
Abstract
A 72-year woman with a history of multiple cerebrovascular accidents presented with severe epigastric pain. An oesophageal perforation by the tip of a Ryles tube, which had migrated into the mediastinum, was diagnosed by radiography. An attempt at pushing the nasogastric tube into the stomach resulted in increasing the rupture to about 6 cm in size. Replacement by a triple-lumen nasojejunal feeding tube and subsequent feeding with c.1,400 calories per day enabled the perforation to close without further intervention.
Introduction
Oesophageal perforation has a reported incidence of 3.1 per million per year. 1 The oesophagus lacks a serosa, and hence is more susceptible to rupture, resulting in mediastinal contamination. Chest radiography may reveal mediastinal emphysema or a pneumothorax suggestive of oesophageal perforation. Many need surgical intervention, but some may benefit from non-operative endoscopic measures. 2
Short report
A 72-year old tracheotomised female with known cerebral impairment from repeated cerebrovascular accidents over the previous 12 years, the last being 1 year before, had been maintained on nasogastric (NG) feeds.
She had suffered aspiration pneumonia six months prior and weighed <40 kg. She had undergone a routine change of the NG tube at another hospital. Afterwards, she complained of severe epigastric pain and thus underwent chest radiography, which showed the tip of the NG tube in the mediastinum. This was confirmed on a computed tomography (CT) scan, which showed the lower end of the tube exiting the lower third of the oesophagus at the level of D9 laterally into the posterior mediastinum, with its tip upturned and abutting the aorta. A pneumomediastinum and a small left pleural effusion were noted. A small left pneumothorax was also seen. She was transferred to our hospital for further management.
She was anaemic (Hb 107 g/L), hyponatraemic (Na+ 133 mmol/L), with a leucocytosis of 19.1 × 109/L (neutrophils 86.9%), normothrombocythaemia (150 × 109/L) and raised C-reactive protein at 24 mg/dL. She was hypocalcaemic (1.95 mmol/L), with raised creatinine of 0.111 mmol/L, coagulopathy (international normalised ratio 1.16), and protein deficiency (serum albumin 31 g/L) and total protein of 57 g/L.
Upper gastrointestinal endoscopy was performed under intravenous propofol. The previously placed Ryles tube (RT) was coiled and present in the mediastinum with a visible tear in the lower oesophagus. Using a rat-tooth alligator jaw grasping forceps (FG-47L-1, Olympus, USA), it was retracted and attempts made to push it into the stomach, but this increased the oesophageal tear, which reached a size of 6 cm. The NG tube was therefore removed with an endoscopic snare (SD-221L-25, Olympus, USA). A triple-lumen nasojejunal (NJ) feeding tube (16F,150 cm, Freka Trelumina, Fresenius Kabi, Germany) was then repositioned carefully (Fig. 1, panels 1a–1f). No further intervention was contemplated due to the patient's age and co-morbidity.
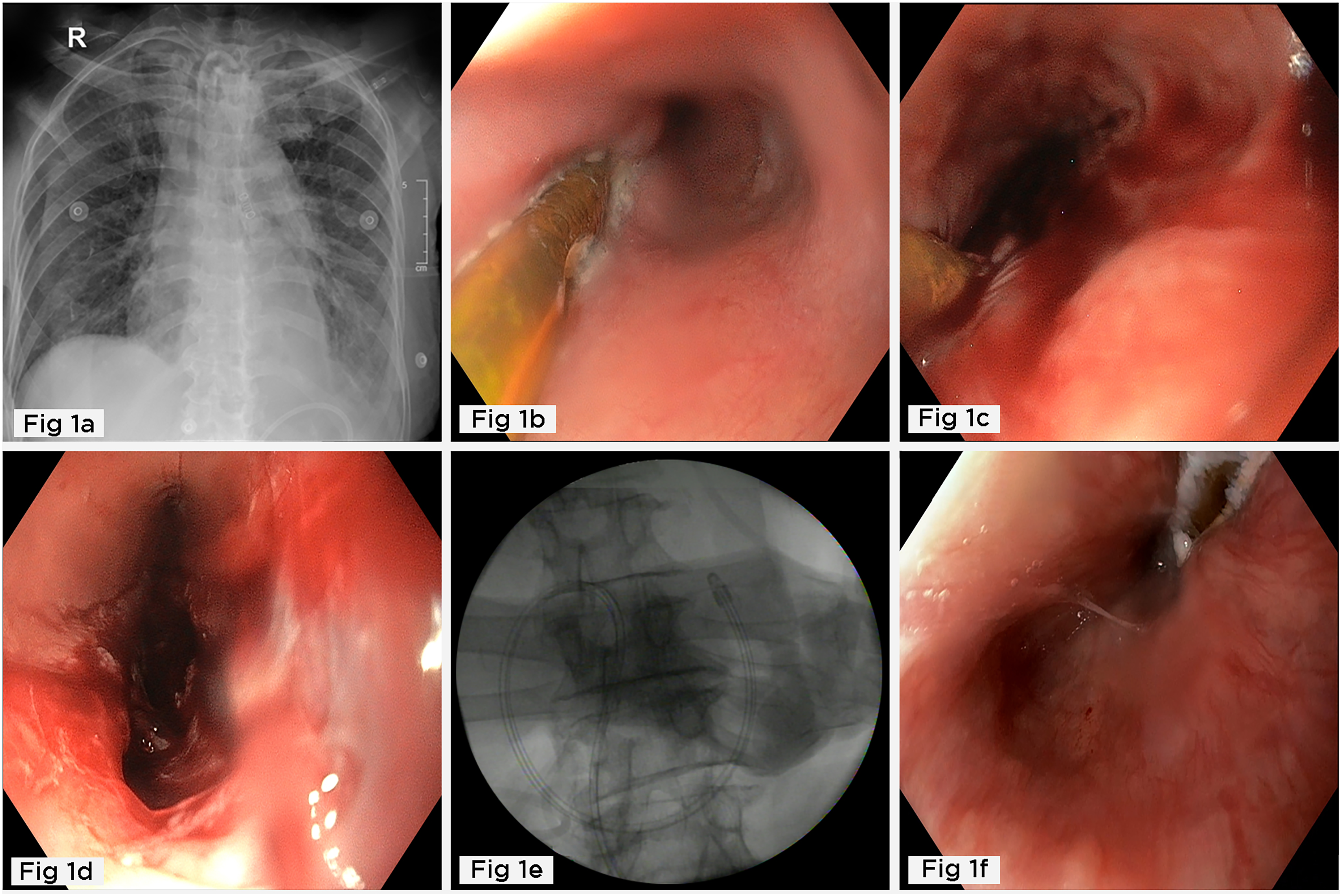
(a) Radiograph showing the tip of Ryles tube in the mediastinum. (b) and (c) Endoscopy showing Ryles tube in the lower third of oesophagus. (d) Endoscopy showing oesophageal perforation after removal of Ryles tube. (e) Fluoroscopy showing nasojejunal tube in the jejunum. (f) Follow-up endoscopy showing sealed oesophageal perforation.
Her urine and tracheostomy tube culture grew Pseudomonas aeruginosa (pan-sensitive); so she was started on meropenem (1 g IV tds for 5 days). She developed thrombocytopenia (platelet count: 93 × 109/L), so the antibiotics were changed to Piperacillin and Tazobactum (4.5 g IV tds, from the sixth day onwards). NJ feeds with 1400 calories per day (Peptamen, 60 mL/h) were given with correction of a subsequent refeeding syndrome with potassium phosphate for 5 days.
