
Abstract
Enteric fever, an endemic disease, is a significant health problem in developing low- and middle-income countries (LMICs). We studied the utility of Typhoid IgM/IgG assay in Widal titre positive samples among malaria negative patients. A total of 30 febrile patients were included. A blood sample was collected for performing the Widal test and a rapid lateral flow immune assay (Typhoid IgG/IgM tests). A total of 13/30 were positive on blood culture; however, Salmonella typhi grew on only two (6.6%). Of the 30 samples, 24 (80%) were positive for the rapid immunochromatographic (ICT) test None of the samples negative by the rapid ICT test grew Salmonella typhi. The rapid ICT test has better sensitivity and is easy to perform with minimal infrastructure; hence, it is a practical alternative to the age old Widal test
Introduction
Enteric fever, an endemic disease, is a significant health problem in LMIC. Global estimates suggest approximately 11−21 million cases and 1,28,000 to 1,61,000 deaths annually. 1 Typhoid fever, caused by Salmonella enterica serotype typhi, produces high morbidity and mortality across the globe. 2 Signs and symptoms, being nonspecific, demand an accurate diagnosis for timely treatment as appropriate antibiotics are required for recovery, prevention of complications and also to control transmission. 3 The isolation of the organism from blood or bone marrow is time consuming, although still recommended for confirmation. 4 Malaria and typhoid fever, caused by two different organisms and transmitted differently, are common problems in tropical countries; often occurring concurrently, with a considerable overlap of clinical signs and symptoms.5,6
Accurate and appropriate laboratory diagnosis is essential. 7 Culture from various samples and several serological tests help to diagnose enteric fever in different stages; blood culture is usually considered the gold standard and becomes positive in the first week of fever. 8 Some of the serological techniques such as chromatographic immunoassay and tube agglutination tests are quick and simple to perform. 9 Although blood culture is the gold standard, only 30 - 40% tests are positive as most patients have already been treated with antibiotics by the time their samples are collected for culture. 4 Basic laboratory equipment for blood culture and technical training for its evaluation are beyond the means of many peripheral diagnostic facilities.4,7 Furthermore, this process takes 2 - 3 days, which is too long before treatment needs to be initiated; thus clinicians usually tend to rely upon rapid antigen based methods like Widal and the typhoid IgG/IgM rapid test for the diagnosis.7,10,11 The Widal test, used commonly, has only moderate sensitivity and specificity, and its interpretation is difficult in the light of cross-reacting circulating antibodies. False positive and false negative results are common in areas of high endemicity. Molecular tests, being complex and expensive, are difficult to apply in routine use.3,4 Thus serological tests, which are rapid, inexpensive, reliable, and easy to perform with high sensitivity & specificity; are considered the most appropriate in out-patient settings.10,12 The rapid immunochromatographic test is a lateral flow immunoassay for qualitative detection of IgG and IgM antibodies against Salmonella typhi (S.typhi) and paratyphi. It can be used as a screening test and can be visually interpreted within 1h. 8 Typhoid assay detects IgM for recent infection and IgG for late phase of infection.
Materials and methods
Our prospective descriptive study was carried on in the Immunology laboratory of the Microbiology Department at a tertiary care hospital in, East Delhi. 30 febrile patients, diagnosed malaria negative and Widal positive were included irrespective of gender, age or any other underlying diseased condition.
The Widal tube agglutination test was carried out on all the sera using commercial available antigen suspension (Span diagnostic kit) for the somatic O and flagellar H antigens. Titrers were correlated clinically according to existing baseline values.
The typhoid IgG/IgM Test (Typhoid IgG/IgM test device, Medsores Ozone Biomedicals Private Limited, Faridabad, India) is a lateral flow chromatographic immune-assay.
Bacteriological blood culture was carried out using 8 - 10 ml of peripheral venous blood. After incubation of 37°C for 24 h, all blood cultures were subcultured on MacConkey agar after 24 h, 72 h and on the 5th day. The colonies of S.typhi S.Paratyphi A and B were identified according to standard protocol.
