
Abstract
Our comparative cohort study, carried out between 3rd January and 30th April 2020, looked at the maternal and perinatal outcomes associated with pre-eclampsia. Of 2019 booked pregnant women, 141 (7.0%) had pre-eclampsia, and 59.8% of these were severe at admission. Significant adverse maternal outcomes were eclampsia, HELLP (haemolysis, elevated liver enzymes, and low platelets) syndrome, and placental abruption, and significant adverse perinatal outcomes were intra-uterine fetal death, preterm delivery, low birth weight (LBW), neonatal asphyxia and early neonatal death. Close attention needs to be given to women with pre-eclampsia in poor resource circumstances.
Introduction
Hypertensive disease of pregnancy is one of the major causes of maternal mortality and morbidity. It includes chronic hypertension, gestational hypertension, pre-eclampsia, eclampsia and superimposed pre-eclampsia. 1
Pre-eclampsia is defined as raised blood pressure occurring at ≥20 weeks of gestation with one or more of the following: proteinuria, acute kidney injury, liver dysfunction, neurological features, haemolysis, thrombocytopenia, or fetal growth restriction. 2 Its incidence varies between 5–10% worldwide.3–5 Its aetiology is unknown, and its pathogenesis suggests an unexplained failure of perfusion of the intra-myometrial segments of the spiral arteries between the 12th and 16th weeks of gestation. The resultant placental ischemia produces vasoactive substances such as endothelin-1, which induce high blood pressure. 6
Some risk factors for pre-eclampsia are well known, including nulliparity, advanced maternal age, systemic lupus erythematosus, (pre-gestational) diabetes mellitus, family history of hypertension, barrier family planning methods and fertility treatments such as assisted reproductive technologies.3,7–9
Complications of pre-eclampsia are numerous: maternal complications include cerebro-vascular accident, retinal detachment, pulmonary oedema, acute renal injury, eclampsia, increased risk of caesarean section and even maternal death. Magnesium sulfate administration reduces the rate of convulsion from 1.9% to 1.1%. 10
Fetal complications are intra-uterine growth restriction (IUGR), placenta abruption, intra-uterine fetal death, premature delivery, birth asphyxia, low birth weight (LBW), and neonatal death. 11
Maternal and perinatal outcomes may be worse where poor pregnancy follow up and labour monitoring are the norm. Thus, we carried out our study in the setting of a low-income country.
Methods
Our comparative cohort study was carried out between 3rd January and 30th April 2020 in three University Teaching Hospitals in Yaoundé, Cameroon. Women with pre-eclampsia as from 28 complete weeks’ gestation (group A) were recruited and followed up till delivery. The diagnosis of pre-eclampsia was based on a blood pressure of ≥140/90 mm Hg occurring as from 20 weeks’ gestation up to 48 h after delivery, associated at any time with a significant proteinuria (≥300 mg/24h). For each woman confirmed with pre-clampsia, three other women admitted immediately after, with gestational ages ≥28 weeks but normal blood pressure of <140/90 mm Hg during the whole pregnancy up to 48 h after delivery (group B), were used as controls (group B). If pre-eclampsia was detected in any woman of this second group, she was transferred to group A.
Women with multiple gestation and those lost at follow-up were excluded, as well as those with incomplete records. Our study received approval from the Ethics committee of the Faculty of Medicine. All women gave their informed written consent.
The variables recorded in all women included maternal age at delivery, parity, GA at first visit and at delivery (confirmed by an ultrasound scan performed <20 weeks’ gestation), number of antenatal visits, mode of delivery, the presence or absence of marginal cord insertion (MCI) (defined in this survey as the insertion of the umbilical cord with its external margin at <2 cm from that of the placenta 12 ) at the examination of the placenta, birth and placenta weight, sex of newborn, Apgar score, maternal and perinatal outcomes. Neonatal asphyxia was defined as a 5th minute Apgar score <7. LBW was defined as a birth weight <2500 g and neonatal infection was diagnosed with a C-reactive protein ˃6 mg/l on the first day of life, a leucocytosis ˃25 × 103 white blood cells/ml or a positive urine or blood culture. Other variables were recorded in women with pre-eclampsia: GA at diagnosis, magnesium sulfate administration, and severity of the disease. The protocol of magnesium sulfate administration was as follows: 5 g given intramuscularly in each buttock, and 4 g intravenously (loading dose: 14 g), then 4 g intravenously every four hours, to be continued under maternal surveillance till 24 h after delivery or after the last convulsion.
