
Abstract
Patients experience delays in emergency surgical care. Our 3-month mixed-methods observational prospective study examined the duration of in-hospital delays (IHDs) to emergency surgery at a tertiary hospital in Malawi and perceived reasons for such delay, assessing the correlation between surgery and anesthesia. Delays over two hours occurred in the majority, and almost 20% waited over twelve hours. However, we found no correlation between surgeons and anaesthetists in the perceived reasons for In-hospital delays to emergency surgical care.
Introduction
The lack of access to safe, affordable surgical and anesthesia care impacts approximately 5 billion people worldwide. This burden is disproportionately borne by people who live in low- and middle-income countries (LMICs). 1 In the literature, access to timely essential surgery is defined as the proportion of the population that can access, within 2 h, a facility that can perform the Bellwether procedures. 1 Some surgical conditions are time-sensitive and require immediate intervention. Patients in high- and low-resource settings experience delays in emergency surgical care and thus suffer increased morbidity and mortality.2–11
There are three primary phases of delay: pre-hospital, inter-facility, and in-hospital.1, 2 Pre-hospital delay, or a delay in seeking care, can stem from financial or geographic restrictions, cultural beliefs, lack of education, historic disconnection from formal health systems, and lack of awareness or confidence in formal health structures. Inter-facility, or delay in reaching a healthcare facility with the capability of providing definitive care after initial healthcare presentation, is related to the lack of access to hospitals with surgical capacity and lack of access to reliable and affordable transportation and geographical barriers. 1 Finally, in-hospital delay (IHD) is a delay occurring after presenting to a hospital that can provide definitive care. Previous studies have identified unavailability of appropriate health care providers, hospital beds, absence or failure of equipment and essential supplies, ongoing emergency surgery, and lack of reliable electricity, running water, robust blood banks, and oxygen as common causes of delays to surgical care in low-resource settings.1, 12–17
However, few studies have prospectively compared healthcare providers’ perspectives on reasons for IHDs to emergency surgical intervention. It is imperative to understand context-specific reasons for delay to ensure that initiatives to address surgery delays are appropriate, acceptable, and attainable.
Malawi is a landlocked country in southeast Africa with limited surgical capacity and a developing surgical workforce.18, 19 As Malawi trains more surgeons, anaesthetists, clinical officers, and nurses, it is important to assess other components of the health system infrastructure critical to surgical care delivery. A previous retrospective analysis performed by the Kamuzu Central Hospital (KCH) Department of Surgery identified that over a third of patients who required emergency abdominal surgery waited more than 24 h after hospital arrival before undergoing operative intervention. 20
KCH is a tertiary hospital in Central Malawi, located in the country's capital, Lilongwe. It serves as the referral center for the region. It is a 900-bed hospital with eight operating theatres. Specialties using these theatres are general surgery, orthopedics, paediatric surgery, urology, neurosurgery, otolaryngology, and plastic surgery. Specific days are allocated to subspecialties who take turns utilizing these theatre rooms. However, depending on the type of specialty under which the emergency falls, any of the rooms can be disrupted at any given time to make way for the emergency case. There is a six-bed intensive care unit (ICU), a six-bed surgical high dependency unit (HDU), male and female surgical wards, and a four-bed casualty department. General surgery consultants, surgical registrars, junior doctors, and clinical officers provide trauma care. The general surgery service consisted of five consultant general surgeons, four surgical clinical officers, and at least three surgery registrars over the study period. Anesthesia care was provided by clinical officers assigned to individual operating theatres and the ICU during the day and two anaesthetists who were on call overnight or on weekends – one for the main operating theatre and one for the ICU.
Methods
Our study was carried out between January 24 and March 29, 2020. KCH data clerks and the study personnel (BR) collected the data. Patients met study inclusion criteria if they were ≥13 years old and presented to the emergency department with an urgent or emergency general surgical condition after assessment by a registrar or consultant surgeon. As the focus of this study was on general surgical patients, we excluded patients if they were admitted initially to the medicine service and then transferred or if the primary condition was obstetrical and gynecological, orthopaedic, or neurosurgical (Figure 1).
