
Abstract
The existing referral system from primary institutions to higher institutions within our health district for obstetric patients has not been subjected to any analysis of shortcomings. We therefore made an assessment of resultant adverse maternal, foetal and neonatal outcomes by a prospective observational cohort study done over a 6-month period at a tertiary centre. Data were collected from 317 patients. We found an important failure to identify high risk patients at primary institutions. This resulted in an increased overall adverse outcome five-fold, adverse maternal outcome seven-fold, adverse neonatal outcome six-fold and stillbirth four-fold. Ongoing training and use of updated guidelines are our urgent recommendations.
Introduction & background
The United Nations Sustainable Development Goal 3 target states that by year 2030, the global maternal mortality ratio should be <70 per 100,000 live births and the neonatal mortality ratio <12 per 1000 live births. 1 The ‘Saving Mothers’ report of South Africa (2017–2019) states that rapid and reliable emergency transport, along with appropriately trained health care workers and resourceful health care facilities are important pillars of the current health referral system to reduce maternal mortality. 2 An important factor related to avoidable maternal death was referral problems between institutions, and these mainly owing to transport issues, with a secondary factor being poor inter-institutional communication between health care personnel.
A referral system for obstetric patients has been present in the Pietermaritzburg complex, and although referral patterns have been studied in the Pietermaritzburg Metropolitan Critical Care service, 3 no study has been done in the field of Obstetrics & Gynaecology. This area has a high litigation rate and our study aims to identify problems and provide appropriate solutions to minimise adverse outcomes and provide better health care.
Each level of health care from primary to tertiary caters for different categories of patients depending on the severity of their illness. 4 The intention is that patients attend the primary health care which is nearest to their residence first and then, depending on the severity of their condition, they are treated or referred. The onus is therefore on the health care provider at each stage to decide if criteria are met for the patient to be managed or referred further. It goes without saying, that delays in necessary referral will inevitably result in increased adverse outcomes.
Most patients needing tertiary referral are transferred by Emergency Medical Response Services (EMRS) by road or air. The EMRS crew are responsible for patients’ health in transit and therefore their timely management is also important to prevent adverse outcome.
Various studies done in Africa and Asia,5–13 related to referral patterns, analysed different parameters of referral. While some studies evaluated the strengths and weaknesses in the referral pathways, others were done to obtain data related to number of patients referred, cases referred and specific days of the week which had more referrals.
Analysis of the referral pattern in other countries5–8 showed that health care personnel related factors as well as lack of infrastructure were major shortcomings which contributed to adverse maternal outcome. Delays in referral due to transport related issues, along with substandard care during the transport of patients were shown to increase maternal mortality in other studies.9–13 In South Africa, inter-facility transport problems are reported as resulting in 1 out of 10 maternal deaths, with miscommunication being responsible for 253 maternal deaths out of 3438 cases between 2014 and 2016. 2
The objectives of our prospective observational cohort study were to assess referral patterns and identify deficiencies in the referral system in each case, to determine possible association between adverse events and referral pattern short comings, and finally, to outline improvements which can be made to the current referral pattern, even when no adverse outcome was reported.
Method
Ethics approval was obtained from the Biomedical Research Ethics Committee (BREC/00001196/2020), Department of Health as well as Grey's Hospital before starting data collection. The study group comprised of obstetric patients referred over a six-month period from 1 June 2020 to 30 November 2020, from drainage areas according to referral patterns. Referral criteria according to Grey's hospital policy were used. All in-patient records were analysed. The referral system was analysed and shortcomings noted, and patients followed up for adverse outcomes. Our study sample comprised of 423 patients, of whom 106 were excluded, (Figure 1) mostly (41%) because they walked to the hospital or used their own transport, without being known prior to Grey's hospital. These were mostly low risk patients and were either delivered or ‘stepped down’ to their base hospital. Limited data were available in 28% of cases owing to unavailability of records or limited information. 16% of patients excluded, had gynaecological issues. Some 7% were ‘walk-ins’ known to Grey's hospital and another 7% were accepted directly as emergencies without passing through gynaecological out-patients. Four were accepted for neonatal reasons.
