
Abstract
Dengue, a common tropical viral disease, often has complications of thrombocytopenia causing bleeding and warranting blood transfusion. This is costly in low-income settings. We conducted an observational study using a relatively new parameter called immature platelet fraction which indicates regeneration of platelets by the bone marrow. Our study on 124 dengue patients showed a strong correlation between platelet count and immature platelet fraction and we observed that 96.1% and 97.4% patients showed rise in platelet count at 24 and 48 h, respectively. In the absence of bleeding, platelet transfusion was prevented in 64% of patients with an IPF level of 10% or more.
Introduction
Among arthropod-borne viral diseases, dengue infection is the most common and one of the most important emerging infectious disease of urban and semi-urban areas in tropical regions of the world. 1 Out of almost 2.5 billion people living in dengue-risk regions worldwide, around 100 million new cases occur every year. 2 The need for transfusion of platelets in dengue infection is indicated in patients with severe bleeding and low platelet counts. The immature platelet fraction (IPF) measures young and reticulated platelets with high RNA content recently released in the peripheral blood. 3 Data regarding the correlation of IPF in Dengue infection are limited and the clinical applicability of this parameter is not well known.
Materials and methods
We conducted an observational study over a period of two and half years (June 2015–December 2017) in Sir Ganga Ram Hospital on 124 patients, above 18 years of age, diagnosed with Dengue infection (Dengue NS1 or IgM or both positive) having a platelet count <100/m 9 . The study was conducted on 50 patients retrospectively from June 2015 to January 2016 and prospectively on 74 patients from then till December 2017.
