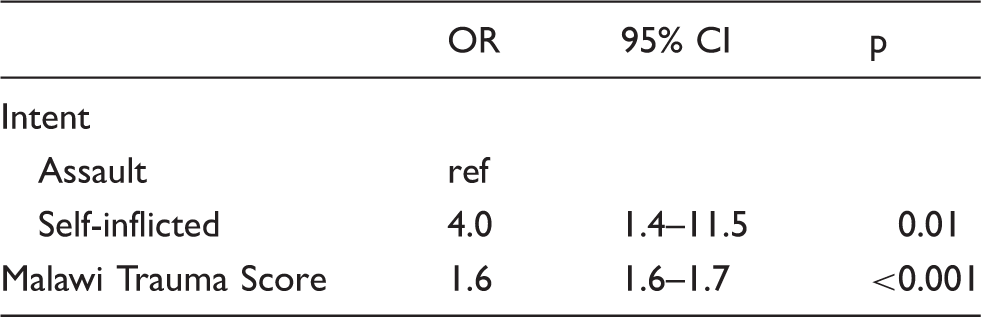
Odds of mortality associated with a self-inflicted injury.
Discussion
Intentional injuries contribute to a considerable proportion of the global burden of trauma. Of all intentional injuries, more deaths occur due to suicide than from homicide and war combined. 12 The vast majority were declared dead in the ED and far more likely die in the pre-hospital setting so not captured by any hospital registry. We also show a statistically significant increase in the odds of mortality following a self-inflicted injury that was four times that of an intentional injury by assault.
Reported rates of self-inflicted injury vary widely in SSA. The lifetime prevalence of attempted suicide is as low as 0.7% in Nigeria to as high as 6% in Liberia, with mean annual rates ranging from 0.1 per 100,000 in Ghana to 100 per 100,000 in Namibia.13–16 However, a 2014 review of suicidal behaviour noted that only 16 of 54 African countries report self-inflicted injury, and only 11 countries report on completed suicide to the World Health Organization. 17 Similarly, a 2020 systematic review identified published literature on suicidal behaviour in SSA from only 40% of the region. 10 Of the available published literature, the mechanism of suicide is similar across African countries and consistent with our findings of predominately hanging, poisoning, and drowning; however, we did find a higher frequency of blunt injuries, such as vehicular suicide.10,18 In contrast, the most common method of suicide in the USA is firearm use, accounting for 35% of firearm suicide mortality worldwide. 19
The characteristics of those with self-inflicted injuries in our cohort are similar to regional and global estimates. Self-injury in our cohort was committed mostly by males. Globally, males commit suicide almost twice as frequently as women, with even higher rates up to 21:1 occurring among males in Africa.3,17 The majority of our in-hospital mortality occurred among males who were unemployed, concordant with well-established correlations between socioeconomic status and suicide in both HICs and LMICs.7,20 Young adults aged 18–35 years make up the majority of self-inflicted injuries in South Africa, Tanzania, and Zambia.21–23 A similarly hospital-based study in Mwanza City, Tanzania found a median age of 24 years among all victims of intentional injury, both assault and self-inflicted injury. 23 In Pretoria, South Africa suicides most frequently occurred in the 21–40 year age range. 21 In a school-based survey of adolescents in grades 7–10 across Zambia, 11.9% reported a history of intentional injury to themselves, highlighting the burden of psychological stress among this age group in this setting. 22
Although studies suggest that the prevalence of depression in LMICs and SSA countries is comparable to that found in HICs, at around 10–20% of the population at any one time; most people living with depression go untreated. 24 A prior cross-sectional survey study in Malawi found the prevalence of depression to be as high as 30% in the out-patient primary health care setting, but the rate of detection by clinicians was 0%. 25 Training on mental health screening is, therefore, an important prevention strategy that is desperately needed in this setting. Owing to the association of depression and suicidal behaviour with other health problems such as HIV and substance abuse, there is an opportunity to implement such mental health interventions in alternate settings. For example, as the prevalence of depression in persons living with HIV is 9–19%, screening programmes in HIV clinics have been successful in preliminary studies. 26 As alcohol use raises the likelihood of a suicide attempt sevenfold, 27 screening for mood disorders and suicidal behaviour could be incorporated into existing efforts targeting alcohol abuse. In the Adjumani District of Uganda where rates of suicidal behaviour are high, mental health services were implemented by local community volunteers. 28 An additional prevention strategy includes encouraging mental health awareness at an early-age through school-based interventions. 29 Several socio-economic factors influence suicidality in youth living in LMICs, such as loss of one or both parents, sex working, and expectation of an early death. 30 The psychosocial stress of poverty, including financial insecurity, unemployment, and lower education, results in an increased risk of mental health disorders, especially in rural populations with the least access to care. 31 Screening for suicidal behaviour and counselling is of particular need in populations with these risk factors.