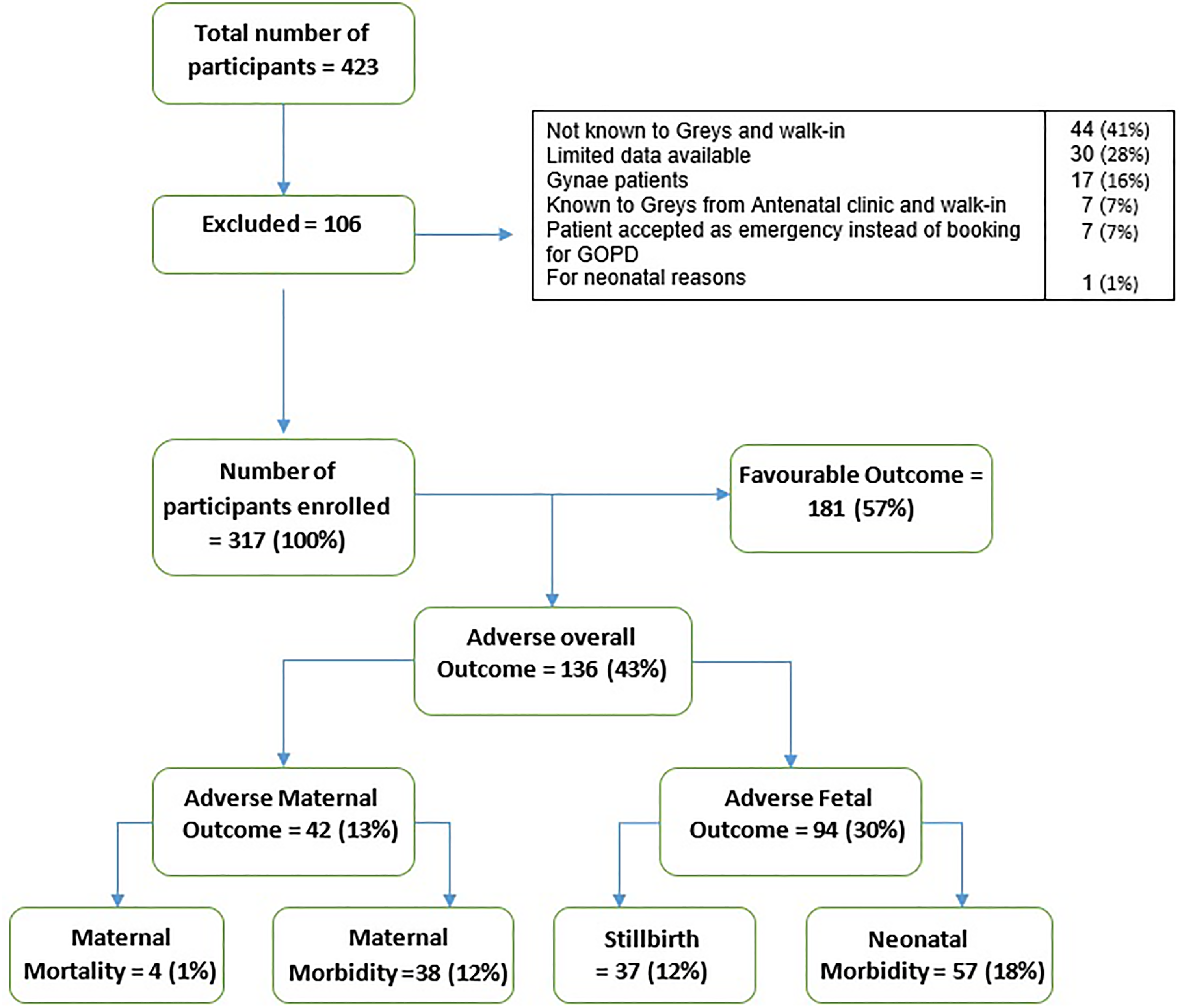
Flowchart showing participants selection and exclusions.
Outcomes measured were maternal or foetal mortality or morbidity. Maternal morbidity included Intensive Care Unit (ICU) admission, need for blood products, hysterectomy, obstetric haemorrhage and obstetric anal sphincter injuries. Neonatal morbidity included infection, cerebral palsy, hypoxic ischaemic encephalopathy, need for intubation and intensive care admission.
Data were analysed using IBM SPSS statistics version 22. All descriptive statistics covering the demographics, health care worker factors at base, transport factors and all other thematic areas were analysed. Pearson's chi-square test was used to test for associations between referral system practices and perinatal outcomes. Demographic and other confounding variables were also tested for association with adverse perinatal outcomes. Confounders were controlled by including statistically significant outcomes in subsequent logistic regression models.
Results
Table 1 shows the demographic characteristics of the study population. The variables were categorised according to the primary health care institution from which the patients were referred. The majority of patients were in the age group 18–24 years. Teenage pregnancy constituted 10% of all patients, and most (33%) patients referred had a Body Mass index (BMI) in the overweight range (33%) (according to CDC classification), with 20% having a BMI > 35. Most (74%) patients were primipara, and 40% were term, and 26% early preterm. Most (83%) patients were unemployed but healthy (95%) without any prior comorbidity. Almost all patients who had previous comorbidity had previously been seen and followed up at the antenatal clinic at Grey's hospital. Human Immunodeficiency Virus (HIV) infection was noted in 74% and most were taking antiretroviral treatment. Antepartum referrals consisted of 92%, while the remainder were delivered at base and then referred for further management at Grey's hospital
Demographics of participants (n = 317).

