
Abstract
Guinea-Bissau has particularly alarming indicators of maternal health, with one of the highest maternal mortality (MM) worldwide. According to UNICEF-2014, this ratio (MMR) was 900/100,000 live births, mostly due to preventable and treatable causes. In 2013, the European Union developed an Integrated Programme to reduce Maternal and Infant Mortality (EU/PIMI),** the largest project of this kind, implemented in Guinea-Bissau. This study performed a national audit of MM over 2020, with the aim to analyse its numbers, characteristics, and causes. We used data of local and regional hospitals where EU/PIMI-II was operating. These hospitals showed lower MMR than previous national figures; however, the exclusion of the main obstetrical referral hospitals, and the unknown number of community-based deliveries make it difficult to compare. Guinea-Bissau still faces enormous challenges in reducing MM. Despite the slow progresses, this study gives us hope, as EU/PIMI-IÍs interventions appeared to have a positive impact in MM reduction.
Introduction
Maternal mortality (MM) is defined as ‘the death of a woman while pregnant or within 42 days of termination of pregnancy’. 1 Of all MM, 75% is due to haemorrhage, infection, (pre-) eclampsia, complications from childbirth and unsafe abortion, which are all preventable and treatable causes. 2 Poverty, illiteracy, cultural beliefs, poor quality and accessibility of health services, negatively influence pregnancy outcomes.3,4 Globally, 9.2% of women in reproductive age die due to pregnancy-related causes, 94% of the MM burden is in low- and middle-income countries (LMICs), and 66% are recorded in Sub-Saharan Africa.1,2 A 35% global MM reduction has been seen since 2000; nevertheless the MMR was still unacceptably high: 211/100,000 live births. 1 In Guinea-Bissau, there was a 45% MMR reduction, from 1210 to 667/100,000 live births.1,4,5
In the last two decades, the Millennium/Sustainable Development Goals (MDG/SDG) set specific targets to reduce the global MMR to 70/100,000 live births by the end of 2030, meaning that each country should reduce by two-thirds their 2010 baseline. 3 In Guinea-Bissau, several projects have been addressed to achieve this, such as the National Plans for Sanitary Development (PNDS), the National Operational Plan to Accelerate Child and Maternal Mortality Reduction (POPEN), and the European Union Integrated Programme to Reduce Maternal and Infant Mortality (EU/PIMI). EU/PIMI was the largest programme established in the country and consisted of two phases (EU/PIMI-I: 2013–2016 and EU/PIMI-II: 2017–2021), implemented by three different partners: Instituto Marquês Valle Flôr (IMVF), United Nations Children's Fund (UNICEF) and Entraide Médical Internationale (EMI). IMVF focused on staff trainings and human/material resources support; UNICEF was responsible for the community healthcare; and, EMÍs concern was to cover health expenditures (by providing free consultations, ambulances, and rewards for proper diagnosis/medical treatments - e.g. obstetric ultrasounds and Caesarean sections), owing to the increase in out-of-the-pocket costs (32% to 75%) and decrease in health investments made by the Government (50% to 9.2%), between 2000 and 2018. 6
Guinea-Bissau scores very low in the Human Development Index, as well as the Gender Inequality Index, which strongly influences maternal health.1,4,7,8 Guinea-Bissau is considered, together with Sierra Leone and Guinea, a ‘MM hotspot’ in West Africa, with an insignificant MM annual reduction rate of 3.5% between 2000 and 2017.1,9 It has even been reported that maternal deaths (MD) increased in Guinea-Bissau, 7 between 1996 and 2000; mainly owing to civil war, a meningitis epidemic and the general political instability in the country. 10
No recent information has been published on MMRs in Guinea-Bissau. Therefore, taking advantage of the available EU/PIMI-II data collection, we performed a nationwide audit of MD over 2020, in order to analyse its numbers, characteristics, and causes.