For the prospective arm of the study, a detailed clinical history of symptoms (fever, rash, headache, retro-orbital pain and bleeding) was taken along with history of any comorbid illness and for the retrospective arm such data were obtained from hospital records. Patients were then sub-classified according to the World Health Organization classification of dengue 2012.
In the prospective arm, full blood count, liver and renal function tests, chest radiograph and abdominal ultrasound scan (if required) were done. Daily monitoring of platelet counts and IPF was conducted from the first day of admission till outcome (discharge and death). IPF was measured on Sysmex XN 2000 using the PLT-F method.
In addition, clinical events such as bleeding, platelet/packed cell transfusion and requirement for intensive care were recorded along with monitoring trends of IPF and platelets. The study algorithm regarding haemorrhage is shown in Figure 1.
Algorithm of the study.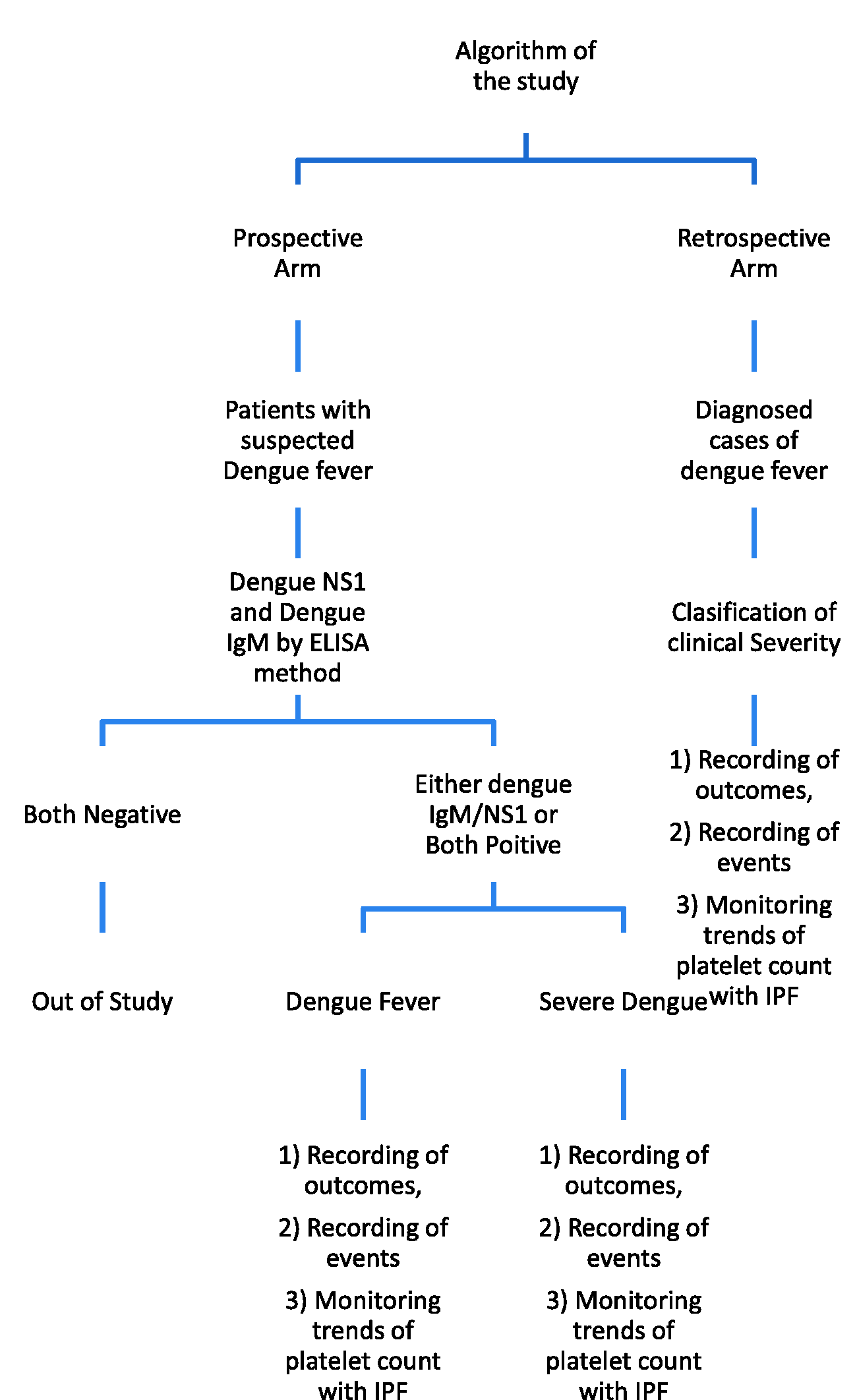
Major bleeding was defined as:
Fatal bleeding, and/or Symptomatic bleeding in a critical area or organ, such as intracranial, intraspinal, intraocular, retroperitoneal, intra-articular or pericardial, or intramuscular with compartment syndrome, and/or Bleeding causing a fall in hemoglobin level of 20 g/l or more, or leading to transfusion of two or more units of whole blood or red cells.2–6
Any bleed other than the above-mentioned bleed was termed as minor bleed. Thrombocytopenia was defined as a platelet count of less than 150 × 109. 7
Results
In our observational study on 124 patients with a mean age of 34.1 years, 53 (42.74%) had simple dengue with no alarm signs, 67 (54.0%) had alarm signs, and 4 (3%) had severe dengue. The highest frequency was observed in the second and third decade of life (25.8% each) with males accounting for 71.8% of cases. Bleeding was reported in 10 (8%) of whom one had major and nine minor bleeding.