All laboratory parameters were analyzed by using the statistical package for social sciences (SPSS) version 21. The sensitivity, specificity, PPV & NPV for Typhidot were calculated with culture for Salmonella as the gold standard.
A total of 30 Widal positive but malaria negative patients were enrolled to assess the utility of rapid ICT test in use and compare with the blood culture and Widal test.
Results
Female patients were in the majority (74%). The age of the study population ranged from 2–60 years, with approximately one third in the 15-30 years ranges and their mean age being 25.5 years.
Out of these 30 samples, 13 (43%) were positive for the growth of any organism and the remaining 17 (57%) were negative for any bacterial growth. Out of these 13 positive blood culture samples, only 2 (6.6%) had growth of Salmonella typhi. The distribution of Widal positive samples are depicted in Figure 1.
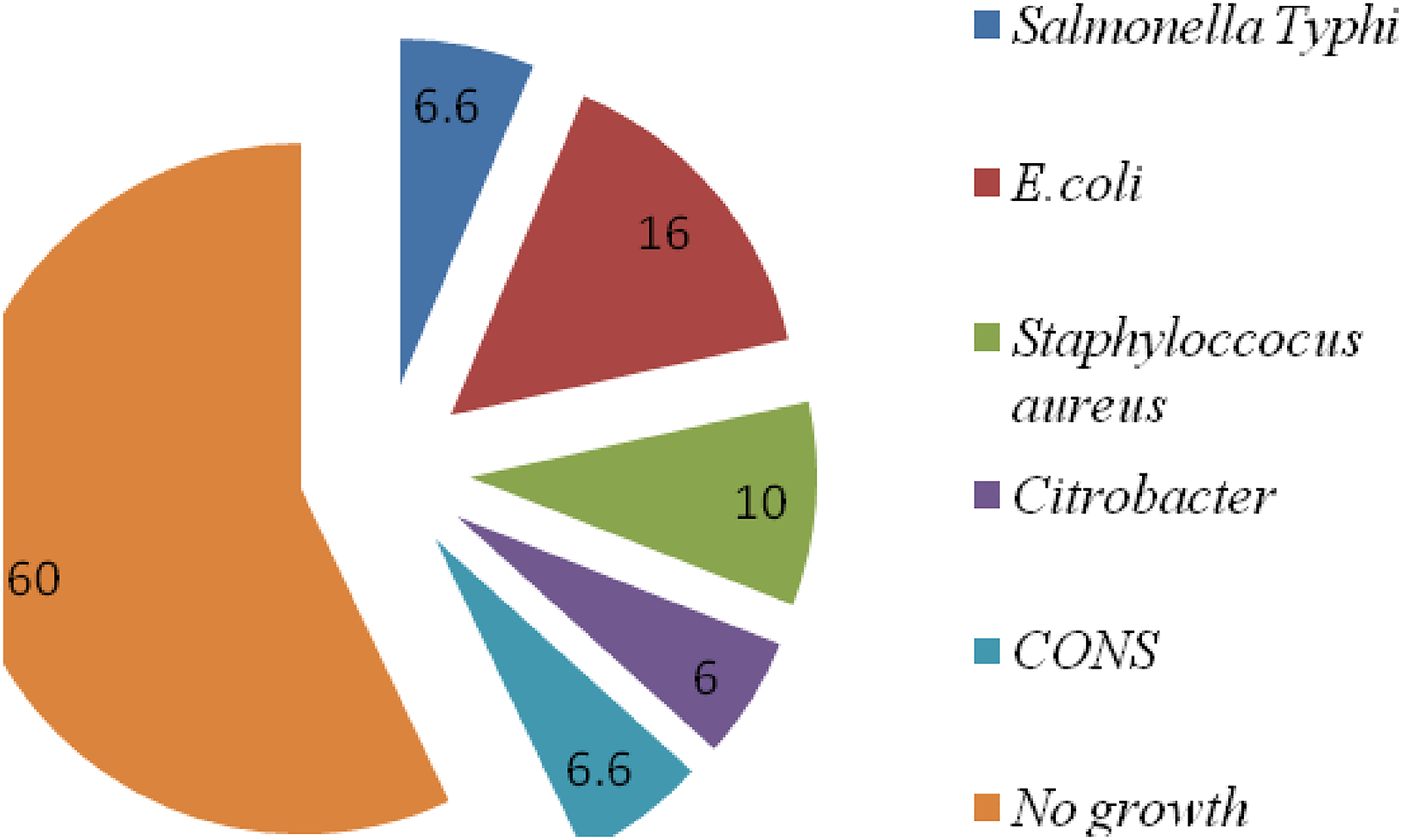
Frequency distribution of organisms isolated in blood culture. (n = 30).