Our minimum sample size was calculated to 41 women with pre-eclampsia. Data were analysed using SPSS 23.0. Data of women of group A were compared to those of group B. Fisher's exact test was used to compare categorical variables and t-test to compare continuous variables. We used relative risks with 95% confidence intervals (CIs) to present the comparison between the two groups. Logistic regression was used to control for confounders. P < 0.05 was considered statistically significant.
Footnote: The formula for sample size calculation was N = 2 × (Zα + Zβ/P0-P1)2 × P × (1-P), 13 where Zα = 2.33 corresponding to a type I error of 1%, Zβ = 1.96 corresponding to a power or 97.5%, P0 the proportion of admission of newborn amongst women with PE (59%), 11 P1 the proportion of admission of newborn amongst women without PE (13%) 11 and P is (P0 + P1)/2. To further increase the strength of our studies, we decided to recruit more women with PE.
Results
During our study period, we found 141 booked pregnant women with pre-eclampsia in 2019 admissions (a prevalence of 7.0%). A total of 44 women were excluded (12 for refusal to participate, 19 for being lost at follow-up and 13 for incomplete data).
In addition, 415 women without any hypertensive disease of pregnancy were also recruited, and 42 (10.1%) refused to participate, 47 (11.3%) were lost at follow-up and 35 (8.4%) had incomplete files. The remaining 97 women with PE (group A) and 291 women without PE (group B) were followed up.
Some sociodemographic and obstetrical variables are shown in Table 1.
Some sociodemographic and obstetrical characteristics of the population under study.

RR: Relative risk, CI: Confidence interval, SD: Standard deviation, GA: gestational age, ANC: Antenatal care, NICU: neonatal intensive care unit.
Antenatal clinics in the study population were mainly carried out by obstetricians (59.5%) and nurses (22.4%). Mean GA at diagnosis was 34.4 ± 3.7 (range: 28–43) with 65 (67.0%) between 34 and 43 weeks. Early postpartum period (within 24 h after delivery) diagnosis was made in 4 (4.1%). Severe pre-eclampsia (blood pressure ≥160/110 mm Hg, with or without headache, visual disturbances, epigastric pain or oliguria) was observed in the majority of women at diagnosis (58, 59.8%).
The two groups were similar with regard to maternal age and fetal sex (Table 1); with no statistically significant difference concerning urban residency, unmarried status, rate of past caesarean or cord abnormalities. Although not statistically significant different, nulliparous women were more in group A than in B.
Women with pre-eclampsia had fewer antenatal visits; 29 (29.1%) had <4 visits, and only three women had at least eight visits. Such women with <8 visits were therefore found more in group A.
Induction of labour was carried out more often amongst group A. Success was reported in 14 (70%) in group A as against 16 (84.2%) in group B. Caesarean sections were more frequent amongst group A (Table 2). Additionally, instrumental vaginal delivery, mainly indicated for Acute fetal distress (AFD), was carried out more amongst women of group A. Induced prematurity was found among 30/44 (68.2%) of group A as against 9/42 (21.4%) of group B.
Indications for caesarean sections in the population under study.
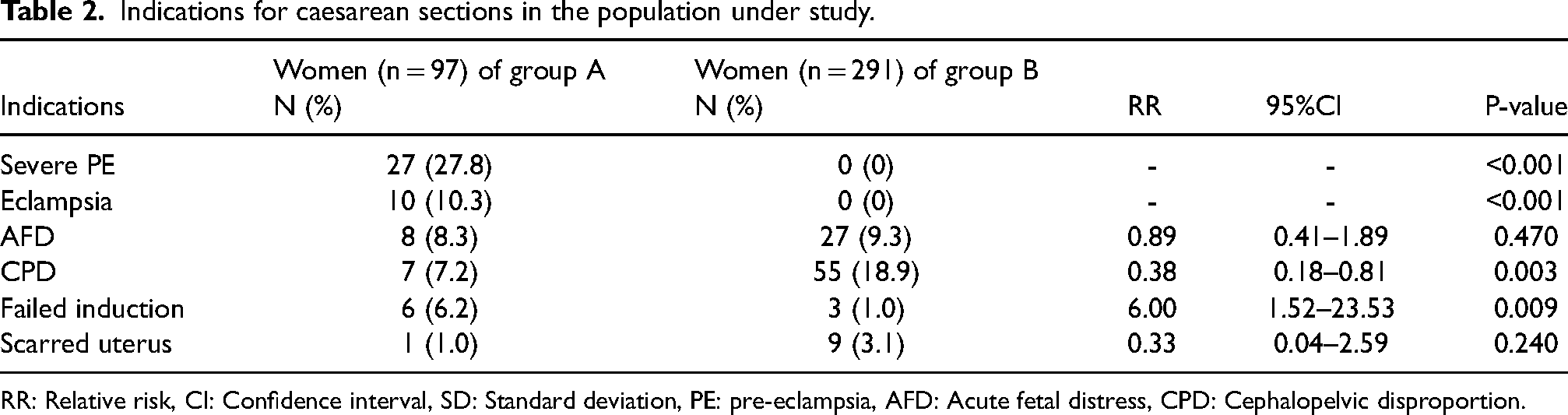
RR: Relative risk, CI: Confidence interval, SD: Standard deviation, PE: pre-eclampsia, AFD: Acute fetal distress, CPD: Cephalopelvic disproportion.