Methods
A national audit was performed, using a retrospective observational design, to analyse the data, characteristics and determine the MD causes. Our study was conducted in 132 local and regional hospitals, where EU/PIMI-II was operating. These facilities were distributed over eleven regions: East (Bafatá, Gabu), South (Quínara, Tombali, Bolama, Bijagós) and North (SAB-Autonomous Sector Bissau, Cacheu, Oio, Farim, Biombo). EU/PIMI-II was not operational in the two major national referral hospitals in SAB – the Hospital Nacional Simão Mendes and the Military Hospital- and in the private facilities, for that reason they were not included in this study.
We used the WHO definition of MM to collect the data. 1 The relevant MM information was gathered by EU/PIMI-II staff, through monthly reports, using delivery books, MD reports, clinical files, partographs and surgical notes (see Table 1). Microsoft Excel was used to organise the data, over a one-year period (from January-December 2020), using MMR as our main outcome measure. Data analysis was done using SPSS. We used the new International Classification of Diseases-Maternal Mortality (ICD-MM) 11 to cluster the causes of death, taking into consideration that the causes of death were not clearly defined prior to their registration. For the sake of comparison, we also included information of 2018–2019.
Variables collected and used for characterization of maternal deaths, Guinea-Bissau (2020).
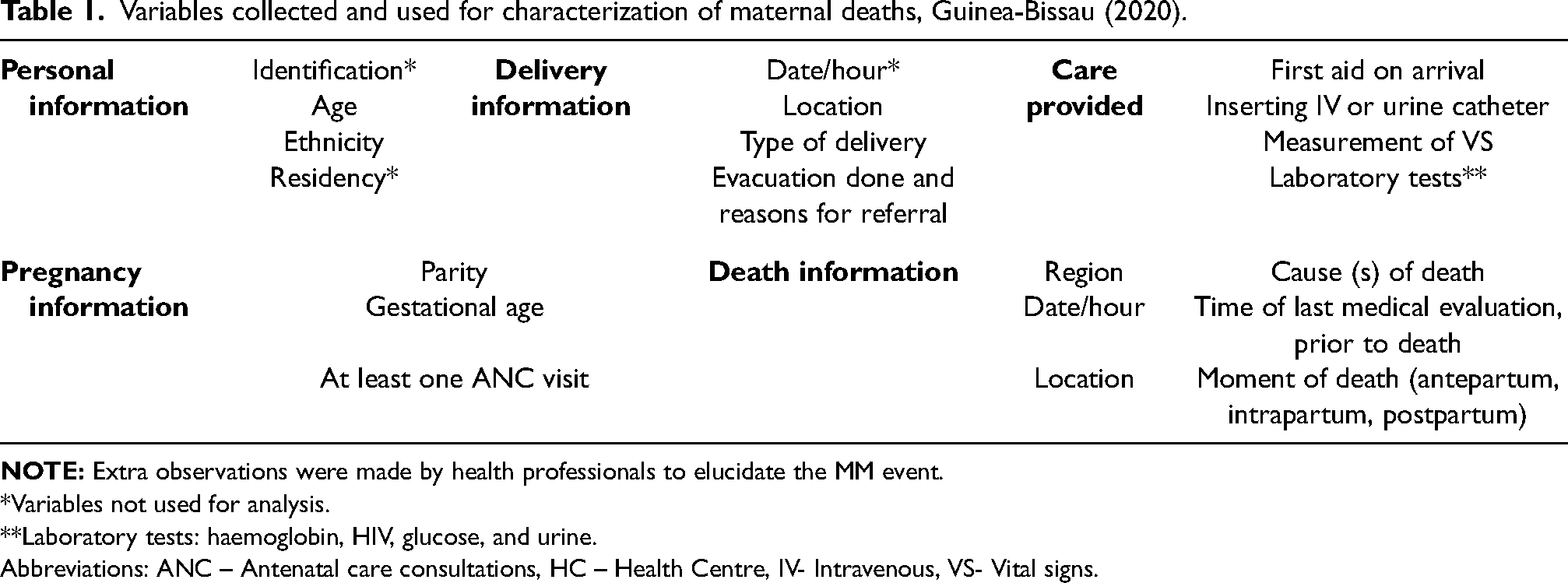
*Variables not used for analysis.
