
Abstract
Coronary heart disease and its complications remain the most common cause of morbidity and mortality throughout the world. In addition, its incidence among adults <45 years of age has also been steadily increasing in the past few decades. Besides the typical aetiology such as coronary artery abnormalities or autoimmune disorders, increasing rates can be attributed to escalating trends of obesity, type 2 diabetes mellitus, and illicit abuse of drugs such as cocaine and amphetamines in the younger population. 1 Every cardiovascular event in a young adult must be thoroughly investigated as the aetiology is typically unconventional. Our case reports a young man who developed an acute inferior wall myocardial infarction (IWMI) in the setting of hyperhomocysteinaemia secondary to vitamin B12-folate deficiency itself due to tropical sprue.
Case report
A 27-year-old male presented with complaints of a sudden, dull epigastric pain with shortness of breath. His jugular venous pressure was elevated. Pallor and knuckle pigmentation were appreciated, along with fine crepitations in the right infraclavicular region. A 12-lead ECG exhibited significant ST-segment elevation in leads II, III, and aVF, suggestive of an acute inferior wall myocardial infarction (IWMI). He was immediately started on unfractionated heparin. His angiography demonstrated a re-canalized right coronary artery.
Upon further investigation, a complete blood count revealed an anaemia (Hb of 76 g/L), low platelet (102 × 109/L) and WBC count (3.5 × 109/L), suggestive of pancytopenia. Moreover, a high mean corpuscular volume (105 fl), macrocytes, and hyper-segmented neutrophils on peripheral smear indicated a diagnosis of megaloblastic anaemia. In addition, our patient had a low vitamin B12 (129 pmol/L) level, low serum folate (<1.36 nmol/L) level, and an elevated homocysteine level (>55 µmol/L). A bone marrow aspiration showed features of erythroid hyperplasia with a megaloblastic picture.
To determine the underlying cause of folate-B12 deficiency, a duodenal biopsy was performed, which revealed focal blunting of villi, crypt hyperplasia, and increased intraepithelial lymphocytosis suggestive of tropical sprue (Figure 1). Our patient was thus started on vitamin B12 and folic acid supplements, aspirin and clopidogrel, and a doxycycline course for two weeks. Subsequently, blood counts improved, and he could be discharged with advice to continue vitamin supplementation and dietary modifications. At his two-month follow-up, he reported no new complaints and showed clinical signs of improvement.
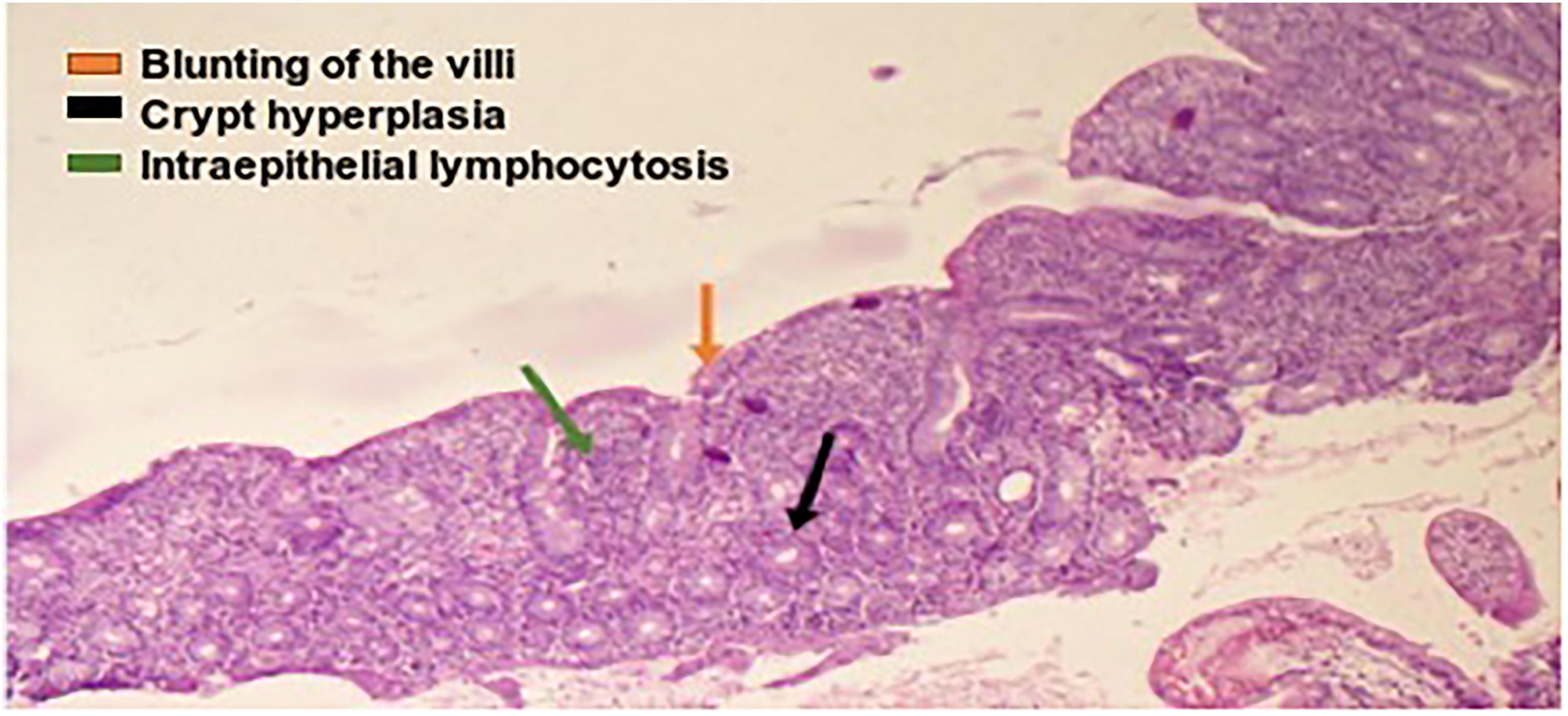
Histopathology of duodenal specimen, suggestive of tropical sprue.
Discussion