The results of Widal and Typhoid IgG/IgM test among blood culture positive samples are depictied in Table 1.
Widal and typhoid IgG/IgM test among the blood culture positive samples. (n = 30).
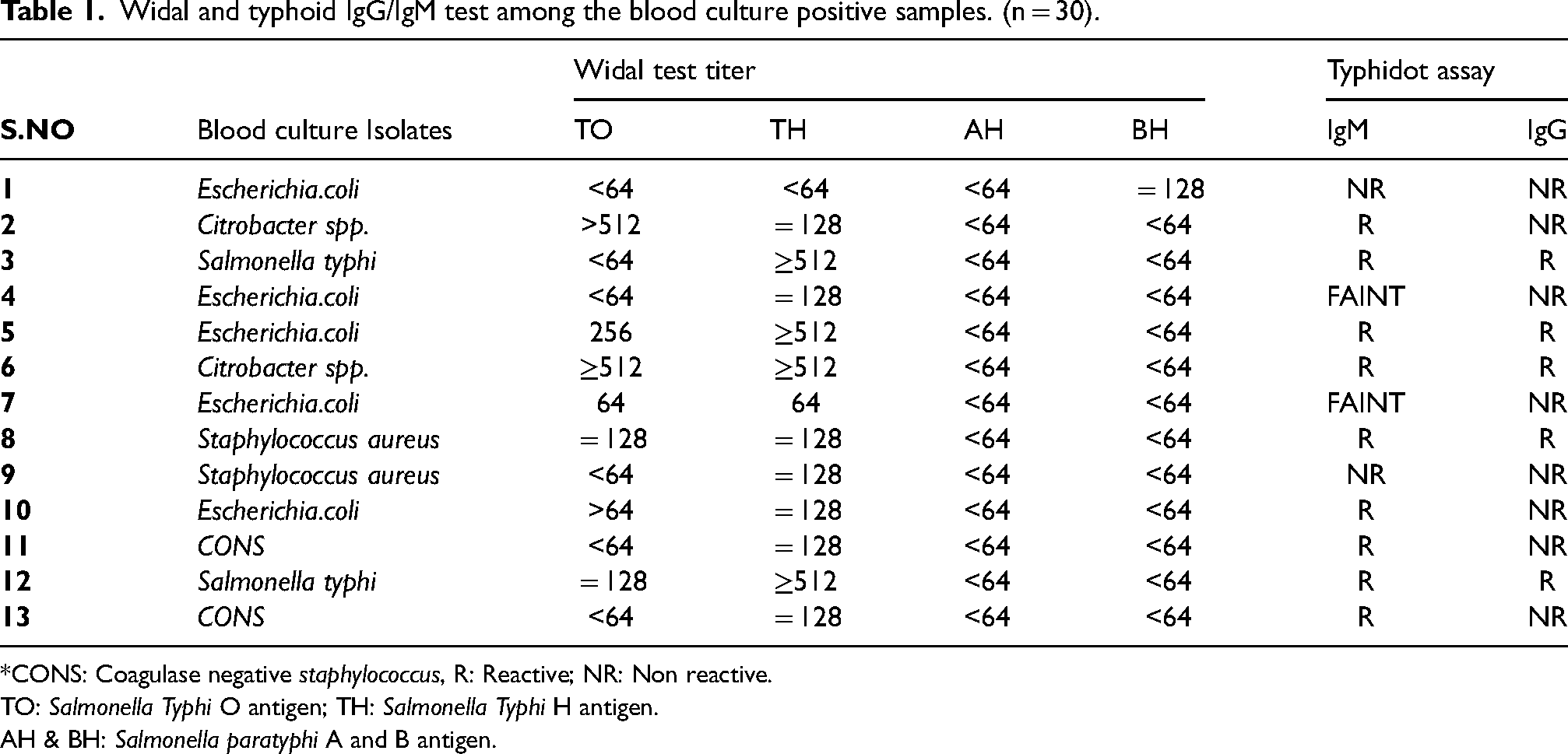
*CONS: Coagulase negative staphylococcus, R: Reactive; NR: Non reactive.
TO: Salmonella Typhi O antigen; TH: Salmonella Typhi H antigen.
AH & BH: Salmonella paratyphi A and B antigen.
Out of 30 samples in the present study, 24 (80%) were positive while, 6 (20%) were negative for the rapid ICT test. None of the rapid ICT test negative patients grew Salmonella typhi. The results of Widal test and blood culture among rapid ICT test negative and positive samples are shown in Tables 2, 3 & 4 respectively.
