
Abstract
There is lack of data on the contrast-enhanced endoscopic ultrasound features of tubercular lymph node; our retrospective analysis of 37 patients with enlarged mediastinal and abdominal lymph nodes showed heterogeneous enhancement in the great majority (70%).
Introduction
Contrast-enhanced endoscopic ultrasound (CE-EUS) is an enhanced imaging modality with evolving diagnostic and therapeutic potential. 1 It combines high-resolution EUS imaging of internal organs with the administration of intravenous ultrasound contrast agents. 2 This contributes information on the vascular pattern of lesions enabling differentiation of benign and malignant or inflammatory and non-inflammatory lesions. 3 The main advantage of CE-EUS is real-time imaging of micro-vascularity as well as the micro perfusion of the lesions. Moreover, the ultrasound contrast agents remain inside the blood without any interstitial extravasation and therefore they provide prolonged enhancement of the vascular system, unlike in contrast-enhanced computed tomography (CT) and magnetic resonance imaging. 4 CE-EUS has been demonstrated to have useful clinical applications in differentiating inflammatory and malignant pancreatic masses as well as lymphadenopathy. 5
Tubercular involvement of lymph nodes is common in low-income countries. 6 These nodes have a confluent or matted configuration and appear hypodense or hypo-echoic on CT and ultrasound respectively, accounting for the characteristic caseation necrosis seen on histological examination. The use of EUS in the evaluation of tubercular lymph nodes in mediastinal and abdominal locations is limited to a few studies.7–11 In an earlier study, we found patchy hypo-echoic areas and hyper-echoic foci to be significantly associated with tubercular lymph nodes. 9 We retrospectively evaluated CE-EUS features of tubercular lymph nodes compared to non-tubercular.
Patients and methods
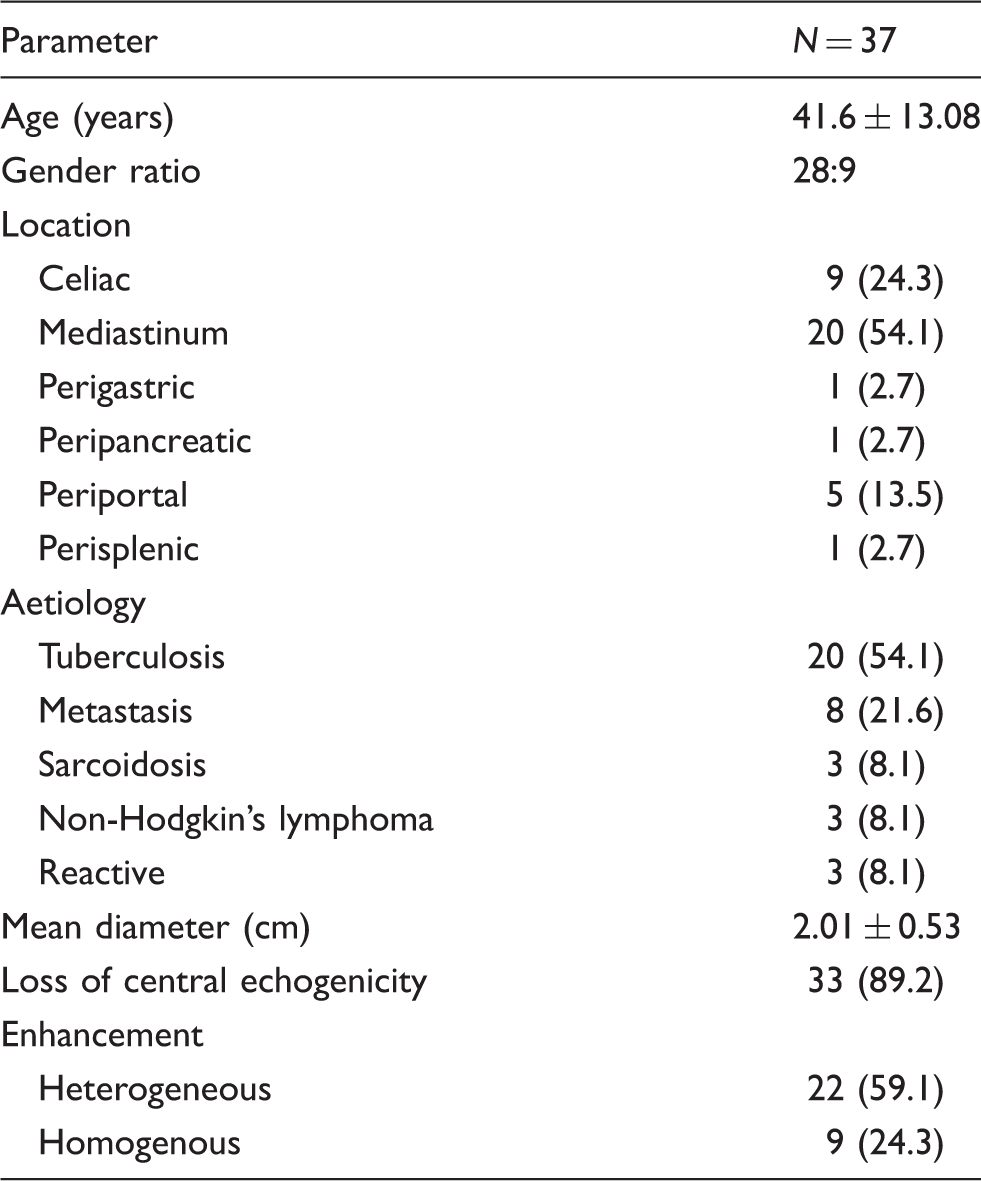
The database of 37 patients who underwent EUS followed by CE-EUS and fine needle aspirate (FNA) of mediastinal and abdominal lymph nodes between August 2018 and July 2020 were retrospectively reviewed for CE-EUS findings. Written informed consent was obtained from all the subjects prior to the EUS, CE-EUS and FNA procedures and the retrospective study protocol was approved by the institutional ethics committee ((NK/6641/Study 415 and INT/IEC/2020/SPL-1387 dated 26 October 2020). Patient demographics, clinical features, imaging findings and EUS as well as CE-EUS findings were retrieved from the database. The final diagnosis was based on the combination of clinical features, cytological and microbiological evaluation of the FNA material and clinico-radiological responses to treatment at six months’ follow-up.
