
Abstract
Linezolid-induced lactic acidosis is a rare, but life-threatening complication of a commonly used drug. Patients present with persistent lactic acidosis, hypoglycaemia, high central venous oxygen saturation and shock. Linezolid causes mitochondrial toxicity due to impaired oxidative phosphorylation. This is evidenced by cytoplasmic vacuolations in the myeloid and erythroid precursors of bone marrow smear as illustrated in our case. Discontinuation of the drug, administration of thiamine and haemodialysis reduces lactic acid levels.
Case presentation
A 50-year-old male patient, known to have extra-hepatic portal vein occlusion, a splenorenal shunt following splenectomy, and a hepato-jejunostomy for biliary stricture with percutaneous transhepatic biliary drainage for recurrent cholangitis, presented with diffuse abdominal pain, loss of appetite and reduced urine output of two weeks’ duration. He was diagnosed with multi-drug resistant pulmonary tuberculosis (MDRTB) two months previously and had been put on an oral regime of bedaquiline, levofloxacin, linezolid, cycloserine, clofazimine and pyridoxine.
At presentation, he was drowsy, dehydrated, hypoglycaemic and hypotensive (BP 88/50 mm Hg) with a kissing inferior vena cava seen on ultrasonography. His central venous oxygen saturation was 90%, despite shock. Initial laboratory parameters revealed an anaemia (Hb 61 g/l), thrombocytopenia (60 × 109/l) and elevated creatinine (141 µmol/l) and severe lactic acidosis (8.8 mmol/L) on arterial blood gas analysis.
With a clinical suspicion of septic shock, intravenous fluid resuscitation and broad-spectrum antibiotics were commenced. Nonetheless, raised lactate levels persisted. Screening with urine, sputum and blood culture proved negative. A chest radiograph was normal. An infection could not adequately be ruled out, and thus empirical antibiotics were commenced. Though shock improved, lactate levels were persistently high. These with very high central venous oxygen saturation prompted us to consider drug-induced mitochondrial toxicity. We, therefore, stopped linezolid, which we considered to be the most likely culprit drug.
His shock improved but lactate was persistently high. High lactate with very high central venous oxygen saturation prompted us to consider drug-induced mitochondrial toxicity. We stopped linezolid which we considered to be the culprit drug. High-dose thiamine and two sessions of hemodialysis were provided. A bone marrow examination done as a part of a workup for cytopenia revealed reactive changes with cytoplasmic vacuolations in myeloid and erythroid precursors classical of mitochondrial toxicity, most probably due to linezolid (Figure 1).
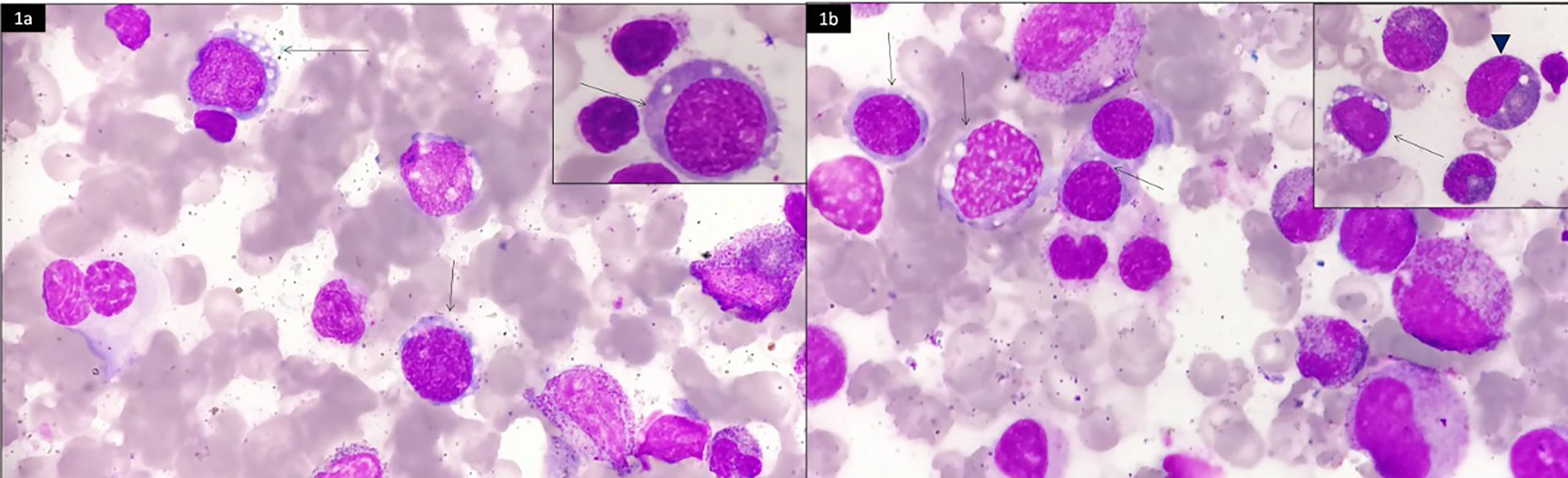
Bone marrow aspiration smears showing multiple erythroid precursors with cytoplasmic vacuolisation (marked with arrows). Inset in (b) shows cytoplasmic vacuolations in a myelocyte (marked with arrowhead). Vacuolisation was more pronounced in early erythroid precursors (Jenner-Geimsa X 1000).
Discussion
Linezolid has been given the status of a Group A drug in the WHO classification and is one of three drugs to be compulsorily included in oral longer regimes for MDRTB. However, significant dose-dependent side effects such as peripheral neuropathy, anaemia, thrombocytopenia and optic neuropathy have limited its use. 1 We add to this list a life-threatening complication of linezolid-induced lactic acidosis (LILA).
Linezolid inhibits protein synthesis by binding to a site on the bacterial 23S ribosomal RNA of the 50S subunit, thus inhibiting protein synthesis. A conserved equivalent binding domain is also present on mammalian 16S rRNA which causes disruption of mitochondrial protein synthesis. As mitochondria are important in oxidative phosphorylation by the Krebs cycle and gluconeogenesis, mitochondrial damage can lead to lactic acidosis and hypoglycaemic episodes. Our patient had high central venous oxygen saturation despite being in shock indicating a possible mitochondrial injury. Non-specific mono-amine oxidase inhibition and direct pancreatic damage due to linezolid could be other possible explanations for its induced hypoglycaemia. 2
The incidence of LILA was found to be 6.8% with duration of treatment of >6 weeks. 3 Elderly age, male sex, renal and liver disease are other risk factors. 4 A decreased clearance of lactic acid in the liver can be explained in our patient who had portal biliopathy and a splenorenal shunt in place. Further, a high dose of thiamine and sessions of haemodialysis might have augmented the clearance of lactic acid in our patient.
A systematic review of 35 articles including 47 cases of LILA revealed a high mortality of 25.5%. 5 With adoption of oral regimes for MDRTB, more patients are likely to be exposed to extended duration of linezolid in out-of-hospital settings. Our case highlights the importance of early recognition and treatment of linezolid-induced side effects.
Footnotes
Authors’ contribution
All authors were involved in patient care. VCK, KS, TPK and RKM wrote the first draft of the manuscript. JD was involved in reviewing the bone marrow slides and provided the images. PS and JD suggested final revisions to the manuscript. All authors read and agreed to the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
An informed consent was obtained.