Most (73.5%) referrals came from district hospitals with a diagnosis of pre-eclampsia in 68%, being the most common reason for referral (Figure 2). Most of these patients were referred from district hospitals (n = 150), followed by community health centres and clinics. A similar pattern was observed for referral of patients with eclampsia, abruptio placenta, postpartum haemorrhage and those with cardiac disease. Some 51 were referred for other reasons.

Bar chart showing number of referrals from primary institutions and diagnosis.
Among the 317 patients studied, 136 had an unfavourable outcome (Figure 4), affecting the mother in 42 and the baby in 94. There were 4 maternal deaths. There was need for blood products due to obstetric haemorrhage in 28 patients and ICU admission for 14 of the patients. 8 underwent hysterectomy as an emergency procedure. There were 3 cases of ruptured uterus which were repaired without need for hysterectomy. 4 cases of obstetric haemorrhage were noted without need for blood products. 4 cases of obstetric anal sphincter injuries were noted, all referred post-delivery from primary institutions. Some patients had more than one adverse outcome hence Figure 3 represents all the 65 adverse maternal outcomes in a total of 42 patients.
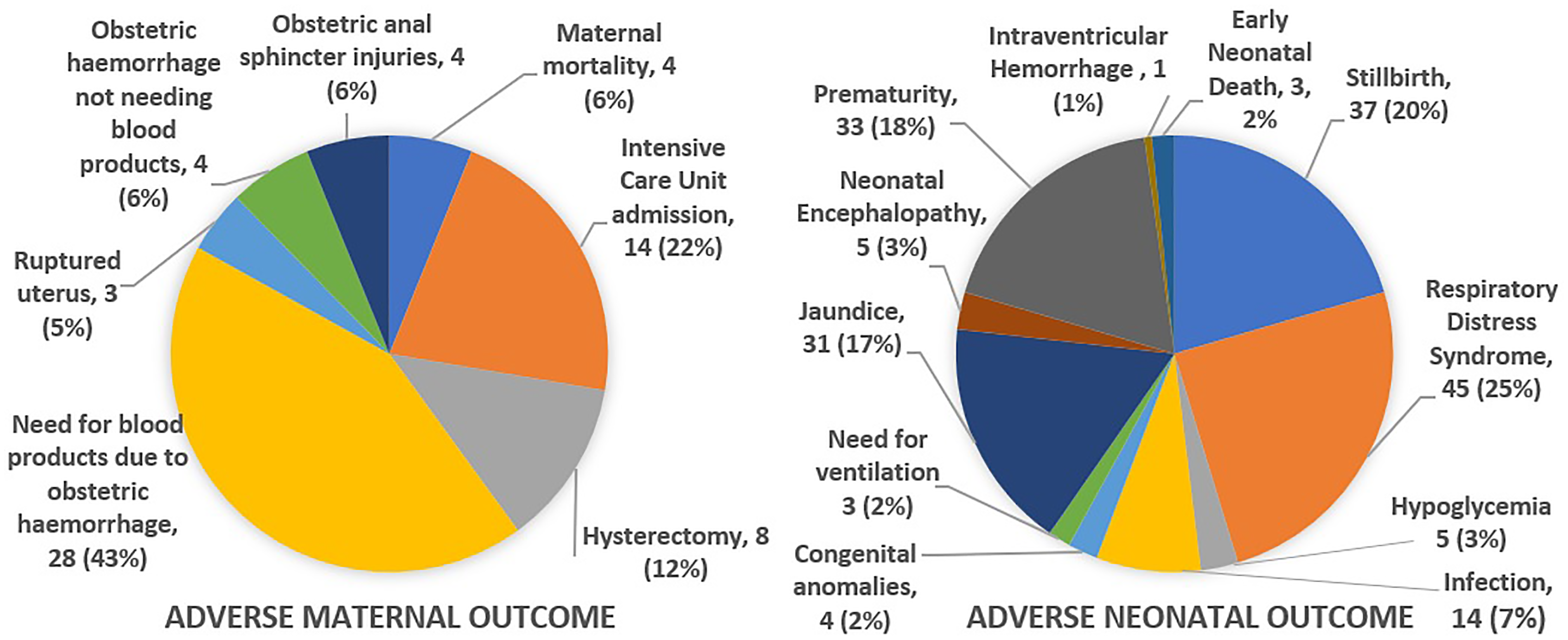
Adverse maternal & neonatal outcomes.