**Laboratory tests: haemoglobin, HIV, glucose, and urine.
Abbreviations: ANC – Antenatal care consultations, HC – Health Centre, IV- Intravenous, VS- Vital signs.
Ethical considerations
No individual patient questionnaires were conducted. An agreement was signed, between the Bissau-Guinean Ministry of Health and EU/PIMI-II, for collection, analysis, and publication of the available data.
Results
In total, 23,443 live births and 79 MD occurred in EU/PIMI-IÍs facilities during 2020, which gives a MMR of 337/100,000 live births. EU/PIMI-II stimulated the discussion of every MD at a local and regional level, with the purpose of improving the quality of care. In 2018 and 2019, there were four less deaths, and a MMR reduction of 26% (455/100,000 live births) and 16% (403/100,000 live births), respectively. Table 2 shows the main characteristics of MD.
Characteristics of maternal deaths (2020), absolute (n) and relative (%) frequencies. Total n = 79.
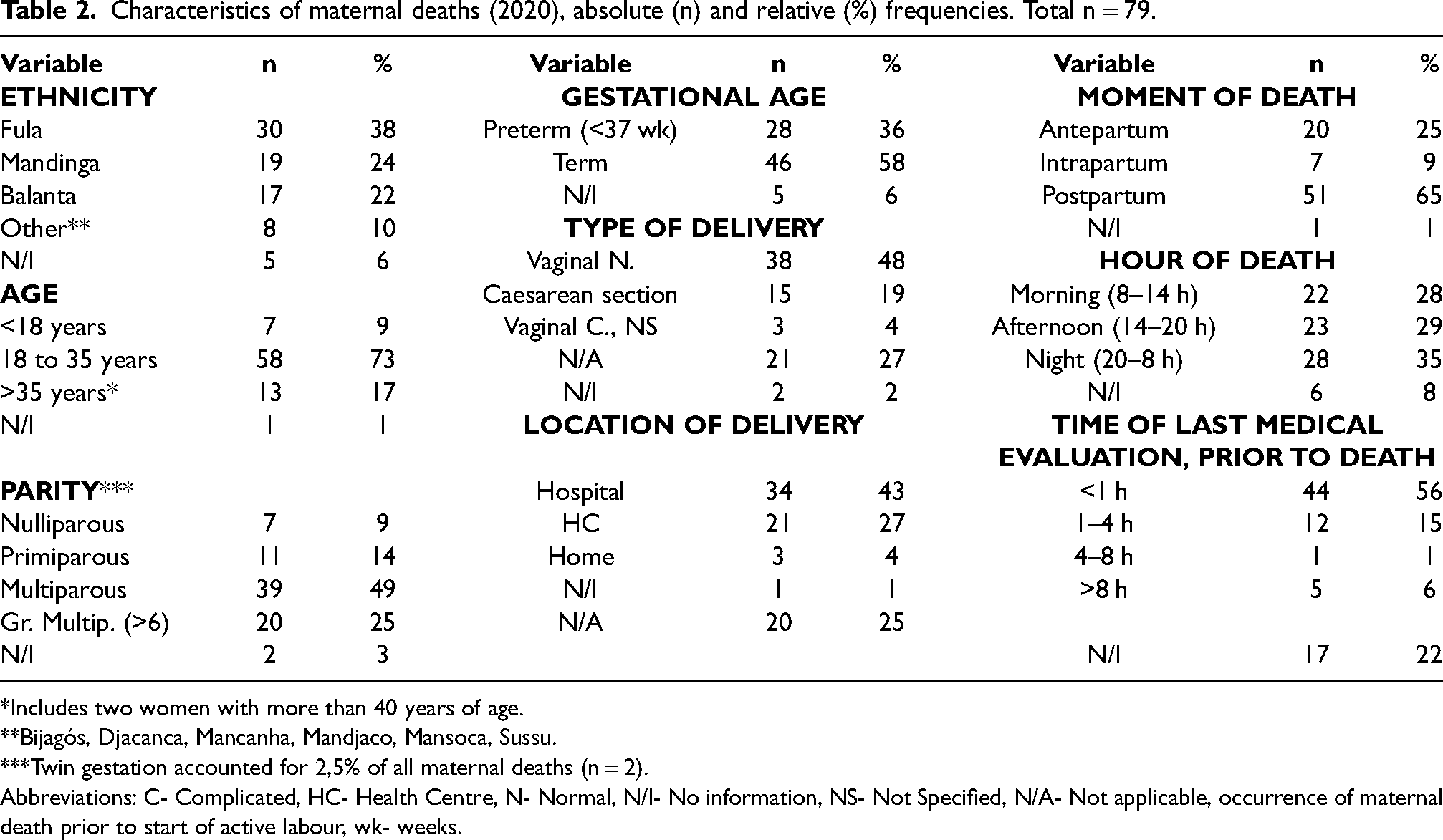
*Includes two women with more than 40 years of age.
**Bijagós, Djacanca, Mancanha, Mandjaco, Mansoca, Sussu.
***Twin gestation accounted for 2,5% of all maternal deaths (n = 2).
Abbreviations: C- Complicated, HC- Health Centre, N- Normal, N/I- No information, NS- Not Specified, N/A- Not applicable, occurrence of maternal death prior to start of active labour, wk- weeks.