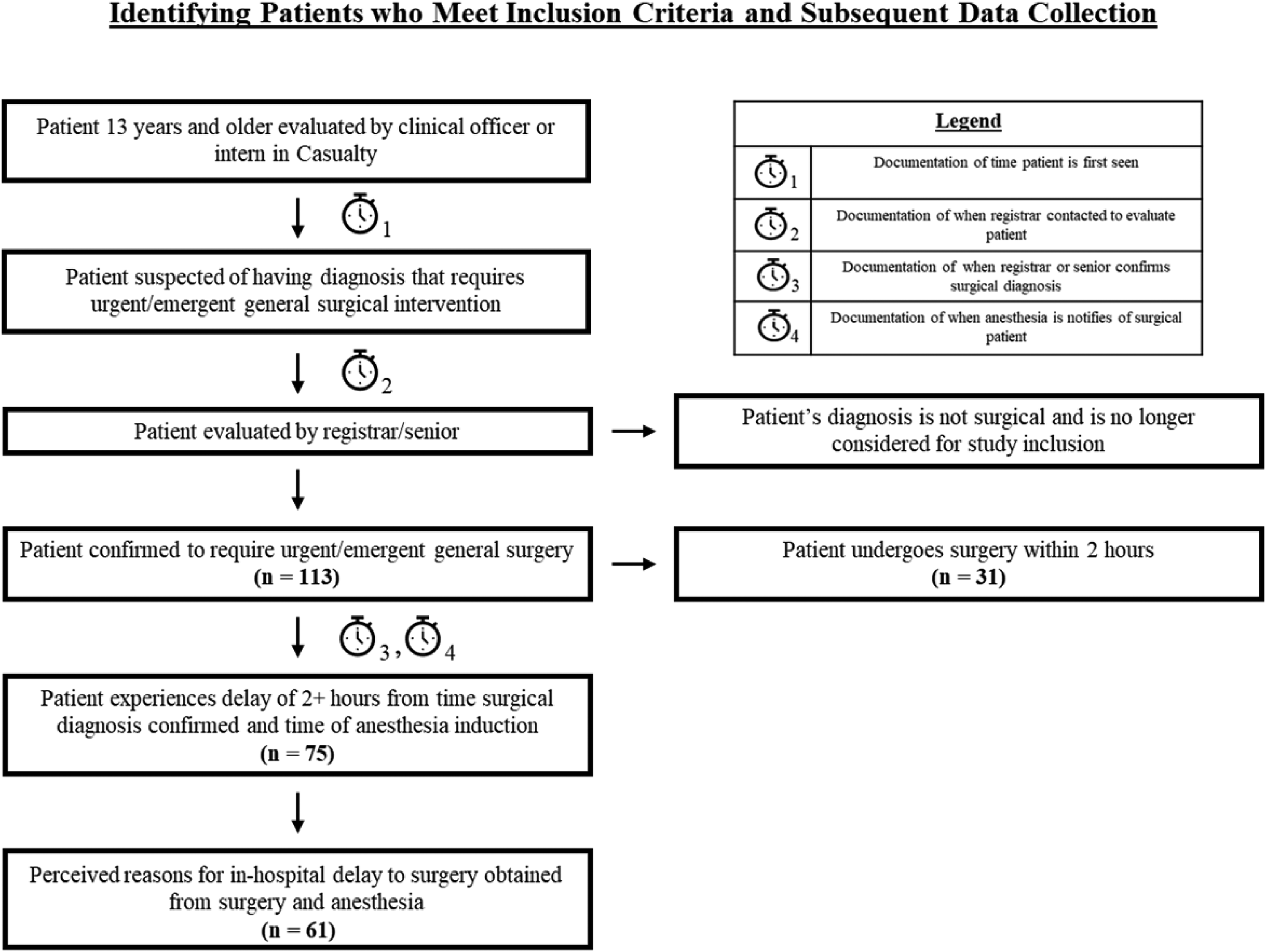
Identifying Patients who Meet Inclusion Criteria and Subsequent Data Collection.
We divided data collection into quantitative and qualitative categories. We defined IHD as the length of time >2 h from the decision to operate to anesthesia induction. A secondary outcome of interest was the perceived reason for in-hospital delays by the surgery and anesthesia teams. Quantitative data consisted of the critical time points from the patient's arrival to anesthesia induction. We prospectively collected these data through observation, chart, and operative log review by the KCH data clerks and the lead author.