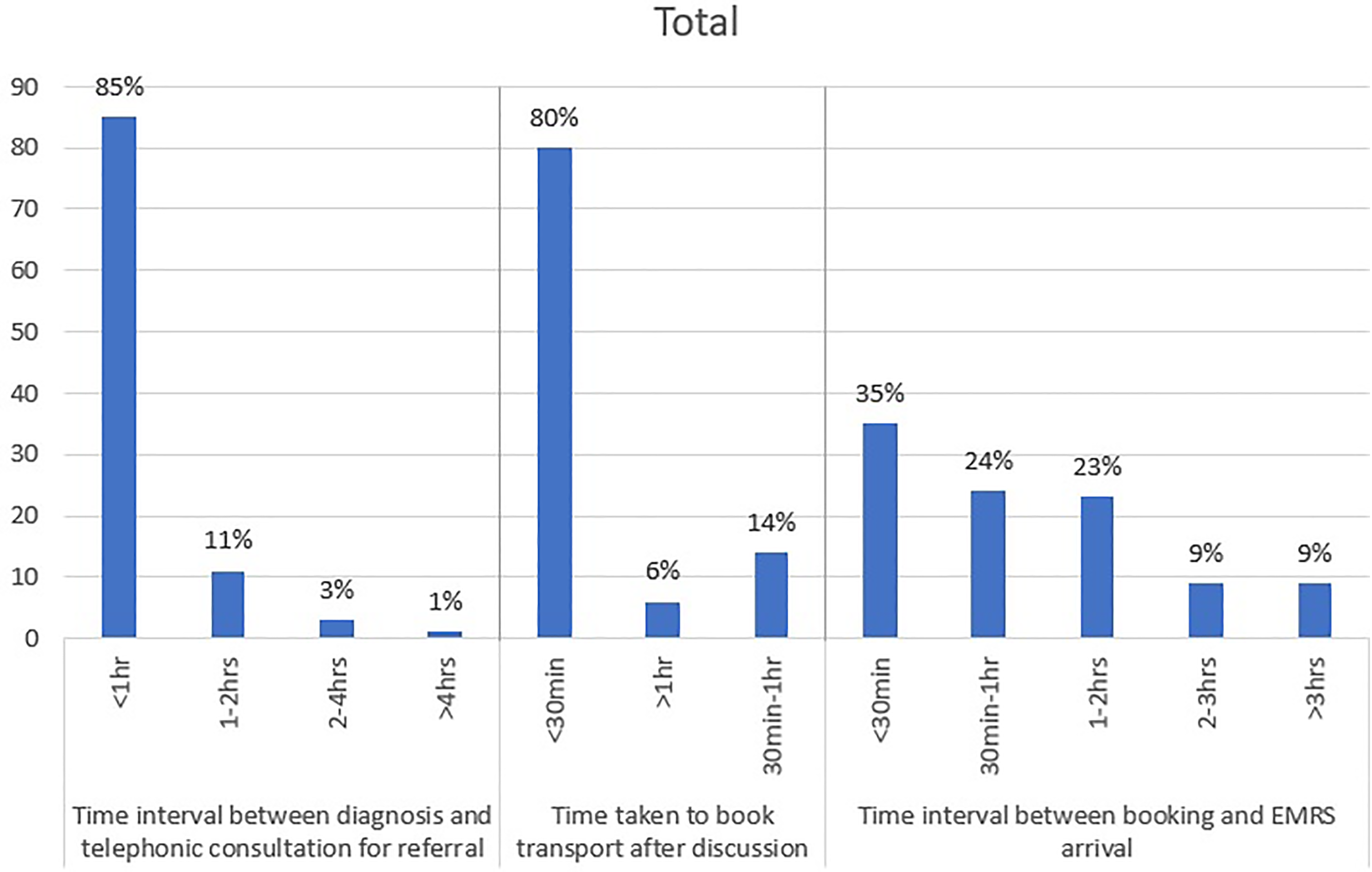
Bar chart showing time intervals.
There were 37 stillbirths noted. The delivered babies were followed up in the ward and NICU. Since many babies delivered at Grey's hospital are preterm due to maternal morbidities, there a were a high number (45) of respiratory distress syndrome noted. With 33 cases of prematurity, many had prolonged NICU stay. Jaundice developed in 31 babies needing phototherapy and 14 had neonatal infections, requiring treatment. Of importance also were five cases of neonatal encephalopathy and one case of intra-ventricular haemorrhage discharged only after a prolonged intensive care. Three babies died. There were a total of 94 babies with 181 adverse outcomes since a baby may have more than one adverse outcome.
The bar chart shown (Figure 4) depicts three different time intervals; firstly, time taken between making the diagnosis at the referral institution and telephonic consultation for referral; secondly, the time after being accepted for transfer at Grey's hospital and booking transport: and thirdly, the time interval before arrival. In terms of EMRS response after booking, the time interval varied from <30 min in 35% of cases to <2 h in 47% and >2 h in 18% mainly because of lack of ambulances available. In nine cases, due to COVID-19 pandemic, there were delays due to protective measures taken in the ambulances.
Some delays occurred when the doctor at the referral institution was not able to see the patient immediately because of other emergencies. In seven cases technical issues were noted, when the EMRS could not be reached by phone, and in 14 cases, even after the diagnosis was made and the patient discussed, further information was demanded by health personnel at Grey's hospital. Specifically, early on in the COVID-19 pandemic, 11 patients had to wait for their COVID-19 results before transfer, and the results were available only after a few days! Fortunately, the delay did not result in any adverse outcome since the patient were being followed up regularly with updates given by the base hospital.