Tubercular lymphadenopathy was diagnosed where clinical and radiological features combined with the presence of acid-fast bacilli on Ziehl–Neelsen staining on smear microscopy or isolation of Mycobacterium tuberculosis on culture or its detection on polymerase chain reaction. Caseating necrosis responding to anti-tubercular therapy was included in the definition.
Tuberculosis was diagnosed in 20 patients, while the remaining 17 patients had a non-tubercular aetiology of which eight had evidence of metastatic malignancy and three each had sarcoidosis, non-Hodgkin’s lymphoma (NHL) and reactive changes. Subjects were divided into groups: tubercular and non-tubercular lymphadenopathy and a comparative analysis of demographic, clinical and CE-EUS features were carried out between the two groups.
All procedures were performed by a single experienced endosonographer (SSR). A linear scanning echo endoscope (EG-3870 UTK linear echoendoscope, Pentax Inc, Tokyo, Japan or UCT180 linear echoendoscope, Olympus Optical Co. Ltd., Tokyo, Japan) at 7.5 MHz was used. A detailed EUS examination was performed and the size, number, location, and echo features of lymph nodes were noted. The location was described based on anatomical distribution in mediastinal, coeliac, peripancreatic, periportal or perigastric regions. When multiple nodes were present or represented as a conglomerate mass, the dimension of the largest node was noted as the size. Echogenicity was identified as hypo-, hyper- or an-echoic. Thereafter, CE-EUS was performed after intra-venous injection of 2.4 ml of Sonovue (Bracco, Milan, Italy) microbubble contrast followed by a 10 ml push of normal saline and using a low mechanical index (0.1–0.3). The images were recorded for at least 90 s from the time of the injection.
The appearance of lymph nodes after contrast injection was categorised as homogeneous, and heterogeneous enhancement depending on uniformity of uptake of contrast.
After completing CE-EUS examination, all patients underwent EUS-guided FNA or fine needle biopsy using a 22 G or 25 G needle (Echo Tip, Wilson Cook, NC, USA or Acquire™, Boston Scientific Corporation, Natick, MA) to obtain samples for cytology, cell block or histology.
All data were analysed on Statistical Package for the Social Sciences 22 (IBM, New York, USA). Continuous data were expressed as mean with standard deviation and categorical data were expressed as percentages. Comparison of categorical data was analysed using chi-square test or Fischer exact test (if expected number was <5), while numerical data were compared using independent-t test. A P-value <0.05 was considered to be statistically significant.
Results
Baseline characteristics and CE-EUS features.