When analysing the data per regions, the numbers of MD were higher in the Eastern region (Bafatá n = 21 and Gabu n = 18), Oio (n = 12) and Tombali (n = 11), while the remaining regions accounted for 2–5 deaths per region, giving a total of 16 deaths. SAB (n = 0) and Biombo (n = 1), were exceptions owing to their close location with the main reference hospitals. However, when looking at MMR, the Southern region scored the highest (MMR = 1905 Bolama, MMR = 610 Quínara, MMR = 488 Bijagós, MMR = 462 Tombali). The rest of MMR was: Oio = 412, Gabu = 347, Farim = 210, Cacheu = 154, Biombo = 95 and SAB = 0. Overall, since 2018 the Eastern region showed improvements, while the Southern region numbers deteriorated over time. In terms of seasonality, most MM occurred between November-April, with one peak in July; in terms of MMR, a gradual increase per trimester was seen.
In 71% of women, basic care was provided at their arrival, 77% had their vital signs checked and 89% had the required laboratory tests done. The following observations were made by health professionals regarding MM cases: 22% had severe anaemia; 6% unavailability of blood for transfusion; 14% incidence of (pre-) eclampsia; and 30% arrived late to the health facility or no ambulance was available for evacuation. The suspected or reported causes of death are shown in Table 3. In 35 (44%) of MM, women were transferred from another facility; of those, only 4% had no evacuation report (n = 3).
Reported/suspected primary cause of maternal death (md).

*Diagnosis made and described by different health professionals in the field (doctors, midwives, or nurses).