Hyperhomocysteinaemia is a condition in which the serum homocysteine (Hcy) levels exceed 15 µmol/L. 2 It can be caused by various pathology such as vitamin B12 or folate deficiency, hepatic or renal dysfunction, diabetes mellitus, malignancy, or certain drugs such as folate antagonists, metformin, anticonvulsants, and thiazide diuretics. 2 Homocysteine is a sulfur-rich amino acid converted to methionine which requires B12 as a cofactor. 3 Severe elevation of homocysteine are usually associated with genetic defects involving its metabolism because of mutations of the enzyme cystathionine β-synthase or methylene tetrahydrofolate reductase (MTHFR) gene. 4 Cofactor/vitamin deficiencies are usually associated with mild to moderate elevations of Hcy.
Homocysteine accelerates the development of coronary artery disease by various mechanisms. It contributes to the increased production of free radicals by activating NADPH oxidase and nitric oxide synthase, which ultimately leads to the formation of superoxide and peroxynitrite radicals. 5 Lastly, it upregulates procoagulants, such as tissue factor and downregulates anticoagulants like thrombomodulin, protein C, and antithrombin III, resulting in an overall prothrombotic state.3,5,6 The oxidative nature of Hcy provides a foundation for activating numerous pro-inflammatory pathways, ultimately leading to a downward cascade of endothelial dysfunction, plaque rupture, and thrombosis.
Vitamin B9 and B12 deficiencies are due to conditions of impaired nutritional intake including veganism, alcoholism, and malnutrition. However, in our patient, the culprit was due to impaired absorption. Tropical sprue is a chronic malabsorptive disorder with a multifactorial aetiology that includes gut dysbiosis, neurohormonal dysregulation, and an impaired host immune response.7,8 Clinical and histological features overlap with other malabsorptive disorders such as bacterial overgrowth syndrome, inflammatory bowel disease, and gluten-sensitive enteropathy. Nevertheless, a clear distinction in our patient could be made owing to our patient's swift response to a short course of broad-spectrum antibiotics, the persistence of gastrointestinal symptoms despite a gluten-free diet, and absence of the HLA haplotype DQ2/8 and antibodies associated with coeliac disease (anti-TTG, anti-gliadin).
A wide array of investigations is usually performed for any young adult presenting with a cardiovascular event as it may be due to an exceptional cause. Autoimmune panels are carried out for various connective tissue disorders such as lupus, rheumatoid arthritis, and APLA tend to have coexisting cardiac involvement.
The authors report no funding or conflicts of interest Consent was obtained from the patient for publication of this case.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.