Tubercular vs. non-tubercular lymphadenopathy
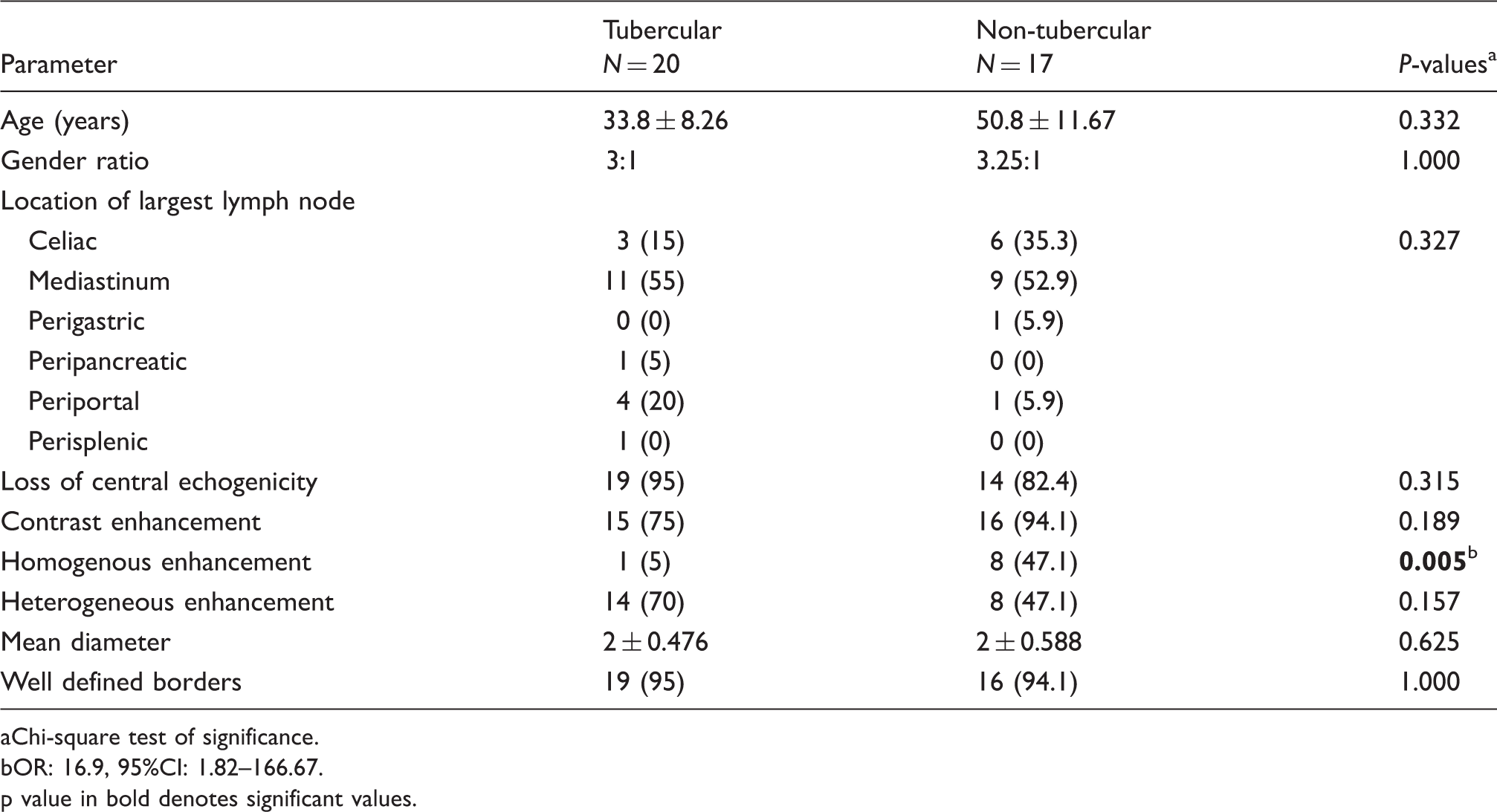
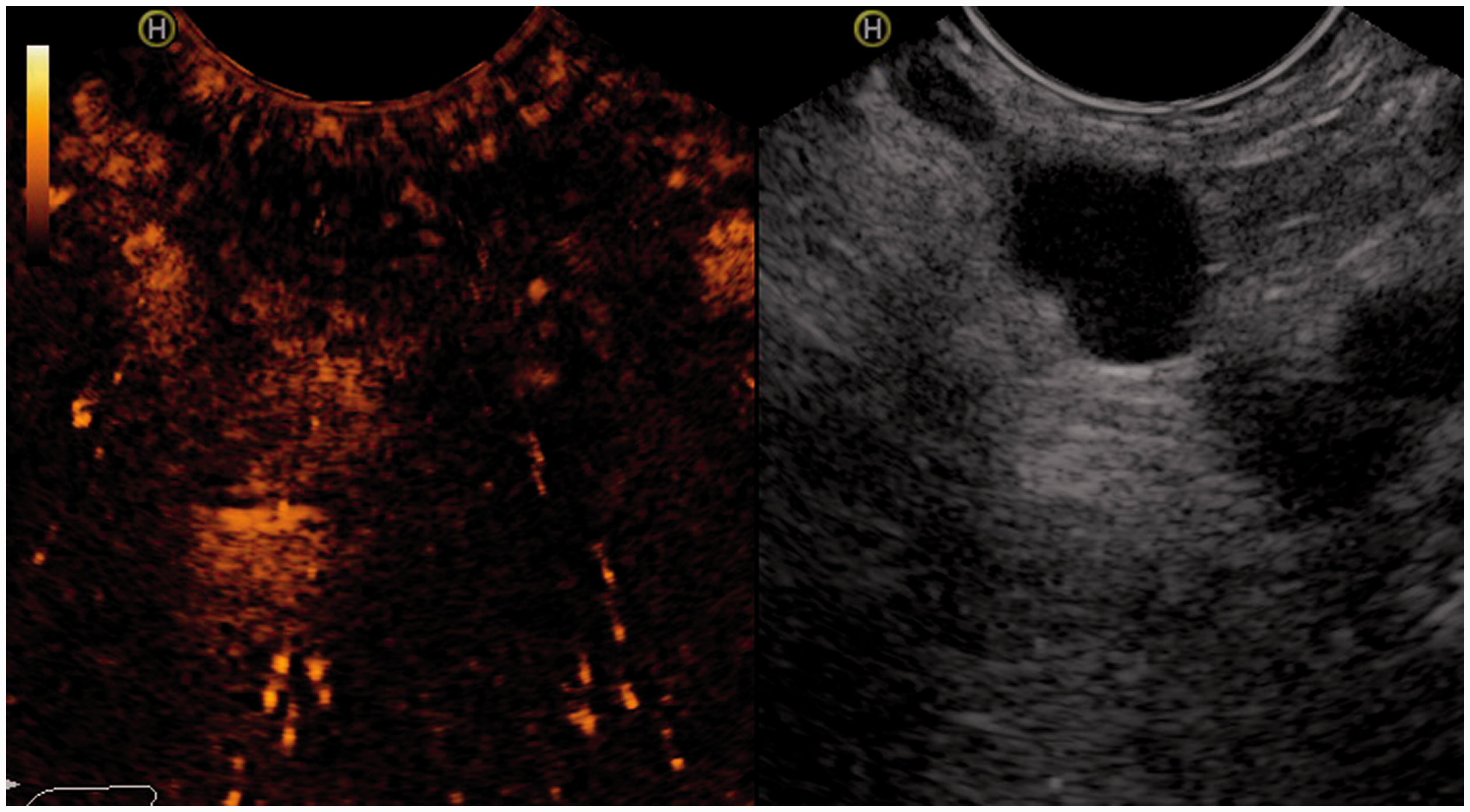
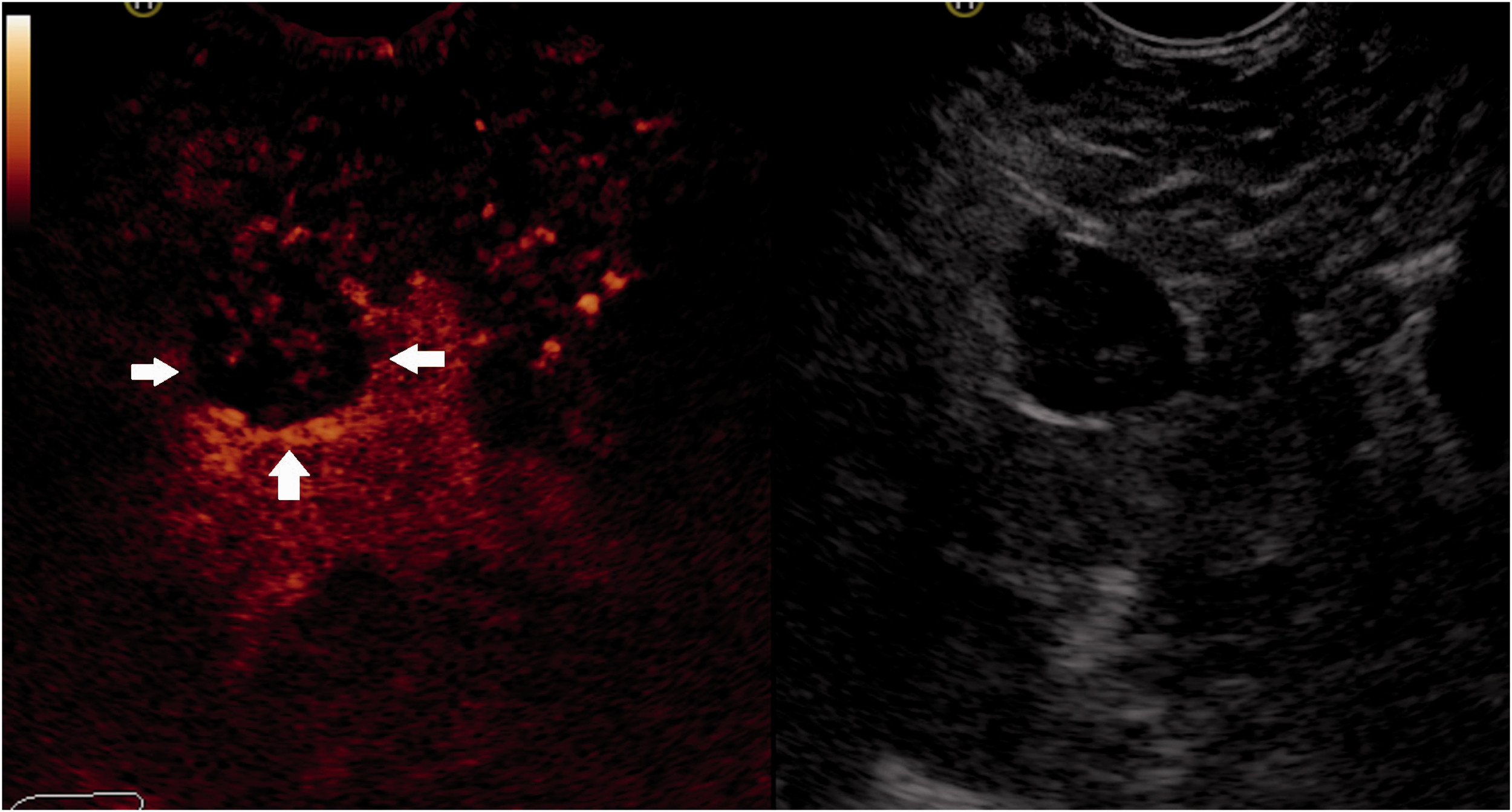
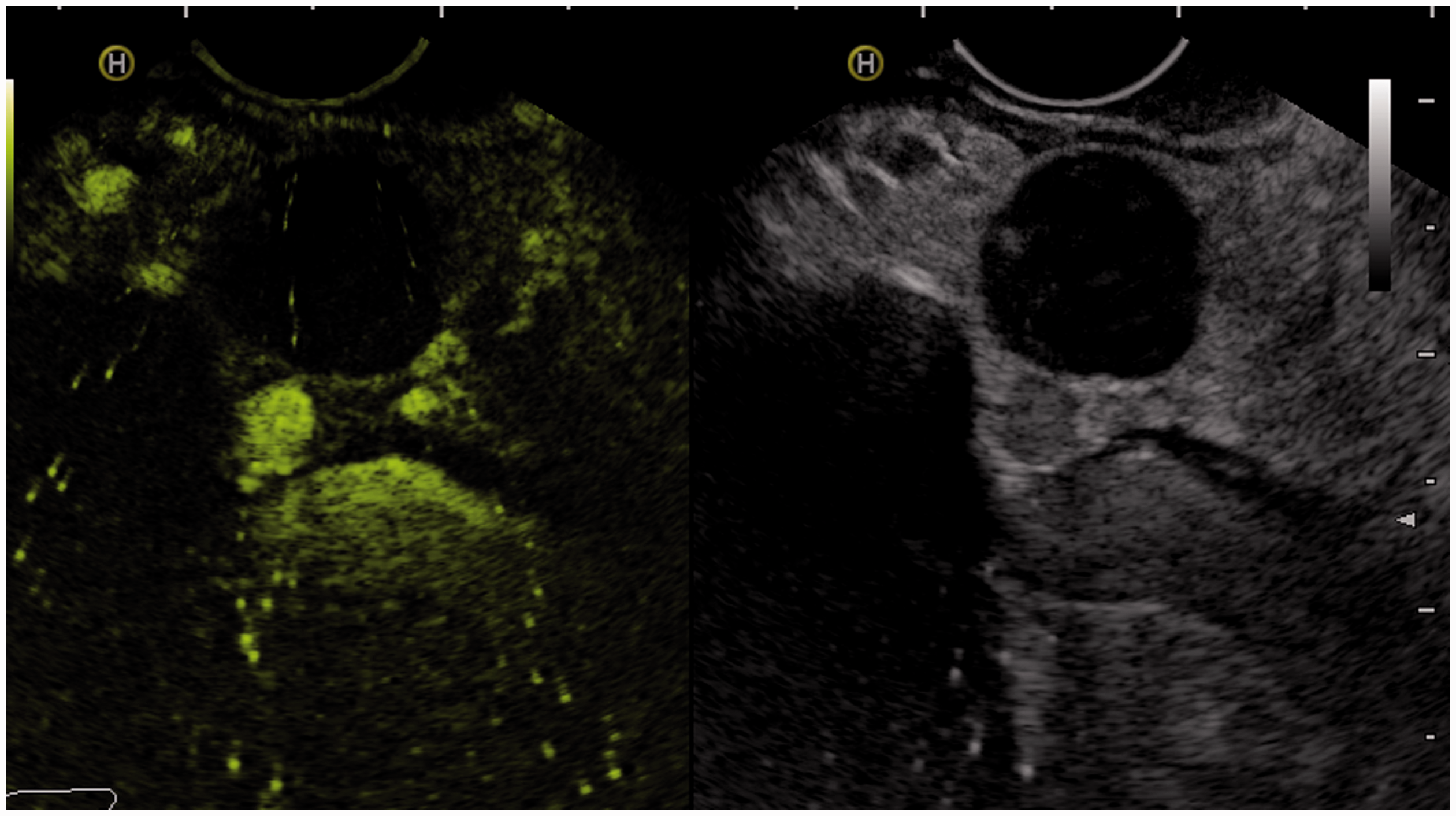
No significant difference was noted with respect to the location of involvement in the two groups (Figures 1–5). On EUS, the tubercular lymph nodes were well defined in 19 (95%) patients, all with loss of central echogenicity but these features were not significantly different from EUS features in non-tubercular lymph nodes. On CE-EUS, however, tubercular lymph nodes had 15 (75%) patients showing enhancement on contrast injection, which was heterogeneous in 14 (70%). White cheesy caseous material was aspirated in five patients with non-enhancing lymphadenopathy. On the other hand, 94% in the non-tubercular group had contrast-enhancing lymphadenopathy with 