In terms of clinical events, 23.38% patient required platelet transfusion, 8 patients (6.45%) required HDU is High Dependency Unit admission, 2 patients (1.61%) required intensive care unit (ICU) admission out of which 1 patient expired. On daily monitoring of platelet count and IPF levels it was observed that with IPF values above 10%, 90.9% patients and 93.5% patients showed increase in platelet counts at 24 h and 48 h, respectively (Figure 2). After attaining peak IPF, it was observed that 96.1% and 97.4% patients showed rise in platelet count at 24 and 48 h, respectively. Rise in platelet counts was strongly correlated (p < 0.001) with peak IPF levels. In patients with severe thrombocytopenia (platelet counts <150/m
9
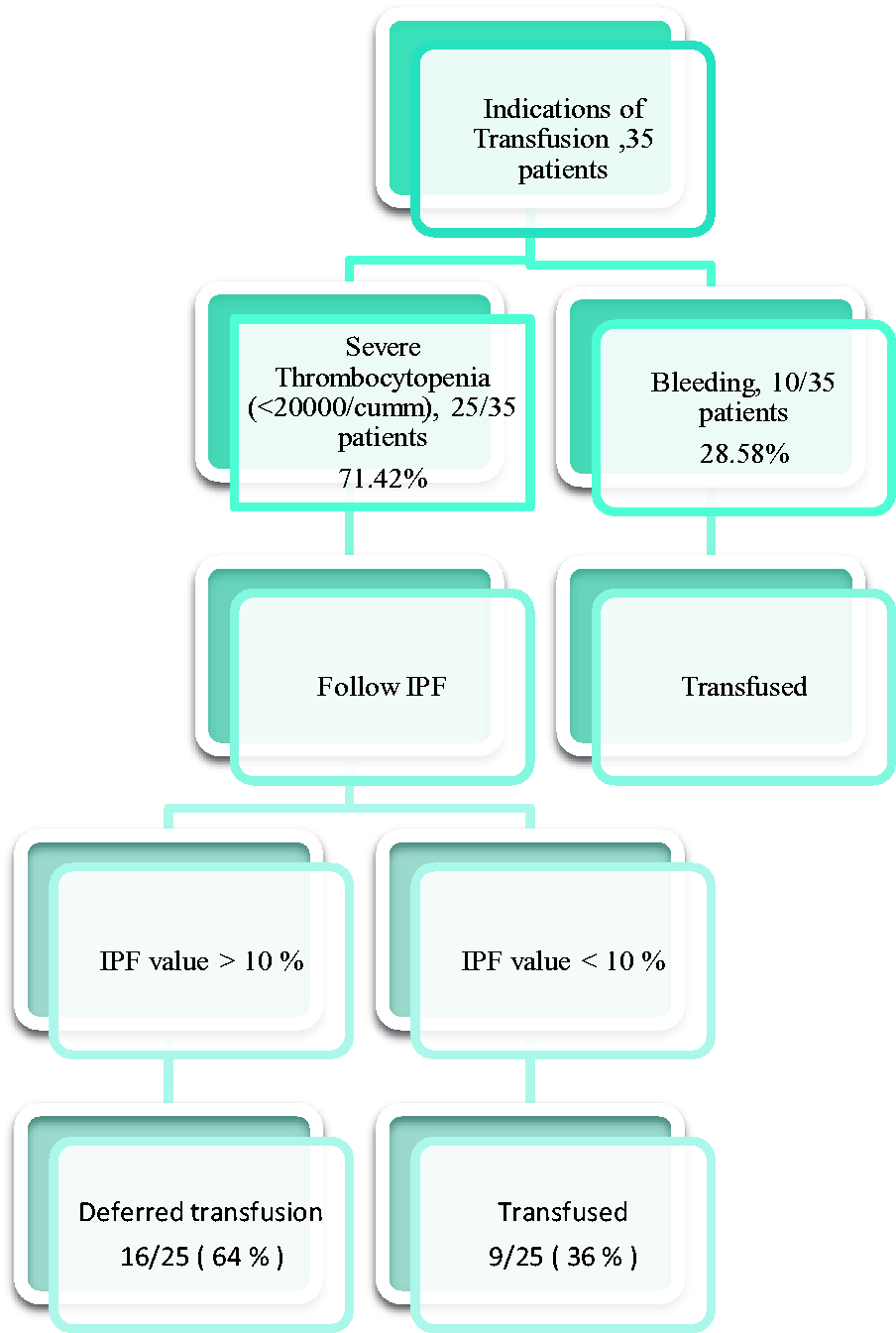
)in the absence of bleeding, platelet transfusion was prevented in 64% patients in our study by measurement of IPF levels (Figure 3).
Correlation of IPF and platelet counts in a patient. Prevention of platelet transfusion on the basis of immature platelet fraction.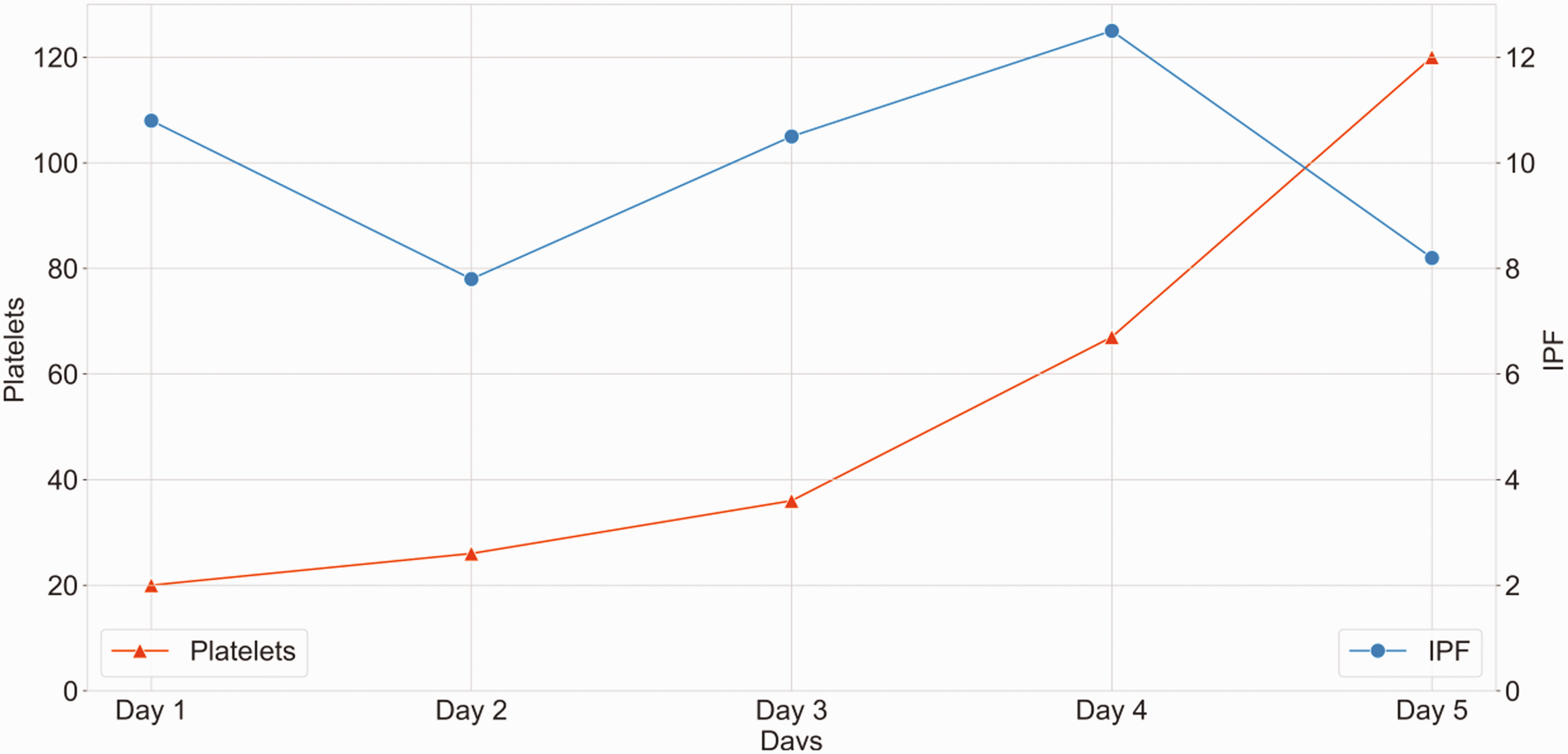
Nine patients with minor bleed and low platelets were given platelet transfusion in view of hemodynamic instability on presentation. Six units of random platelet concentrate and one platelet apheresis were transfused for these patients. One patient whose platelet count was 20/m 9 and IPF was 6% presented with massive intracranial haemorrhage and required admission in ICU and blood transfusion as well. This patient died.
Discussion
The most common complications observed in dengue patients are thrombocytopenia and bleeding. Guidelines stipulate platelet transfusion in case of active bleeding or severe thrombocytopenia. 6