LBW was more in group A (Table 1), remaining associated with pre-eclampsia even after adjustment for prematurity and intra-uterine fetal death. There was no statistically significant difference in placenta weights between the two groups.
MCI was more amongst group A. Placenta abruption was, however, significantly associated with pre-eclampsia, even after adjustment for the former. (Table 3).
Maternal outcomes of the population under study.

RR: Relative risk, CI: Confidence interval, HELLP: Hemolysis Elevated Liver Enzymes Low Platelets, PPH: postpartum hemorrhage, ICU: Intensive care unit.
Eclampsia occurred amongst 17 (17.5%) of group A, occurring during pregnancy amongst 10 (58.8%), one during labour and 6 (35.3%) after delivery.
Among the 58 women with severe pre-eclampsia, all of whom received magnesium sulfate, 12 (20.7%) had eclampsia as compared to 5/39 (12.8%) with non-severe pre-eclampsia who had not received it. Table 4 summarizes the adverse maternal and perinatal outcomes associated with pre-eclampsia.
Adverse maternal and perinatal outcomes associated with pre-eclampsia.

*adjusted for marginal cord insertion, **adjusted for prematurity and IUFD.
RR: Relative risk, CI: Confidence interval, aRR: adjusted relative risk, HELLP: Hemolysis Elevated Liver Enzymes Low Platelets, PPH: Postpartum hemorrhage, ICU: Intensive care unit, IUFD: intrauterine fetal death, LBW: Low birth weight, NICU: Neonatal intensive care unit.
Admission in the neonatal intensive care, indicated for prematurity, LBW, neonatal asphyxia or infection, were more frequent in group A (Table 1). Pre-eclampsia was associated with more perinatal death (15/97 or 15.5% vs 13/291 or 4.5%).
Discussion
Significant maternal adverse outcomes were eclampsia, HELLP syndrome, placenta abruption, high caesarean section risk, blood transfusion and admission in the intensive care unit (ICU), while adverse perinatal outcomes were intra-uterine fetal death, pre-term delivery, LBW, neonatal asphyxia, neonatal infection, newborn transfer to the neonatal ICU and early neonatal death.
Our rate of pre-eclampsia is similar to the 7% rate observed in Nigeria. 14 Eclampsia occurs nowadays in <1 out of 10,000 pregnancies in high-income countries, with its associated maternal mortality being <1%. 1 Our high rate of eclampsia may be explained by the poor follow up of women, exemplified by their usually late booking (Table 1) and the fact that the vast majority had <8 recommended visits, as recommended by WHO in 2016, 15 given that non-severe pre-eclampsia can progress rapidly to severe or to eclampsia, 16 as demonstrated in our survey. Although eclampsia is more frequent before delivery, it also occurs after, and therefore, women with pre-eclampsia should be well monitored even after delivery. Cases of eclampsia even in women with non-severe pre-eclampsia are reminders that magnesium sulfate should always be available in the maternity wards to enable early treatment and prevention of eclampsia.
The rate of HELLP syndrome and placenta abruption were similar to rates observed in South Africa. 17
Caesarean section and intensive care admission rates depend on many factors, including availability, protocol, and costs, and so are not readily comparable. Our high rate of eclampsia, failed induction and placenta abruption, certainly contributed to our intervention rates, and obviously related to a high rate of blood transfusion, as well as intra-uterine fetal death rates.
Although we did not record twin deliveries, pre-term delivery was inevitably frequent owing to our active management of pre-eclampsia; this inevitably results in low birth weights, and increased perinatal death rates, but is justified in there having been no case of maternal mortality in our series as a result of eclampsia.
A limitation of our survey is that we recruited only cases confirmed with proteinuria and we might have missed some other cases, especially if they occurred at home or >48 h after delivery.
Conclusion
Severe pre-eclampsia is not uncommon in our environment. Women should be encouraged to start Antenatal care (ANC) earlier and to attend for more visits to allow early diagnosis and management of pre-eclampsia. Close attention should be offered to women even after delivery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.