50% each having homogenous and heterogeneous enhancement respectively. A significantly higher number of patients with non-tubercular lymphadenopathy had homogenous contrast enhancement in comparison to the tubercular nodes (P-value: 0.005, OR: 16.9, 95%CI: 1.82–166.67) (Table 2). All patients with reactive lymphadenopathy as well as sarcoidosis showed a homogeneous enhancement pattern. However, there was no significant difference in the CE-EUS features between tubercular and malignant lymph nodes.
CE-EUS: Reactive lymph node demonstrating homogeneous enhancement of the lymph node (arrows). Comparison of tubercular and non-tubercular lymphadenopathy. Chi-square test of significance. OR: 16.9, 95%CI: 1.82–166.67. p value in bold denotes significant values.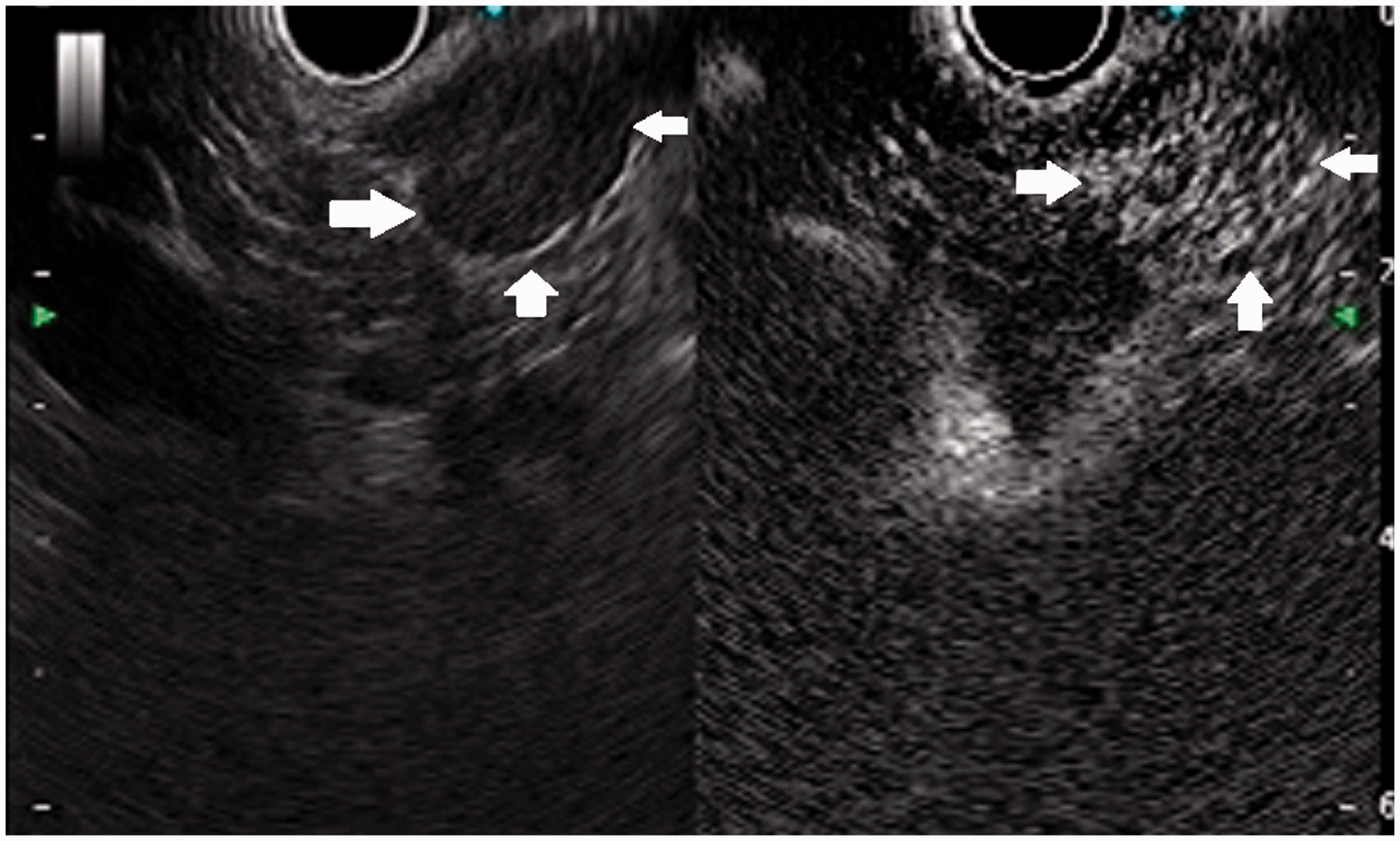
Discussion
