
Abstract
Acute copper sulphate poisoning is associated with multi-organ failure and high mortality. Patients typically present with gastrointestinal symptoms, haemolysis, methaemoglobinaemia, acute liver injury, rhabdomyolysis and renal failure. Management is usually supportive, and the role of chelation therapy has not been established. Copper is not dialysable. Plasmapheresis has been shown to remove protein-bound copper, reducing plasma and intracellular concentrations. We present a case of severe copper sulphate poisoning, who did not improve with chelation therapy with D-penicillamine and supportive care, but with therapeutic plasma exchange (four cycles) showed rapid clinical recovery.
Case report
A 28-year old male was admitted after ingesting copper sulphate (approximately 50 g) for the purpose of self-harm. Immediately following the ingestion, he had multiple episodes of bluish-green coloured vomiting along with epigastric pain and loose stools. Within 12–24 h, he developed jaundice, passing dark cola-coloured urine. He was previously healthy and did not smoke or take illicit drugs. On admission, his pulse was 110 per minute, blood pressure 120/70 mm Hg, respiratory rate 26 per minute and oxygen saturation 98% on ambient air. He was initially managed with intravenous fluids, ondansetron, and pantoprazole. Upper gastrointestinal endoscopy revealed moderate to severe corrosive injury (Zarger's grade 2–3) in the pharynx, oesophagus, stomach, and duodenum. A naso-jejunal tube was placed endoscopically for nutrition.
There was no evidence of methaemoglobinaemia (serum methaemoglobin 0.9%) nor rhabdomyolysis (creatinine kinase 1.13 µkat/l). However, he developed a rapid fall in haemoglobin (nadir value, 72 g/L), progressive hyperbilirubinaemia (peak value, 817.4 µmol/L), elevated liver transaminase levels (aspartate transaminase more than alanine transaminase), and acute kidney injury (Table 1). Further investigation for haemolysis revealed elevated free plasma Hb (2.43 g/L, range 0.0–0.15) and the presence of fragmented red blood cells and polychromasia on a peripheral smear. A qualitative screening test detected glucose-6-phosphate dehydrogenase (G6PD) deficiency.
Trend of laboratory features showing the development of haemolysis, acute liver injury and acute kidney injury in copper sulphate poisoning and subsequent recovery with plasmapheresis (started on day 5 of poisoning).
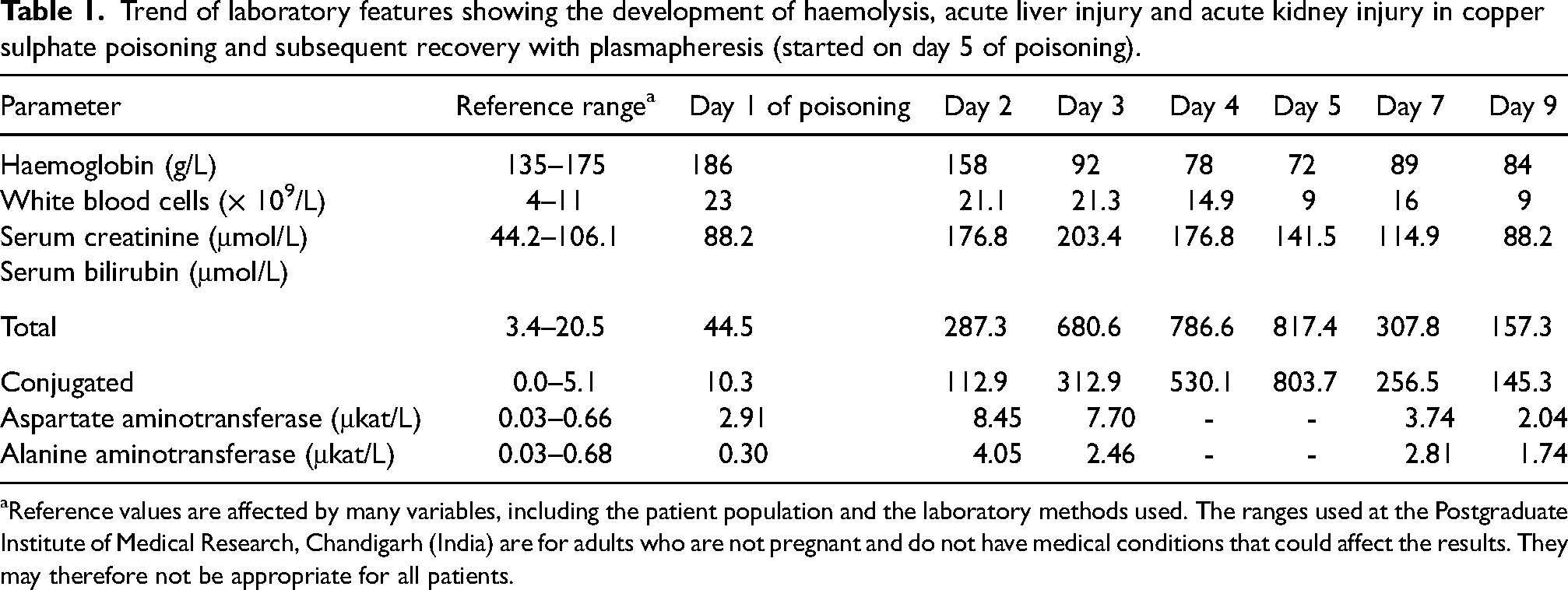
Reference values are affected by many variables, including the patient population and the laboratory methods used. The ranges used at the Postgraduate Institute of Medical Research, Chandigarh (India) are for adults who are not pregnant and do not have medical conditions that could affect the results. They may therefore not be appropriate for all patients.
Our patient received D-penicillamine as chelation therapy and packed red cell transfusion. However, he progressively became drowsy with oxygen desaturation. Thus, a therapeutic plasma exchange was commenced on the fifth day. Following this, he showed a rapid clinical improvement with cessation of haemolysis and improvement in liver and renal function (Table 1). Four cycles of plasmapheresis were administered before discharge.