Discussion
Despite the progress made in reducing MM, Guinea-Bissau is still far from reaching their SDG in maternal health.1,3,7 Guinea-Bissau is one of the poorest countries in the world, with a fragile healthcare system in place. Over the last decades, the country has faced an unstable political and economic scene, thus ‘deciding to seek care, reaching care in time and receiving adequate treatment’ 12 is not always a given for local women. Their ‘low status in society, persistent high fertility rates, low levels of contraceptive use, and early marriage and pregnancy’ 13 in combination with poverty and illiteracy, put these women in a precarious position. They have no say about their health, and normally depend on their husband′s decision to seek proper healthcare,8,14 as ‘power and authority remain with them as heads of the family’. 15 Bissau-Guinean women tend to have at least four children. 16 The overall contraceptive prevalence rate has remained low (14% in 2014, 20,2% among married women in 2018–2019), regardless of numerous family planning campaigns. Some 95% of sexually active women (15–24 years) do not use contraceptives, because of lack of knowledge and because of their partners' disapproval.8,14 Misdiagnosis and/or mistreatment of obstetric pathology by traditional birth attenders (TBA) has also been an important factor for delay in seeking effective healthcare, increasing their risk of MM. 17 TBAs continue to be the first contact point in the community, especially because of the poor accessibility to regular healthcare (lack of trained staff and material resources).14,15 EU/PIMI-II tried to create a link between the community and health centres,7,15,18 by implementing a community health worker programme (CHWP), as other countries successfully did. 19 However, Guinea-Bissau has a weak voluntarily-based CHWP in place, since the Government has struggled financially to support it.15,20 The emergence of the COVID-19 pandemic and persistent national strikes held since 2019, also strongly influenced the behaviour of women to seek care, as well as the quality of care they received. These events could explain the slight rise in MMR throughout 2020. During this period, EU/PIMI-II staff continued providing emergency obstetric care, however only as a temporary solution. In March-April we observed a peak in MM, which coincided with the period around the cashew nut campaign. Women were expected to work fulltime on their main income source, which meant they were impaired from attending regular and emergency obstetric care during that period of the year. However, further evaluation would be necessary to establish a distinct relationship between this and MM. The same could be said about ethnicity and MM.7,15 Our findings suggested that most MM were among Fulas and Mandingas. These ethnic groups have more obstetric complications owing to their slender stature and the persistent illegal practise of female genital mutilation (FGM) (found to be present in 45–50% in 2014).4,8,21 A specific link between FGM and MD has not yet, however, been made. 22 Early polygamous marriages with much older men, and a high HIV prevalence among young women (<25 years) is common in these groups. EU/PIMI-II held sensibilization campaigns about the importance of HIV infection prevention, good practises during/after pregnancy, and about FGM, with the idea of changing misconceptions, cultural practises, and behaviours. One positive finding in our study was improved ANC coverage to 90%. However, many of these women only visited ANC once in their pregnancy, which compares very poorly to the WHO minimum of eight required ANC appointments.13,15,17 This is crucial, since this is the main way to identify risk factors and prevent and treat many complications during pregnancy.12,23
Reaching care in time is also a major problem in Guinea-Bissau, as there is no proper referral system in place, and very few ambulances are available. EU/PIMI-II tried to tackle this problem by developing a referral and counter referral system, arranging new ambulances, providing fuel, improving maintenance of old ambulances, and organizing staff trainings about identification of emergency evacuations and its safe procedure. A positive finding in our study is that almost half the women transferred possessed an evacuation guide, of whom 27 (34%) had an accurate initial diagnosis made. Most women had laboratory tests done, had an intravenous catheter in place and had a clinical record, which is not always a given fact in Guinea-Bissau. 13 Reaching care on time is a challenge in Guinea-Bissau, because the road infrastructure is of very poor quality. In July we noted a peak in MM, which coincided with the rainy season, when road conditions deteriorate, and malaria is at its peak.16,20,24 Also geographical location, residing >25 km from the hospital, increased the MM odds ratio to 7,4.9,22 More than half of the Bissau-Guinean population lives >5 km from a health facility, impacting accessibility and affordability of healthcare for many women. 15 The Eastern region is one of the most isolated and dispersed areas in the country. Gabu and Bafatá reported the worst MM numbers, coinciding with previous publications.7,22 Despite these maternal health indicators, progresses have been noted in this region since EU/PIMI-II′s implementation. Another successful strategy implemented to improve poor health accessibility are the Maternity Waiting Homes. Here, women can stay for free, based on their pregnancy risk or the distance to their homes.8,14 Now, there are houses fully functioning (Bafatá, Cacheu, Bolama and Tombali), with new ones emerging.
