
Abstract
We present three unusual cases of atypical scrotal lesions in children. The first was a firm left scrotal mass with the testis indistinguishable. The second with apparently a large hydrocoele, which was a cyst, and the third with multiple nodular lesions, pushing the left testis into the right hemiscrotum. These turned out to be a pigmented neuroectodermal tumour, a lymphatic malformation and neurofibromas respectively. Paediatric surgeons should be aware of such surgical surprises.
Introduction
The scrotum is often left unexamined, but inspection and palpation play major roles in the clinical diagnosis of scrotal masses. Inguinoscrotal hernias and hydrocoele are the most common indications for surgical visits in children. Ultrasonography may supplement clinical examination to confirm a diagnosis.
Case reports
Case 1
A one-year-old boy presented with a left scrotal mass. This was, on examination, firm in consistency with no distinct testis palpable. Ultrasound scan revealed an irregular heterogeneous mass with a small area of normal testis at the upper pole. The serum alpha fetoprotein (AFP) level was 3.7 µg/L. Abdominal and pelvis ultrasound scan were normal.
A high inguinal left orchidectomy was performed. Histopathological examination revealed nests of round cells separated by thick fibrous septae. Pigmented cells were seen at the periphery of the tumour nests and within septae (Figure 1(a)). Figure 1(b) shows pigmented cells with immunopositivity for cytokeratin. A pigmented neuroectodermal tumour of infancy was diagnosed.
(a) HPE picture showing pigmented cells at periphery of tumour nests and within septae. (b) Pigmented cells with immunopositivity for cytokeratin.
At 2.5 years, there was no local recurrence.
Case 2
An 11-year old boy presented with a right scrotal swelling since birth. He had been seen at three years, but was advised a wait-and-see approach. The swelling had gradually increased in size, with a sudden increase since one week. There was no history of trauma or fever but the swelling was associated with a dull ache since then. On examination, the right scrotum was enlarged but genitalia was normal (Figure 2(a)). The swelling partially transilluminated and the testis could be palpated. A clinical diagnosis of a large hydrocele was made; on exploration, a large cyst partly haemorrhagic was found (Figure 2(b)). The lesion was excised; it was found to be lymphatic malformation. At four years’ follow-up, he was asymptomatic.