Widal and blood culture positivity in typhoid IgG/IgM test negative study population (n = 6).

TO: Salmonella typhi O antigen; TH: Salmonella typhi H antigen.
AH & BH: Salmonella paratyphi A and B antigen.
Widal and blood culture in typhoid IgG/IgM test positive samples among study population. (n = 24)
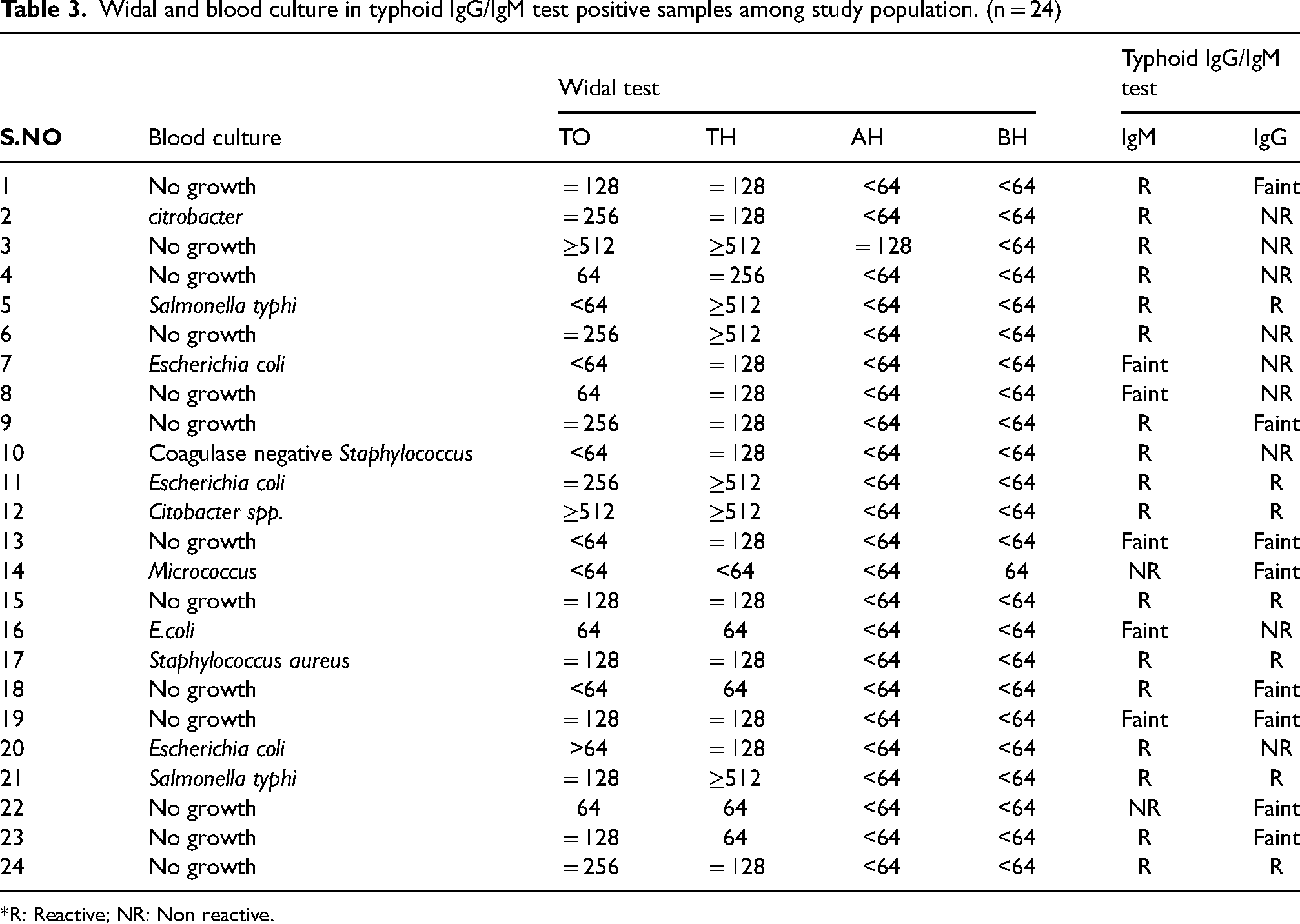
*R: Reactive; NR: Non reactive.
Sensitivity, specificity, PPV & NPV of typhidot with culture as gold standard.
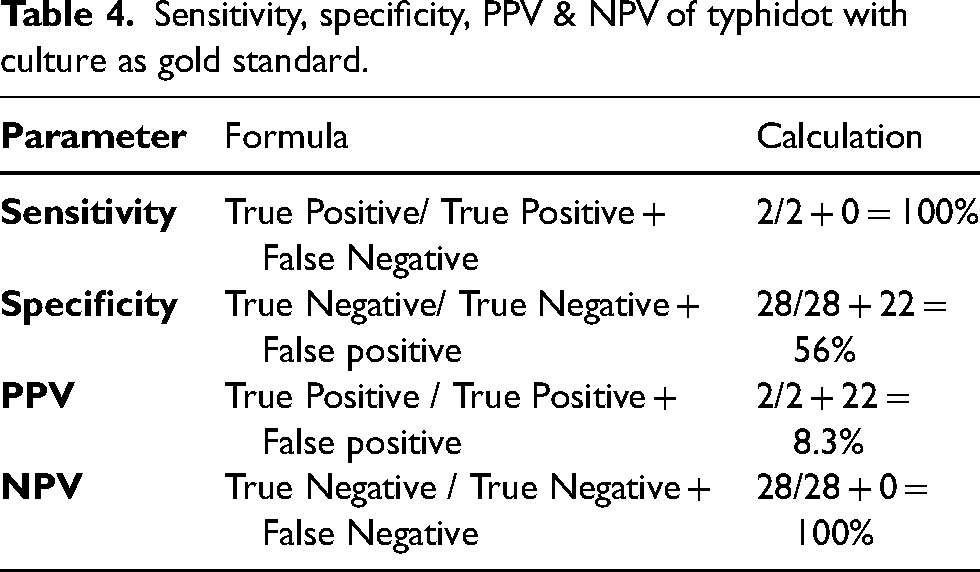
Samples from two patients had Salmonella typhi in blood culture, both of whose Widal test showed titer of Salmonella typhi for H antigen ≥ 512 and TO < 64 and = 128 respectively, whereas the paratyphi A and B, AH and BH antigen titres in both were <64. Typhoid IgM antibody for these two patients was reactive, while the presence of IgG antibodies in these patients showed faint lines. As regards the other patients, the Typhoid IgM antibody were positive in 17 (70%) while IgG antibody was positive in 2 patients (8.3%). 5 patients (20.8%) showed a faint line for the presence of IgM antibody, while 10 patients (41.6%) had a faint line for IgG antibody. Samples from another 2 (8.3%) showed faint lines for both IgM and IgG antibodies, though the intensity of the test band does not have any linear correlation with the antibody titre in the specimen and this test is limited to the qualitative detection of antibodies to S. typhi or paratyphi. With culture for Salmonella as the gold standard; the sensitivity, specificity, PPV & NPV of Typhidot were 100%, 56%, 8.3% and 100% respectively (Table 4).