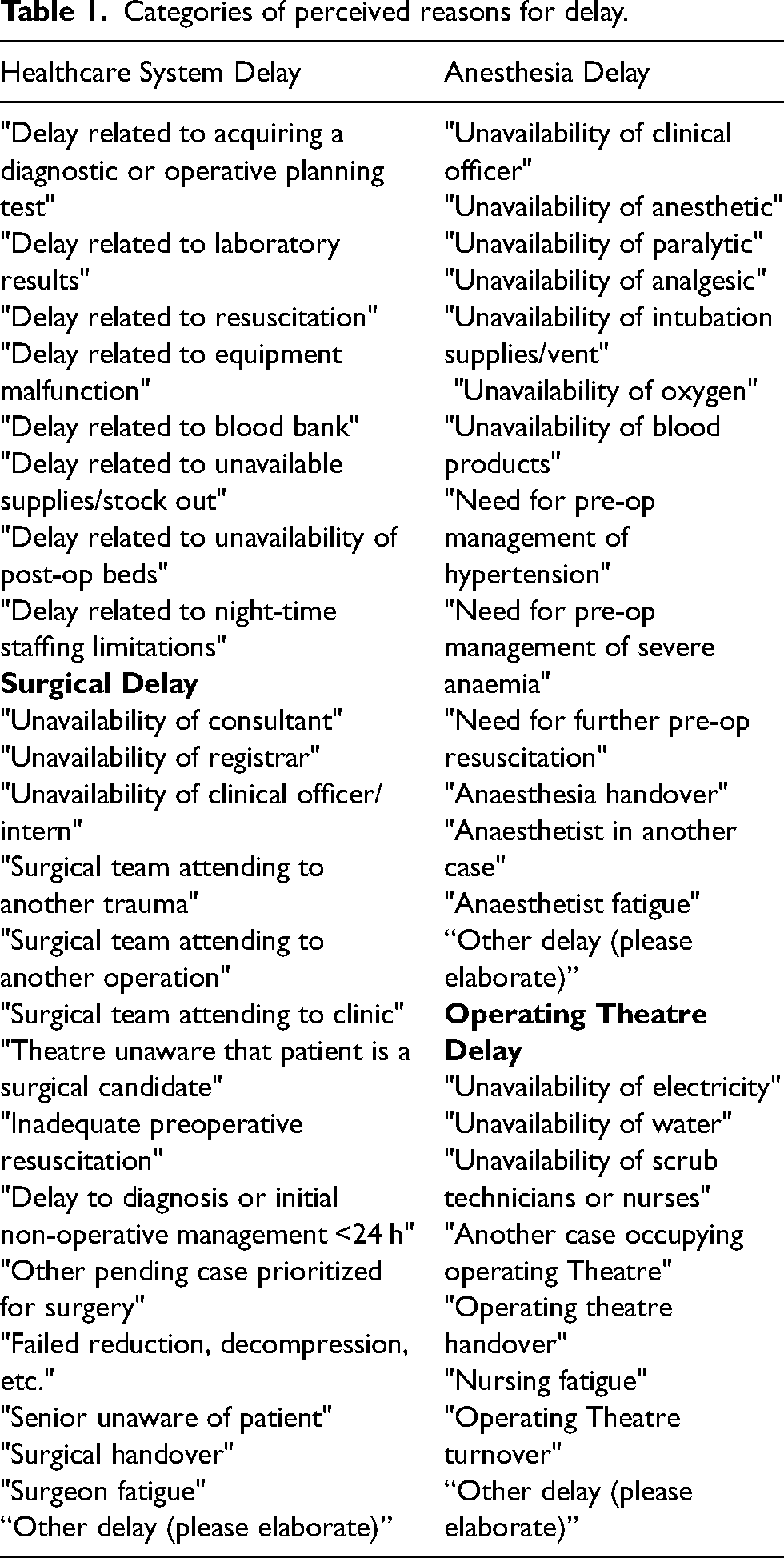
We developed a general framework of perceived reasons for in-hospital delay through informal interviews with seniors from the KCH surgical and anesthesia teams. There were four main categories – healthcare system, surgical, anesthesia, operating theatre, and 42 unique responses (Table 1). Study staff gathered qualitative data from observation of anesthesia and surgery morning reports, which occurred daily Monday to Friday, discussing weekend cases on the following Monday. We recorded perceived reasons for delay. Providers could offer more than one reason, and we included all reasons in our analysis. If not explicitly discussed in the morning report, the study staff attempted to gather the providers’ responses within 48 h of the surgical intervention. The failure to reach providers within 48 h or lack of provider ability to recall reasons for delay accounted for missing data.