Tuberculosis is an important cause of abdominal and extra-abdominal lymphadenopathy in low-income countries. Up to 45–50% patients with abdominal tuberculosis may have imaging evidence of lymphadenopathy. 12 CT and Ultrasound have low specificity in identifying tubercular lymph nodes. Hypodense nodes, although characteristic are not pathognomic of tuberculosis; calcified nodes may also be seen in lymphomas and metastases. 13 Thus, a tissue diagnosis is critical for accurate diagnosis.
Lymph node enlargement seen in inflammatory conditions such as tuberculosis is characterised by a necrotic centre with fibrosis and calcification. The pathognomic histological pattern of necrosis seen in active tuberculosis is of the caseation type. 14 Malignant lymph node enlargement as seen in metastasis or lymphoma is characterised by replacement of the entire nodal architecture by infiltrating tumour cells. Thus, as seen in our study, loss of nodal echogenicity on EUS is a feature common to both tubercular as well as malignant nodes. 15 Likewise, enhancement on contrast injection, which is a surrogate of vascular supply that is increased in benign inflammatory as well as malignant lesions, 16 was equally present in both tubercular and non-tubercular nodes. However, tubercular nodes showed a heterogeneous pattern of enhancement owing to the heterogeneity in the underlying pathology of the nodes ranging from necrosis to calcification depending on the duration of the disease that was radiologically reflected as a non-homogeneous or heterogeneous enhancement pattern. 17 On the other hand, non-tubercular nodes that were predominantly non-necrotic showed a homogenous contrast enhancement owing to their increased vascularity with a relative lack of necrosis, haemorrhage or calcification.
We found that a homogenous pattern of enhancement on CE-EUS is more likely to reflect a non-tubercular pathology. Therefore, this feature could give a negative predictive value in excluding tuberculosis as an aetiology of lymphadenopathy. Although, tissue sampling and histological examination is the gold standard for establishing the diagnosis, contrast enhancement pattern may give a useful clue to the probable nature of the underlying pathology.
The major limitation of our study is its small sample size and retrospective design. Procedures were all performed by a single expert endosonologist, but who was not blinded to clinical information. Despite this, we believe ours to be one of the first studies to report the CE-EUS findings of tubercular lymph nodes, emphasising their generally heterogeneous enhancement pattern. A larger prospective study should help to validate our findings.