Discussion
Enteric fever is an endemic health problem in low-and middle income countries. Non-specific presentations requires differentiation from other common febrile illnesses. Poor socioeconomic conditions and lack of proper medical care or facilities further prompt the spread of the disease. 13
No test for enteric fever is 100% sensitive or ideal. Blood culture is the gold standard, although a conclusive report takes some time. So, taking just one sample for blood culture has an approximate sensitivity of 60%. 14 It is not uncommon to find patients receiving simultaneously empirical treatment for typhoid and malaria; moreover many medical practitioners rely on a single Widal test result for the diagnosis of typhoid fever. 5 This not only leads to higher cost of treatment owing to unnecessary expenditure, but also exposes the patient to many consequences of antibiotic misuse. Culture facilities, even if available, lead to inappropriate treatment owing to delays in producing test results. 14 The purity and standardization of the antigen used for the Widal test is a major problem and often results in poor specificity and poor reproducibility of tests results. It is important to realize the limitations of the Widal test and also interpret results in light of endemic titres. 15 There is a need for a quick and reliable diagnostic test for typhoid fever as an alternative to Widal test. Poor specificity may also be a consequence of pre-existing base line antibodies in endemic areas, cross reactivity with other Gram negative bacteria and non typhoidal Salmonella, anamnestic reactions in unrelated infections or prior TAB or oral typhoid vaccination.
Blood culture also has a poor positive predictive value as patients might already be in the second or third week of fever and antibiotics treatment.
Typhoid IgG/IgM is - simple, rapid, cheap and offers early diagnosis with the sensitivity and specificity of 95% and 75% respectively and high positive and negative predictive values.21 The detection of IgM antibodies suggests acute typhoid in the early phase of infection, while IgG antibodies may persist longer for years after infection. 16 A negative rapid immune-chromatographic test is virtually true negative, with a sensitivity of 92% and specificity of 83% among culture proven cases of enteric fever because of the masking affect of high IgG levels of past infection on IgM antibody. 2 Published documented Typhidot sensitivity, specificity, PPV and NPV range from 81.7 - 92.6%, 37.5 −100%, 48.7 - 100% and 88.8- 93% respectively.2,10–12
However, since blood culture is poorly sensitive, any evaluation based on blood culture as the gold standard should be interpreted with caution.
The Typhoid IgG/IgM test offers an additional advantage of minimal operator training above other conventional diagnostic test, though is relatively costly and requires cold storage facility. The results of Widal and Typhoid IgG/IgM test should still be confirmed by blood culture; sensitivity is useful especially in those settings where the organism has become resistant to antibiotics. However, for reasons stated, Widal and Typhidot results may not correlate well with blood culture, which means the latter cannot really be a gold standard; however the immunological test has significant superiority for it to supercede the Widal test 11