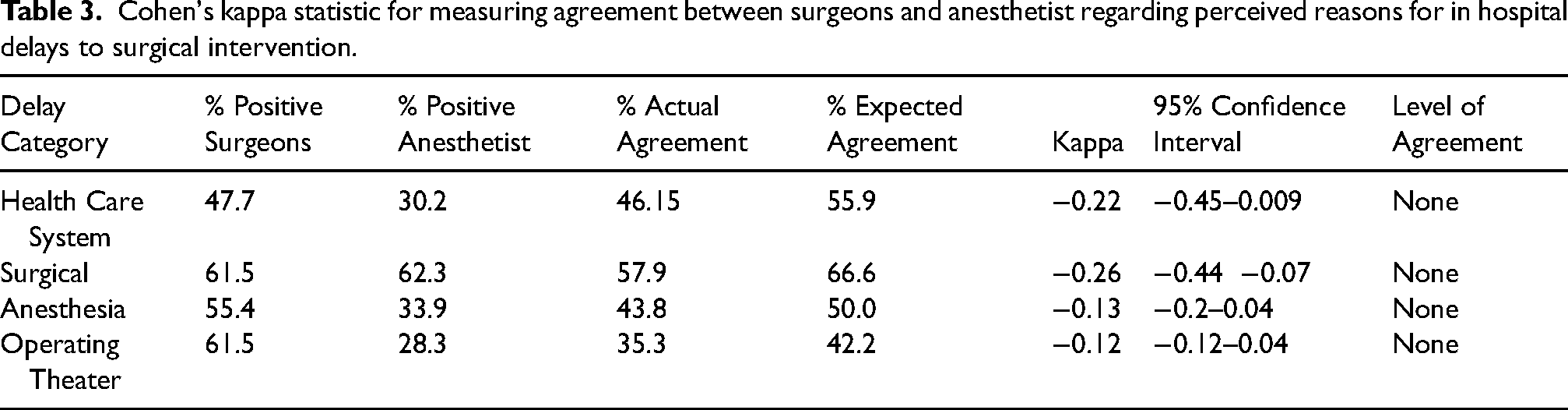
Cohen's kappa statistic for measuring agreement between surgeons and anesthetist regarding perceived reasons for in hospital delays to surgical intervention.
When evaluating patient clinical characteristics, shock was defined using shock index (SI) (pulse/systolic blood pressure).21, 22 Acute abdomen incorporated diagnoses, including ruptured viscera, acute appendicitis, bowel perforation, and gastric perforation. Other preoperative diagnoses included compartment syndrome (n = 1), Fournier’s gangrene (n = 1), ostomy prolapse (n = 1), rectal bleeding post-fistulectomy (n = 1), anastomotic leak (n = 2), rectal prolapse (n = 1), blunt abdominal trauma (n = 1), and femoral hernia (n = 1).
We evaluated data distribution and missing data with univariate analysis. Characteristics of the study population were analyzed using descriptive statistics and stratified by delay duration. Tabulations of the perceived reasons for delay were analyzed and visualized using Microsoft Excel (Microsoft 365 MSO 16.0.12827.20200). We assessed the correlation between surgery and anesthesia perceived reasons for delay using Cohen's kappa coefficient.
We performed all statistical analyses with StataCorp v15.1, College Station, Texas. The Malawi National Health Science Research Committee and the University of North Carolina Institutional Review Board approved this study and waived the need for consent.
Results
During the study period, 113 patients met the study criteria, and of these, 106 (93.8%) had complete quantitative data to calculate the duration of IHD. The total cohort's median age was 35.0 years (IQR 24.0–49.0) and was primarily male (87, 82.1%). The most common pre-operative diagnosis was bowel obstruction (44, 41.5%), followed by acute abdomen (29, 27.4%) and inguinal hernia (15, 14.2%). A majority of patients were transferred from another health facility (84, 79.2%). For patients with initial vital signs, almost a third presented with a shock index >0.9 (31, 27.4%) (Table 2).
Patient demographics by length of delay.

Data are presented as a median (IQR) for continuous measures, and % (n) for categorical measures.