However, platelet transfusions are mostly panic reactions rather than medically indicated in dengue infection, and inappropriate transfusion ranging from 13% to as high as 56.2% has been reported.6–8
Bleeding is multifactorial in aetiology and can be attributed to DIC- disseminated intravascular coagulation with clotting factor deficiency, and loss of vascular integrity apart from thrombocytopenia. 9 This observation is supported by no significant difference in the frequency of bleeding in patients being shown in those who did or did not receive any transfusion. 10 Major bleeding is unusual in clinically stable patients unless the platelet count are less than 500/m 9 . 9
Using a cut-off value of IPF in our study as 10%, over 90% of patients demonstrated platelet recovery within 48 h, as in other studies. 11
Hence, IPF can have a massive impact on utilisation of health-care facilities in countries with limited resources and high dengue prevalence like India.
Prophylactic platelet transfusion can result in numerous risks, such as allo-immunisation, platelet refractoriness, allergic reactions, febrile non-haemolytic reactions, bacterial sepsis, and less commonly transfusion-associated acute lung injury. Hence, it should be avoided unless properly indicated. As most blood banks do not have an apheresis machine for obtaining single donor apheresis platelets, they have to depend on random donor platelets. Such transfusion (prepared from ca. 350 ml of blood) results in a very low increment and so repeated transfusions are needed, further increasing the risks. The cost factor is also significant as a single bag costs ca. US$270, whereas an IPF test is only $6.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.