Among all the parameters analysed, failure to identify high-risk patients by health care personnel at the referring institution reached statistical significance (Figure 5). This implies patients continued having routine antenatal care and were not followed up closely or referred appropriately early. This increased the odds for an overall adverse outcome almost six-fold (OR = 5.7, 95% CI = 1.5–10.6). Adverse maternal outcome increased eight-fold (OR = 7.5, 95% CI = 2.9–12.2) and adverse neonatal outcomes six-fold (OR = 6.1, 95% CI = 1.8–12.4). Failure to identify high risk patients also increased the risk of stillbirth five-fold (OR = 4.7, 95% CI = 1.6–8.7). Transport, technical issues and other shortcomings did not affect overall adverse outcomes. Appropriate management of the patient during transport was another factor which had a significant P value (p = 0.03) but non-significant statistically confidence intervals (OR = 0.2, 95% CI = 0.1–1.1). Other parameters tested which were not statistically significant, but were clinically significant are discussed below.
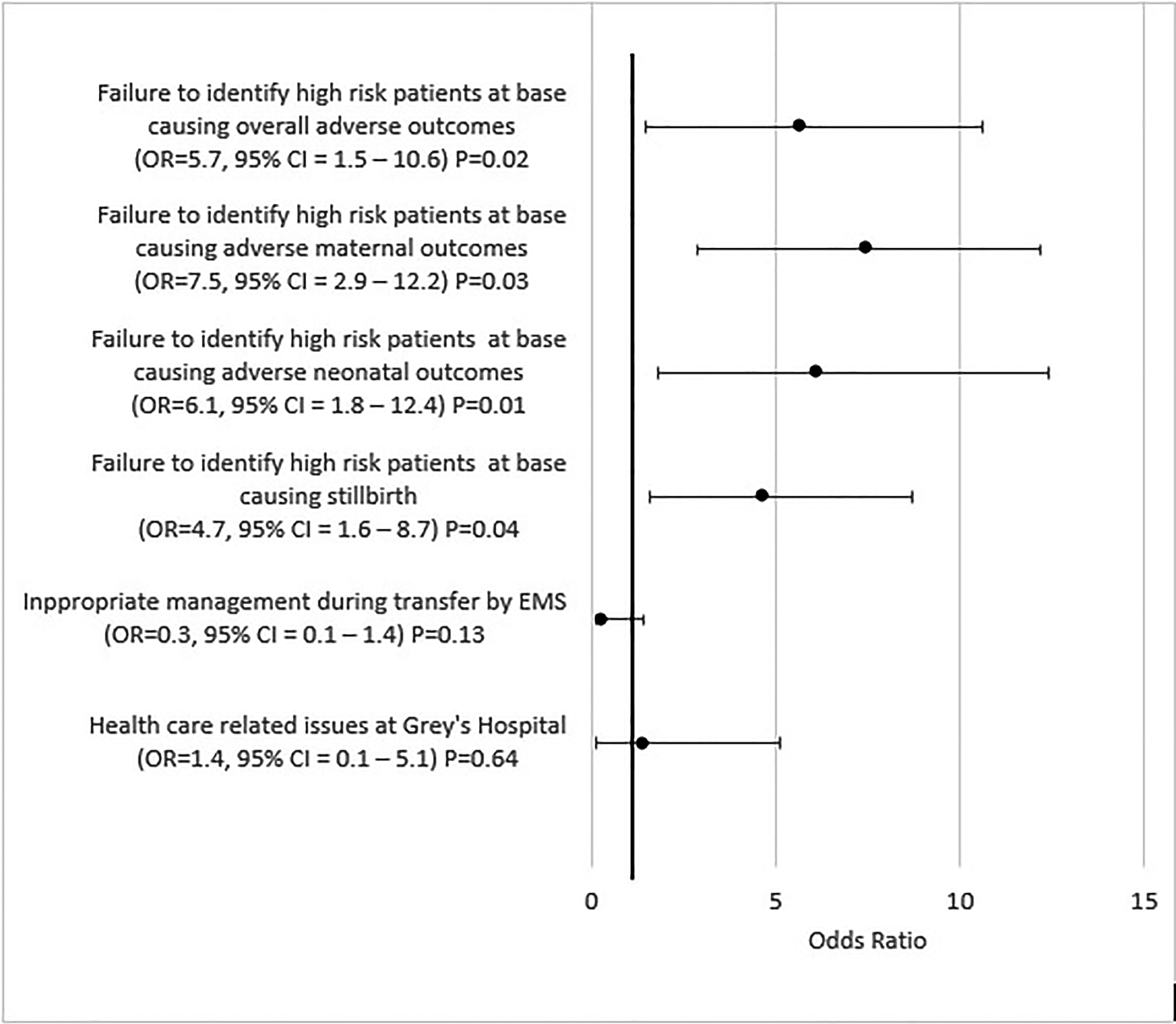
Confidence interval plot showing primary outcomes.