Receiving adequate care has been the focus of improvement in Guinea-Bissau, where ‘poor birth practises, inadequate referral mechanisms and poor emergency obstetric care’ 15 are a constant reality. In 2018, only 45% of births in Guinea-Bissau were attended by a skilled professional and only two doctors per 10,000 people were available.4,13 The lack of personnel may explain the reduced monitoring during night-time, and consequently be the reason why most mothers in our study died during the night, though 56% of women were reviewed one hour prior to their deaths. Also, most of our MD occurred during the post-partum period and in a hospital setting, which coincides with studies in LMICs and richer countries.18,22,25 Our findings were solely based on hospital registrations, considering that community records were inexistent. Most women presenting to our facilities for delivery were previously identified as high-risk obstetric cases and were already advised to deliver in the hospital. Also, the most critically ill were more likely to get transferred to a hospital. Overall, no direct causal relationship can be made for the higher in-hospital MM.7,22 To improve the quality of healthcare patients receive, EU/PIMI-II′s main goal was to improve capacity building (in obstetrics, paediatrics, surgery, and anaesthesia). We believe this has been the most sustainable and efficient strategy to reduce MM in Guinea-Bissau. It has been argued that The Safe Motherhood Initiative lacks a clear and concise strategy to reduce MM. 24 Obstetrics is unpredictable, and complications during pregnancy and childbirth will always occur. Therefore, the solution to a significant reduction in MM lies in having facilities ready to treat emergency obstetric complications. 24 EU/PIMI-II goes in line with this idea by applying different strategies including building and improving infrastructure (e.g. theatre rooms and blood transfusion units), provision of new hospital materials and machines and delivery of free medication.
When looking at the personal characteristics of MM, most were among women between 18 and 35 years old, after a non-complicated term delivery.
The lack of blood for transfusion is obviously important. Many locals believe it is unnatural to donate blood, 15 a predominant idea among the Fula. Successful interventions have been implemented by EU/PIMI-II, through restoration, material supply and building of transfusion units. However, not all of them were used efficiently, owing to low community adherence. Schools, churches, and the military are more apt to donate blood.
The MMR has improved compared to previous years. However, the actual MMR may be under-reported, since many deaths occurred in the community, without ever being reported to a health facility. Furthermore, the exclusion of the central and private sector in our study, as well as the differences in MM registration between projects implemented in the country make the total figures unreliable. As Guinea-Bissau lacks a proper central registration system, we were not able to have a complete overview of the current situation, thus making a proper comparison difficult. Although our study does not reflect the full picture of MM, our findings are useful, as other reports have mentioned a much higher MMR between 667–900/100,000 live births.1,10
Limitations
With respect to data collection, some variables should have been included for a better interpretation of the MM characteristics, for example: distance residency-health facility, amount of ANC′s done, results of ultrasound and diagnostic tests, blood transfusion information, hour of hospital admission, duration of labour and information and causes on foetal death. For a better understanding of the overall maternal situation, socio-economic factors such as early marriage, literacy, and presence of FGM, are missing. Nonetheless despite the poor quality and quantity of much of our data, our conclusions are, we believe, sound.
Conclusion
Our recommendation would be to implement an official MM audit. By knowing the pitfalls, it is easier to target the main problems and support health professionals and policy makers to improve the quality of maternal health care. Therefore, a complete overview is needed, through a vital registration system, which includes the main reference hospitals and the community level.
Footnotes
Acknowledgements
We acknowledge the cooperation of IMVF′s obstetric and paediatric health professionals at a regional and local level. Without their support and arduous work, it would have been impossible to gather the information for this manuscript. We also want to thank F. Fernandes, head of EU/PIMI-II′s statistics department, for his aid in data acquisition and organization.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.