(a) Clinical picture of right hydrocele. (b) Intra-operative picture showing cystic spaces partly filled with old blood.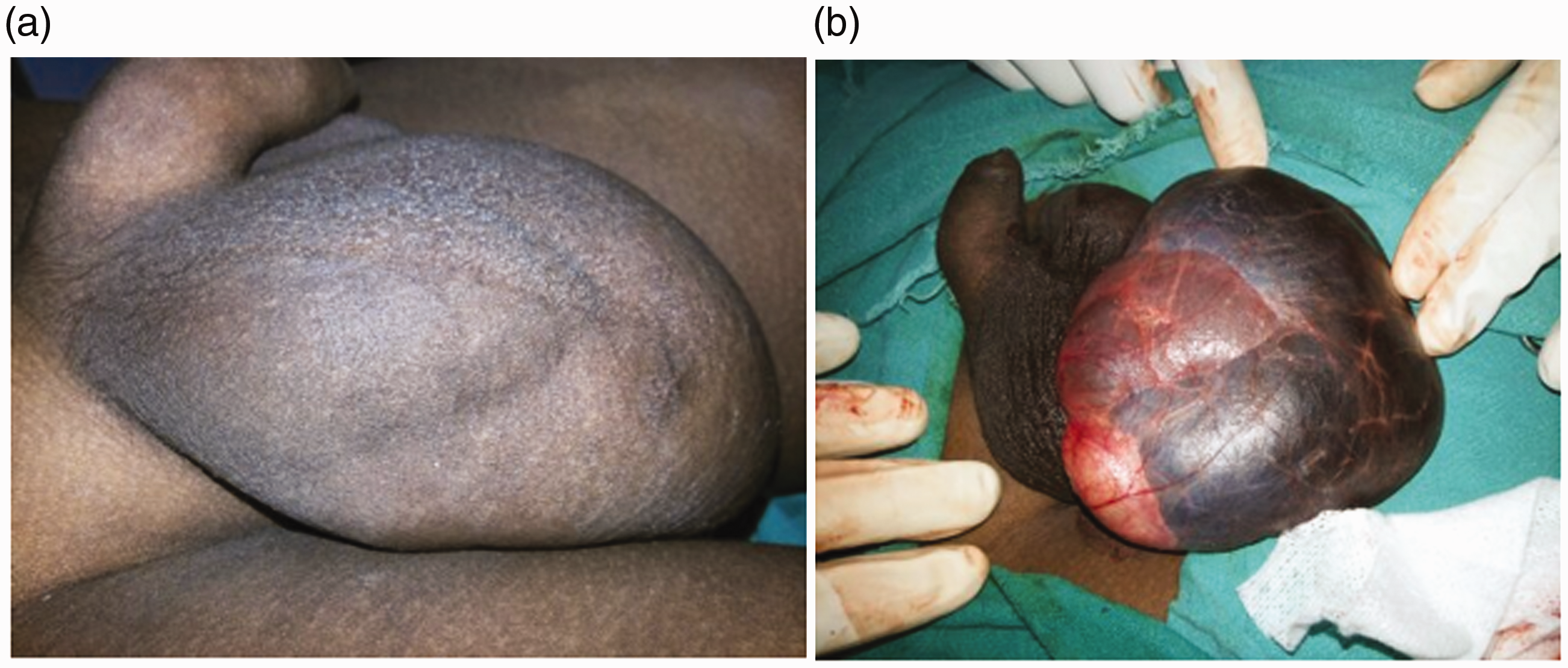
Case 3
An eight-year-old boy presented with multiple nodular lesions in the left scrotum, pushing the left testis into the right hemiscrotum (Figure 3(a)). Fine needle aspiration cytology was attempted but was inconclusive. Scrotal exploration revealed multiple round nodules of variable sizes (Figure 3(b)), which were neurofibromata.
(a) Clinical picture of scrotum showing multiple nodular lesions in left scrotum, pushing left testis to right hemiscrotum. (b) Picture of excised multiple round nodules of variable sizes.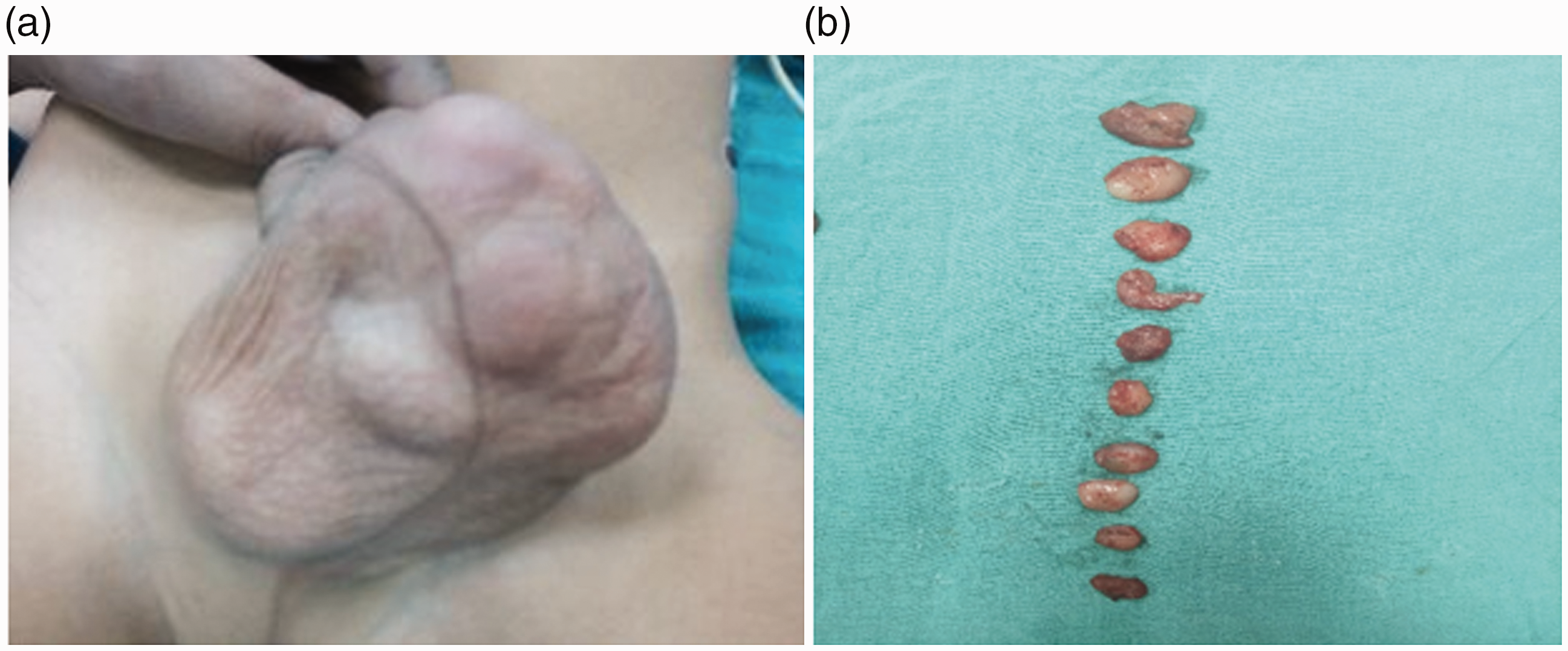
Discussion
Scrotal masses in children are quite common. They may be testicular or extra testicular; solid or cystic. Malignancy is rare. Solid testicular masses are malignant in 90–95% of cases, while extra-testicular masses are mostly benign and majority are cystic.
Most cases of pigmented neuroectodermal tumour of infancy occur in the first year of life, with most common sites being the maxilla, skull and brain. It has a variety of names including melanotic neuroectodermal tumour of infancy, melanotic progonoma, retinal anlage tumour, retinoblastic teratoma, and melanotichamartoma. It is of neural crest origin affecting males and females equally. A biphasic morphology is usually present, as in our case. The two cell lineage includes round cells with hyperchromatic nuclei and scant cytoplasm and melanin-containing cuboidal epithelioid cells. Immunohistochemistry shows round cells positivity for Neuron Specific Enolase (NSE), CD56, synaptophysin, glial fibrillary acidic protein, and S-100, as well as epithelioid cells positivity for cytokeratin, Human Melanoma Black (HMB) and Epithelial Membrane Antigen (EMA). 1 Rapid and local infiltrative growth mandates early treatment, in the form of radical surgical excision with clear margins. For testicular Pigmented Neuro Ectodermal Tumor (PNET), simple orchidectomy is curative. 2 Follow-up is recommended in view of chances of potential recurrence and rare malignant transformation. 3 Recurrence is reported from 10 days to 2 years. 4