Secondary outcome
The flowchart (Figure 6) shows the result of secondary outcomes which were investigated. Although these shortcomings did not contribute to any adverse outcome, they represented significant issues which may result in adverse outcome in other situations. Transport issues were the highest with 90% of shortcomings: 13 of the patients were not adequately monitored. The issue we found concerning was that in 55 cases, although the patients were monitored, no action was taken in response to patients’ change in condition or abnormal vitals like high blood pressure
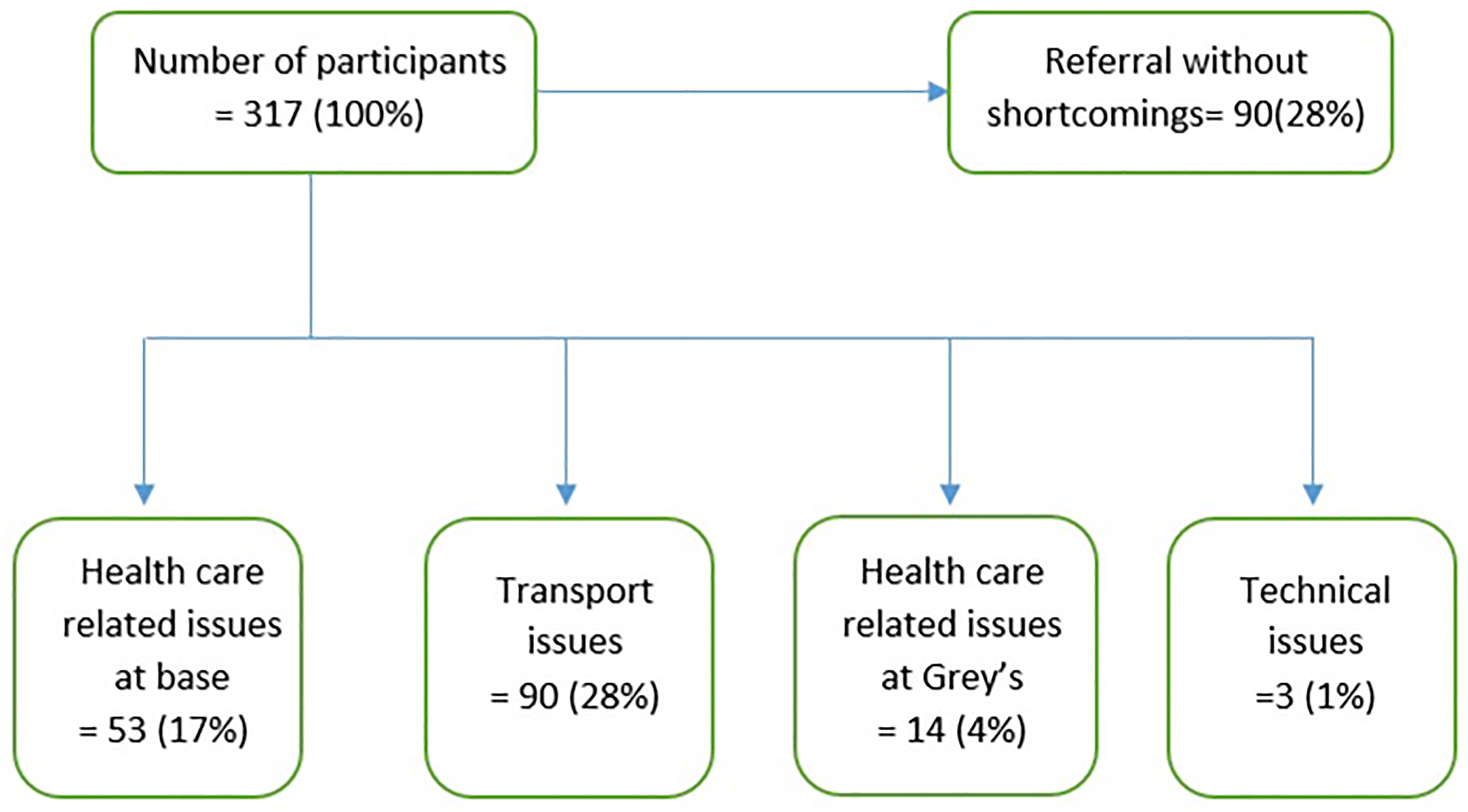
Flowchart of secondary outcomes.
Evidence of substandard care at the primary health care institutions was analysed. Multiple shortcomings were noted (Figure 7). Even after making a correct diagnosis, proper treatment was not offered to 17 patients, who were hence not referred. In 82%, treatment according to local guidelines was not provided, and in 6%, this involved incorrect doses of medication. Failure to make a correct assessment constituted 6% of all shortcomings.