CE-EUS: Tubercular lymph node having heterogeneous contrast enhancement. CE-EUS: Lymph node in patient with non-Hodgkin lymphoma having heterogeneous contrast enhancement. CE-EUS: Malignant lymph node having heterogeneous contrast enhancement. CE-EUS: Non-enhancing tubercular lymph node.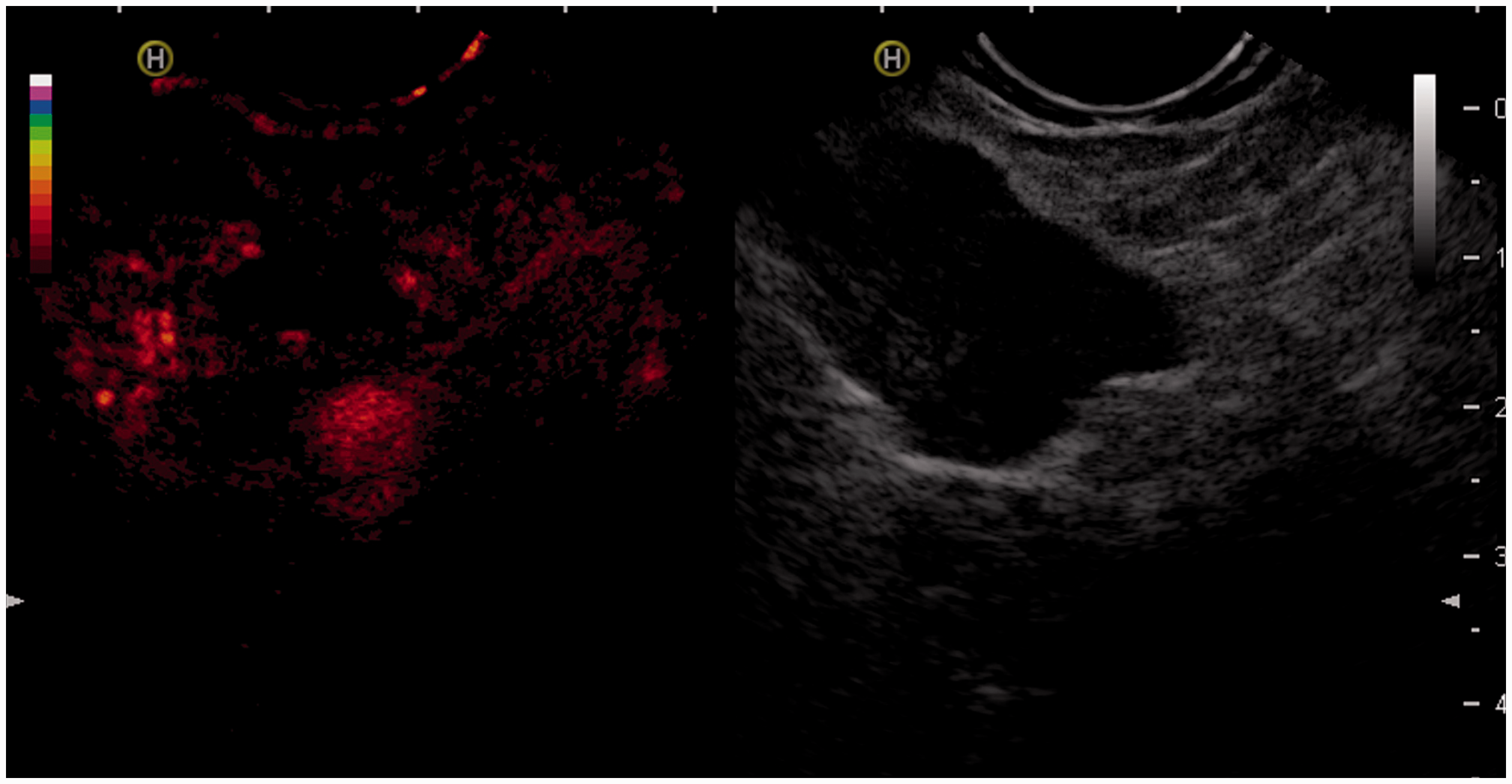
Footnotes
Author contributions
Surinder S Rana: Collection and interpretation of data, drafting of manuscript, design of study. Nikhil Bush: Collection and interpretation of data, drafting of manuscript. Saurabh Dawra: Drafting of manuscript. Ravi Sharma: Collection and interpretation of data. Radhika Srinivasan: Collection and interpretation of data. Rajesh Gupta: Collection and interpretation of data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.