Discussion
Copper sulphate has long been used in agricultural communities for its germicide, pesticide, feed additive, and soil additive actions. It is generally available as powder or in crystal form. Poisoning is mainly reported from South Asian countries and uncommonly in the western world.1–5 Acute consumption of 1 g usually results in clinical toxicity in adults, and 10–20 g is estimated to be lethal. 2 A high concentration of copper ions depletes cellular glutathione stores with subsequent production of reactive oxygen species, leading to oxidative stress and membrane toxicity in red cells, hepatocytes, myocytes, and other cells.1,3
The main features of the toxidrome are haemolysis and methaemoglobinaemia.1–4 Persons with G6PD deficiency are at increased risk of oxidant stress. Owing to their reduced glutathione stores, they are usually more prone to haemolysis than methaemoglobinaemia. 6 Other typical features of severe poisoning include prominent gastrointestinal symptoms through corrosive injury after acute ingestion, acute liver injury and acute kidney injury, the latter through direct toxicity, haemolysis, rhabdomyolysis and hypovolaemia.1–4
Management of copper sulphate poisoning consists of supportive care and detoxification. The former may include red cell transfusion for acute haemolysis or gastric bleeding, oxygenation or ventilation for methaemoglobinaemia, endoscopic placement of a nasojejunal tube for nutrition and intravenous fluid for rehydration.1–4 Methylene blue remains the antidote for methaemoglobinaemia. 6 Although clear evidence of a clinical benefit does not exist, chelating agents are commonly used in severe toxicity. D-penicillamine or dimercaprol are preferred agents, either singly or together, followed by dimercaprol and calcium disodium EDTA.1–4,7 Chelation therapy should be guided by plasma copper level monitoring; this may, however, not be readily available, as in our case. The presence of vomiting and acute kidney injury may further limit the use of chelators.
Enhanced elimination with haemolysis is not recommended because of the large volume of distribution and the high plasma protein binding of copper ions.1–4,7 The potential usefulness of plasmapheresis has been documented in refractory cases that do not respond to chelation or supportive measures. It removes protein-bound copper, reduces plasma and intracellular copper concentrations, and thus prevents further organ injury. 7 Case reports have also demonstrated its usefulness when combined with exchange transfusion. 7
Footnotes
Author contributions
JAS: collected patient data, drafted the manuscript, patient management. AK, LT: collected patient data, patient management. SS, 5RH: patient management. AKP: collected patient data, drafted and revised the manuscript, patient management.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was gained after full explanation concerning confidentiality, and that the case information will be used for education purposes only.