Chest radiography showed no degradation. Our patient could be stabilised and discharged with physiotherapy and rehabilitative care during her stay. At follow up, six weeks later, she underwent a repeat endoscopy, which showed that the oesophageal perforation had sealed. The NJ tube was left in situ as she tolerated this feeding well.
Discussion
A long-stay NG tube may lead to complications, as the oesophageal mucosa becomes irritated by the presence of a constant foreign body, leading to ulceration and, ultimately, perforation, resulting in mediastinal contamination, which is rapidly fatal.
A high level of suspicion, especially shortly after insertion of the NG tube in such circumstances, is needed. Fluoroscopy is the best tool for initial assessment of its position. A chest radiograph may be equivocal. Malpositioning of an RT is best confirmed by CT scan, which can check the size and position of the defect and any resulting collection. A delay of > 24 h in diagnosis and therapy is associated with high mortality. 3
The NG tube may accidentally enter the trachea, coil in the oesophagus, perforate the oesophagus, and develop a retropharyngeal abscess. Critically ill patients, especially those with neurological diseases and poor intake, need enteral nutrition, preferably by the NJ tube. This is preferred to an RT since the former is thinner, has a flexible tip, is better tolerated, and delivers food directly to the jejunum.
RT feeds which are rich in calorie content may have delayed gastric emptying especially of fats (sometimes 8–10 h). The recumbent lower oesophageal sphincter remains open, which may result in massive regurgitation. Most of the time, this is the reason contributing to aspiration pneumonia. Aspiration pneumonia can be prevented by elevating the head of the bed (45°) and oral decontamination. 4
Oesophageal perforations are best dealt with through minor intervention. Most defects may need to be tackled by endoscopy. 5 Small defects may be closed by an overstitch endoscopic suturing system. 6 Oesophagectomy with gastric pull-up is reserved for very large defects or where endoscopic therapy fails.
Many patients with long-stay feeding tubes are malnourished, in a catabolic state with hypoproteinaemia, anaemia, osteoporosis, commonly with vitamin, magnesium and phosphate deficiency. Early hydration and correction of such parameters are essential.
The inflammatory response after perforation is followed by bacterial mediastinitis. Localised infection may be treated with broad-spectrum antibiotics. If a defect is small, it might heal within four weeks, especially in the absence of significant mediastinal contamination, as seen in our case, as she was referred within 24 h.
Conclusions
Patients on ventilators, and unconscious, disoriented or confused may not manifest respiratory distress on false passage of RT. A blind technique of RT placement should thus be avoided, and endoscopic NG tube insertion is preferred.
Replacement of an NG tube where a perforation is suspected or found is fraught with danger.
When available, NJ should be used instead of long-standing NG tube feeding.
A conservative approach may be successful in treating oesophageal perforations.
Early diagnosis and appropriate management are keys to a favorable outcome.
Footnotes
Author contributions
NK contributed to the study concept, manuscript preparation and manuscript review. AV, AM, SP, GP and AD were involved in clinical management of case and manuscript review. AM was involved in critical final review of the manuscript. All authors approved final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.