We obtained timestamps to calculate the length of time from initial evaluation in the emergency department to operative intervention for 102 patients (90.3%). In our cohort, only 31 patients (29.2%) underwent operative intervention within 2 h from the decision to operate. The greatest proportion of patients (36, 34.0%) experienced an IHD of 3–6 h, followed by a delay of ≥12 h (20, 18.9%) and a delay of 7–12 h (19, 18.4%). The majority of patients (52, 51.0%) waited for 0–2 h between initial evaluation and time to decision for surgical intervention, and 39 (38.2%) waited for 3–6h. A further 31 (31.6%) waited for >12h. Only 9 (9.2%) underwent surgical intervention within 2 h. (Figure 2).

Episodes and duration of delay over the continuum of surgical care.
Perceived reasons for delay were received for 68 patients (60.2%), reasons provided by the surgical team for 65 (95.6%), and by the anaesthetic team for 53 (77.9%). The former identified healthcare system, surgical, anesthesia, and operating theatre delays in 31, 39, 36, and 40 cases, respectively. The latter identified healthcare system, surgery, anesthesia, and operation room delays in 16, 32, 18, and 15 cases, respectively (Figure 3). The delay category did not significantly change when stratified by the duration of delay. Calculations showed consistently no correlation regarding perceived reasons for delay with negative kappa values. (Table 3).
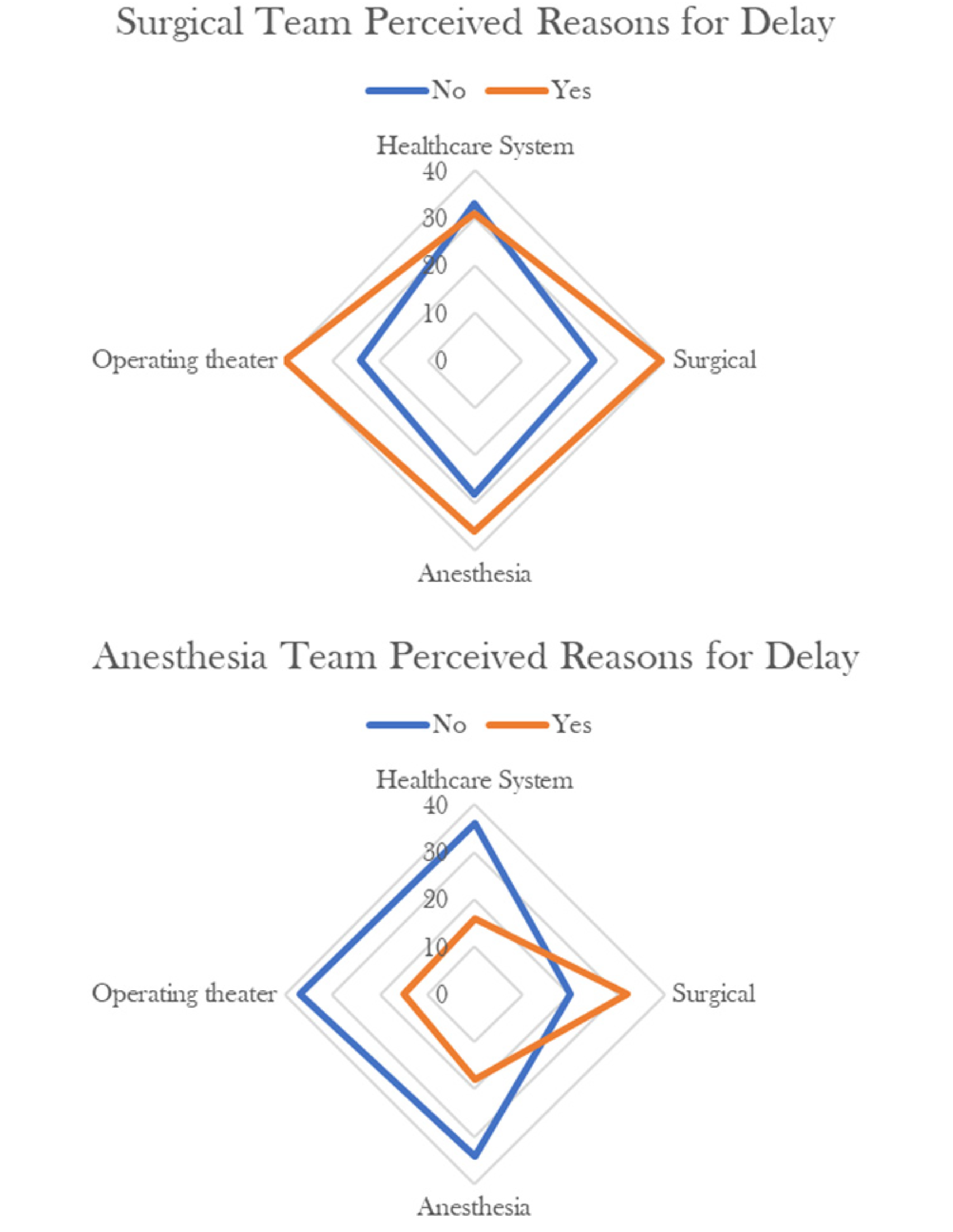
Comparative reason for delays as percieved by the Surgical and Anesthesia teams.