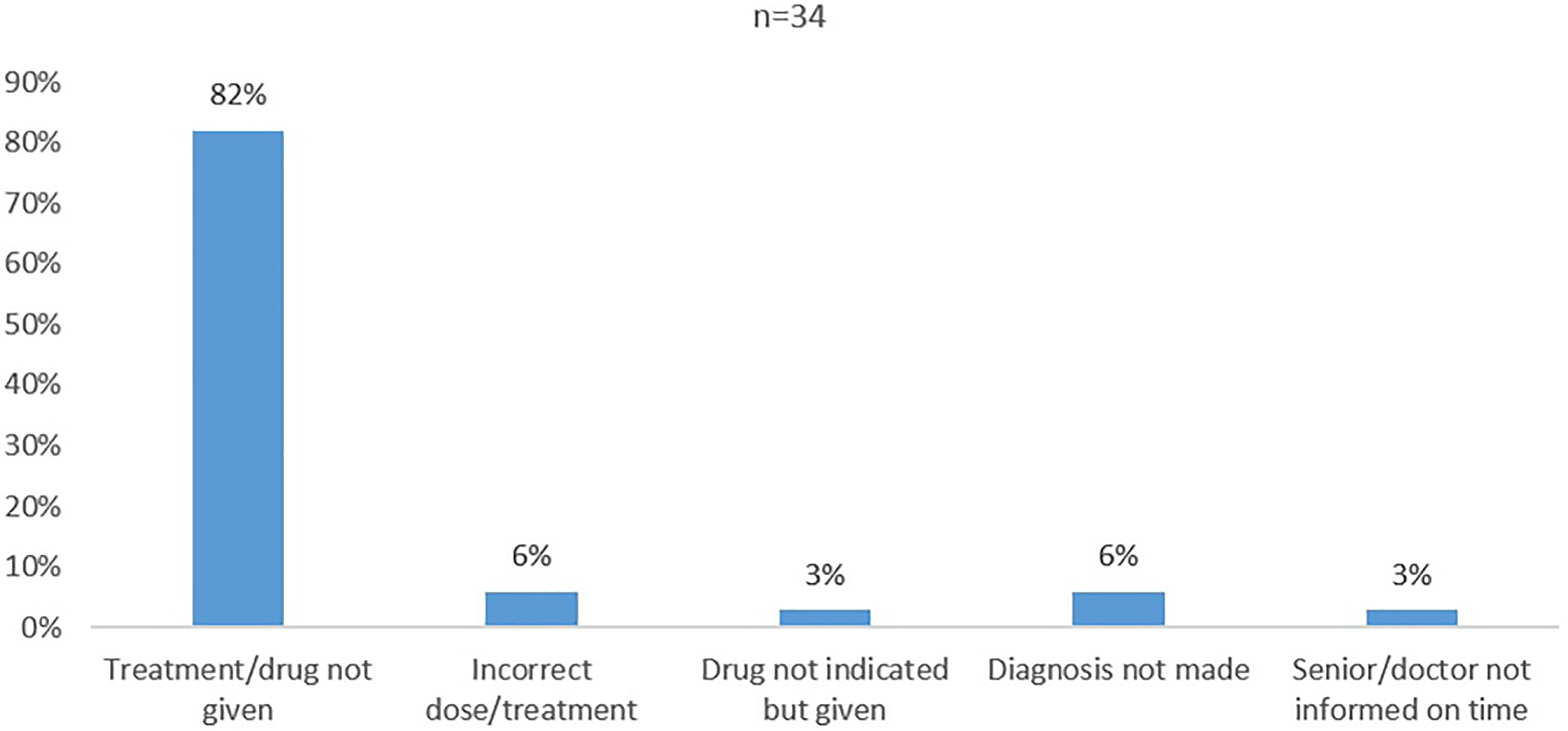
Reasons for substandard care.
Furthermore in 14%, the key problems were correctly noted but the patient was never discussed for referral. In a further 4%, there was a delay of >2 h before a diagnosis was made and the patient was discussed for referral.
Regarding referral, all patients are discussed with the registrar in labour ward or the doctor on call and a decision is then made to transfer the patient or follow-up at base. Among 310 cases analysed, in 12 cases advice given from Grey's hospital to primary institution regarding care of patient was not appropriate or inadequate. We cannot comment on verbal advice given but only on documentary evidence. In 4 cases patients diagnosed with pre-eclampsia with severe features were not accepted and referred to the antenatal clinic the next day. In the same way, patients who should be referred to the antenatal clinic at Grey's hospital were actually accepted, e.g. stable patient with bronchial asthma, patients with preeclampsia without severe features and stable patients with suspected morbidly adherent placenta without any symptoms. Sometimes, the decision is influenced by the health care worker at the primary institution, who will give a worse picture of the patient, so the patient can be referred.