Several barriers exist in addressing self-inflicted injury in resource-limited settings. First, lack of data collection coupled with significant underreporting limits knowledge of the true scope of self-inflicted injury and impede societal and governmental prioritisation. As injury surveillance has gained importance in LMICs, many hospitals have an existing trauma registry collecting data on demographics, intent, and mechanism, which are invaluable in filling the gaps in knowledge on suicidal behaviour in this setting. Also, investigations into the efficacy of setting-specific interventions are needed. For example, in our cohort the majority of non-fatal self-inflicted injury was committed by students; therefore, school-based initiatives that increase mental health awareness and coping mechanisms may be beneficial. However, despite survey data showing a high prevalence of suicidal ideation among school-aged children from this region, evidence for the efficacy of school-based mental health interventions is lacking from LMICs.22,32 Additionally, restricting the means for self-inflicted injuries has proven efficacious in HICs, but could be challenging in LMICs. In our cohort, poisonous substances were the third most common mechanism of self-injury and is frequently used across LMICs. 33 Limiting access to these substances is particularly challenging as most are household items such as bleach, organophosphate pesticides, or readily available medications such as the antimalarial Chloroquine.34,35
Lastly, resource limitations hinder in-hospital management strategies available in HICs beyond the stabilisation of acute injuries. The vast majority of patients in our study cohort were managed in the ED and discharged home. In the USA, self-injurious behaviour often mandates an involuntary admission with in-patient pharmacologic and psycho-therapeutic management. In Malawi, mental health services are limited with only three psychiatrists and three psychiatric facilities in the whole country. 36 In HICs, there are an estimated 105 psychiatrists, 140 psychologists, and 330 psychiatric nurses per million population. In contrast, LMICs have 0.5, 0.4, and 1.6, respectively. 31
Our retrospective review is subject to the limitations of the study design. Many self-inflicted injuries were likely treated at home and thus not captured by this dataset. While prehospital deaths are often captured by this registry as they require passage through the ED for declaration of death and receipt of a death certificate, knowledge of intent must have been reliably reported and documented to be included in this analysis. Prehospital deaths secondary to suicide are therefore also likely under-captured. Of those who did survive and present to the hospital, the injury intent was self-reported; therefore, we suspect significant under-reporting of self-harm in our setting. The lack of distinction between intentional acts of self-harm and accidental self-inflicted injuries, for example in risk-taking behaviour, may also limit our findings. Additionally, vital sign data were missing in 20% of our cohort. Further, with care, children as young as six years, are able to verbalise their distress and intention to end their own lives. Although 513 children under 10 years of age were documented as self-inflicted injury in our registry, we excluded children under 10 years due to their questionable ability to provide credible diagnostic information, especially in lieu of a validated semi-structured interview performed by a trained child psychiatrist. 37 Despite these limitations, our study provides ample evidence of need for further action on self-injury in SSA.
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the NIH Fogarty International Center (Grant #D43TW009340).