Of the initial 42 pre-determined perceived reasons for delay, we recorded 26 distinct reasons, amongst which the most commonly cited were another case occupying the operating theatre (n = 34), the anesthetist busy on another case (n = 27), night time-staffing limitations (n = 26), and the surgical team busy on another operative case (n = 25). Other less cited reasons for delay included inadequate preoperative resuscitation (n = 16), unavailability of the surgical consultant (n = 10), and delay in acquiring adjunctive diagnostic studies (n = 7).
Categories of perceived reasons for delay.
Discussion
Addressing commonly cited human-resource-related reasons for delay will probably require time and further investment from the Ministry of Health to train and retain healthcare providers. At the same time, additional efforts to bolster the surgical workforce's capacity within the past decade have included creating surgical training programs for physicians and non-physicians in the country. 19 Thus, as Malawi sees an increase in the number of trained surgeons and anaesthetists, we may see a corresponding decrease in the duration of IHDs. However, to ensure that the surgical workforce growth does not stagnate, the Ministry of Health should continue to evaluate and respond to actionable metrics, such as the number of functioning operating rooms, surgical beds, surgical providers, anaesthetists, and nurses per 100,000 people. 23
An interesting finding from this study was that there was no agreement between surgeons and anaesthetists broadly on causes of delay. The one group tended to imply the other as responsible. These perceptions differences may reflect the varying degrees of awareness of barriers the other providers face. They may be an area for intervention as overall communication, and multidisciplinary team dynamics needs improvement.
While there were instances where electricity cuts or lack of running water delayed surgery at KCH, these were significantly less common than delays related to human resource limitations.
Our study has several limitations. The short study period was due to the onset of the SARS-CoV-2, thus limiting observations. Furthermore, it was difficult to differentiate when a delay in operative intervention was clinically appropriate. Finally, the overall aim of the study was to delineate the perceived reasons for IHDs to emergency surgery in our setting, which emphasized observing rather than adjudicating cases to determine a singular reason for delay. While this approach may have contributed to the level of surgery-anesthesia discordance, it also allowed our findings to reflect the barriers encountered in our setting more accurately while minimizing external bias.
To further build upon our study findings, the most immediate future direction should be to explore the intersection of pre-and in-hospital delays and patient outcomes. Most patients were transferred from an outside health facility, thus creating additional delays. Augmenting surgical capacity and efficiency at the district level should mitigate delays.
Footnotes
Acknowledgements
The authors sincerely appreciate the work of the data collection and data entry clerks and the Head of the Department of Kamuzu Central Hospital (Dr Gift Mulima). We gratefully acknowledge the University of North Carolina Department of Surgery, the University of North Carolina Project in Lilongwe, Malawi, and the University of California, San Francisco School of Medicine.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was funded by the National Institutes of Health Fogarty International Center Grant #D43TW009340 (Brittany Robinson and Laura Purcell).
Author contribution
Brittany Robinson: contributed to data analysis and drafting of the manuscript.
Laura Purcell and Rachel Reiss: contributed to the drafting of the manuscript and manuscript revision.
Vanessa Msosa and Onias Mtalimanja: contributed to the acquisition of data and manuscript revision.
Anthony Charles contributed to study design, data analysis, and manuscript revision.
Anthony Charles MD, MPH, UNC School of Medicine, 4008 Burnett Womack Building CB 7228.