When a patient is handed over to Grey's hospital by EMRS ambulance, they usually are admitted in labour ward. They are initially seen by the nurses/midwives and then by the registrar or medical officer. Management of patient at Grey's hospital is facilitated by consultants and subspecialists. Hence the treatment plan for each patient is made on a day to day basis according to the patient's condition. Although there was no statistical significance for inappropriate management at Grey's hospital which led to any adverse outcome, few issues were identified where improvement could have been made. Many of the issues were isolated and not recurring and hence did not affect the final study. All these shortcomings were obtained from file of patients and telephonic consultation form.
There were 84 cases whereby there was a delay of more than 1 h between admission and final management plan, most commonly due to the doctor being busy in theatre or with other patients. There were two cases whereby the patients had pathological cardiotocographs with adverse outcomes. One patient delivered a stillborn due to inappropriate monitoring following suspicious cardiotocographs. The second patient had a pathological cardiotocograph for more than 2 h at night, with all doctors on call busy in theatre with another patient. She delivered a baby at term of more than 2500 gm, who subsequently was diagnosed with neonatal encephalopathy.
Though not statistically significant, the cases mentioned above could have been prevented by closer monitoring of patients and taking appropriate and timely decisions. Most patients who were referred had good outcomes. In most cases, maternal deaths were unavoidable due to other medical conditions. All patients who had stillbirths were actually referral from other institutions due to their maternal conditions. The stillbirths occurred before referral to Grey's hospital. These reasons explain the high number of stillbirths at Grey's hospital (n = 36). All these cases are analysed in regular meetings and all concerned health care workers are invited to discuss the shortcomings and action plans to be taken as preventive measures.
Individual cases with adverse outcomes
There were 11 cases identified in the study period where health care related issues directly resulted in adverse overall outcomes. There were two cases of abruptio placenta grade 3 which could have been prevented if they were followed up more closely or referred earlier. In another case of abruptio at a district hospital, the doctor was informed only 1.5 h later leading to the patient having postpartum haemorrhage after delivery of a stillborn and transferred to Grey's hospital where the patient had a hysterectomy. In another case of antepartum haemorrhage with a live baby, there was 6 h delay to transfer a patient from a clinic to district hospital resulting in stillbirth and need for blood products for the patient. There were other cases of preeclampsia with severe features with stillbirth which could have been prevented, had risk factors been identified by health care worker at primary institution as mentioned earlier. There were isolated cases of adverse maternal outcome at district hospitals due to anaesthetic reason and one pregnant patient diagnosed with supraventricular tachycardia but adenosine was not available at the district hospital.
Discussion
Based on our study, we found that health care workers at base contributed to adverse maternal and neonatal outcome mainly because of failure to identify patients with risk factors who need tertiary level care. Essential Steps in Management of Obstetric Emergencies (ESMOE) training should be ongoing amongst both doctors and nurses, especially new health care workers. They should also be supported by senior colleagues or be advised by other health care workers when needed so appropriate management is given to the patient. Guidelines which are implemented should be made readily available, in electronic versions on mobile phones or as hard copies to be used in hospital whenever needed.
Transport of patients itself did not contribute to major adverse outcomes. Even if there were many shortcomings identified, they were not statistically significant. This is in contrast to other studies in middle to low income countries, where transport services are deficient, although delay was caused when all ambulance services were all in use. Further, since most patients referred have pre-eclampsia, blood pressure monitoring during transport is obligatory. However, paramedics in some ambulances are not allowed to administer drugs. Although we did not find any adverse outcome thereby caused, we feel this practice needs to be revised. Continuous professional development for ambulance personnel would keep them up to date with latest guidelines.
The strength of this study is that there was only one investigator hence reducing inter-observer bias. Standards were set as per protocols used locally and in the Pietermaritzburg complex to analyse files. Since the study was prospective, all files were analysed daily and were readily available in ward. In few excluded cases, files were not available. Hence there was no loss to follow-up of cases for patients in the ward or for neonates in ICU. Also, multiple factors could influence the maternal and neonatal outcomes. Different confounders were taken into consideration and all these variables were collected and analysed by regression models.
A limitation of this study is its small sample size (n = 423) and hence it may not reflect other shortcomings which are present and may be more significant. Also, the time period of six months for which data were collected may not take into consideration other significant factors occurring over other periods.
Conclusion
Ongoing ESMOE training and regular feedback meetings to discuss any adverse outcomes help improve awareness. Use of appropriate and updated guidelines should be enforced. Referral criteria should be rigorously followed and failures investigated. A change in policy regarding the ability of paramedics in ambulances to react against any changing or worsening condition of a patient during transport needs urgent consideration.
Footnotes
Acknowledgements
We thank Grey's hospital staff for their support during data collection process and Mr Promise for working out the statistical analysis.
Author contributions
Conception by Prof T.D. Naidoo, Data collection, analysis and final draft by Dr S. Jeeana. Statistical analysis by Mr Promise.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.