Scrotal lymphangioma is very rare and is mostly misdiagnosed as a hydrocele, haematocele, or spermatocele.5,6 It is usually painless and has no sex or race predilection. Rarely, it may become infected or bleed secondary to trivial trauma thus causing an increase in scrotal size and acute pain. Local recurrence may occur if not completely excised.
Neurofibroma is a benign peripheral nerve sheath tumour with Schwann cell origin. Solitary scrotal neurofibroma without neurofibromatosis is rare and has a low malignant potential. 7 It may originate from tunica, epididymis, subcutaneous neural tissue, or spermatic cord. 8 The majority of scrotal neurofibromas are extra-testicular. 9 General physical examination should look for café-au-lait macules, Lisch nodules or optic gliomas to rule out associated neurofibromatosis 1 (NF 1). The treatment of choice is excision. Histology shows uniformly distributed spindle cells with no mitosis. Immunohistochemistry is positive for vimentin and S100 while negative for Smooth Muscle Actin (SMA), keratin and desmin. Prognosis is good with uncommon local recurrence in solitary scrotal neurofibromas. 10
Generally clinical examination cannot differentiate between benign and malignant nature. Ultrasound may help in locating the organ of origin, extent, echogenicity and characterisation of a lesion. It can very reliably differentiate testicular and a paratesticular mass with >95% sensitivity. 11 Poorly defined, disorganized solid masses with heterogeneity and hypervascularity are features favouring malignancy,12,13 although again wholly reliable differentiation between benign and malignant is not possible. 14
For lesions seriously suspected of malignancy, further scans and screening tests are indicated.
Conclusion
While rare, paediatric surgeons should be aware of such surgical surprises, in order not to compromise on their correct treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Parveen Kumar https://orcid.org/0000-0001-5835-4053 Mamta Sengar ![]()