
Abstract
Can a smart phone application be reliably used for laryngoscopy? This thesis was tested for peri-operative evaluation of vocal cords in patients undergoing thyroid and parathyroid surgery.
Keywords
Introduction
Recurrent Laryngeal Nerve (RLN) injury after Thyroid and Parathyroid surgery has an incidence of 1–3% (permanent nerve palsy) and 5–8% (temporary nerve palsy).1–3 This results in hoarseness, dysphagia and aspiration in the early postoperative period, and bilateral RLN palsy may result in asphyxiation. Hence, early diagnosis of RLN palsy is crucial to avoid such complications. Early recognition of intra-operative RLN injury is key.4,5
Various methods exist: direct laryngoscopy (DL), indirect laryngoscopy (IDL); palpation of the larynx during stimulation of the RLN; laryngeal muscle electromyography and intra-operative neuromonitoring, and transcutaneous laryngeal ultrasonography.3,6–10 However, many of these techniques require availability of an expert, special equipment and additional hospital visits for the patient. DL, considered the gold standard is not available in most low resource settings (LRS).
Methods
Our prospective study was conducted in the Department of Surgery, Netaji Subhash Chandra Bose Medical College, Jabalpur from February to May 2023, and was approved by our Institute Ethics Committee; informed consent was obtained from all patients.
All consecutive patients planned to have thyroid or parathyroid surgery were included in our study, and all underwent examination of the vocal cords in the outpatient department and immediately after surgery in the operation room (OR) using a (AN99 8 mm 2 in 1 USB Endoscope Camera, Inskam, 4017-B37, No.57 Guangda Road, Baoan Community, Yuanshan Street, Longgang District, Shenzhen, China). This is a ‘borescope’ designed for surveying pipes, or equipment underwater or in difficultly accessible places, which can be connected to an Android mobile phone with a free downloadable camera application (inskam). The cost of this device is only 10 USD. [https://www.inskam.com/index.php/Product/view/id/768.html]. Ethylene oxide gas sterilization was used before its reuse in another patient.
Pre-operative assessment of the vocal cords was done in the outpatient department with the app based VC assessment (Fig. 1). Topical xylocaine spray was used and the patient was put in a semi-recumbent position with the neck slightly extended. A single endocrine surgeon (SKY) or a resident doctor (MG) performed all examinations via the oral route. Movement of the vocal cords was graded – Grade I full or normal symmetric movement of both vocal cords, Grade II impaired or decreased movement in one or both vocal cords, and Grade III no movement in one or both vocal cord 11 (Fig. 2).
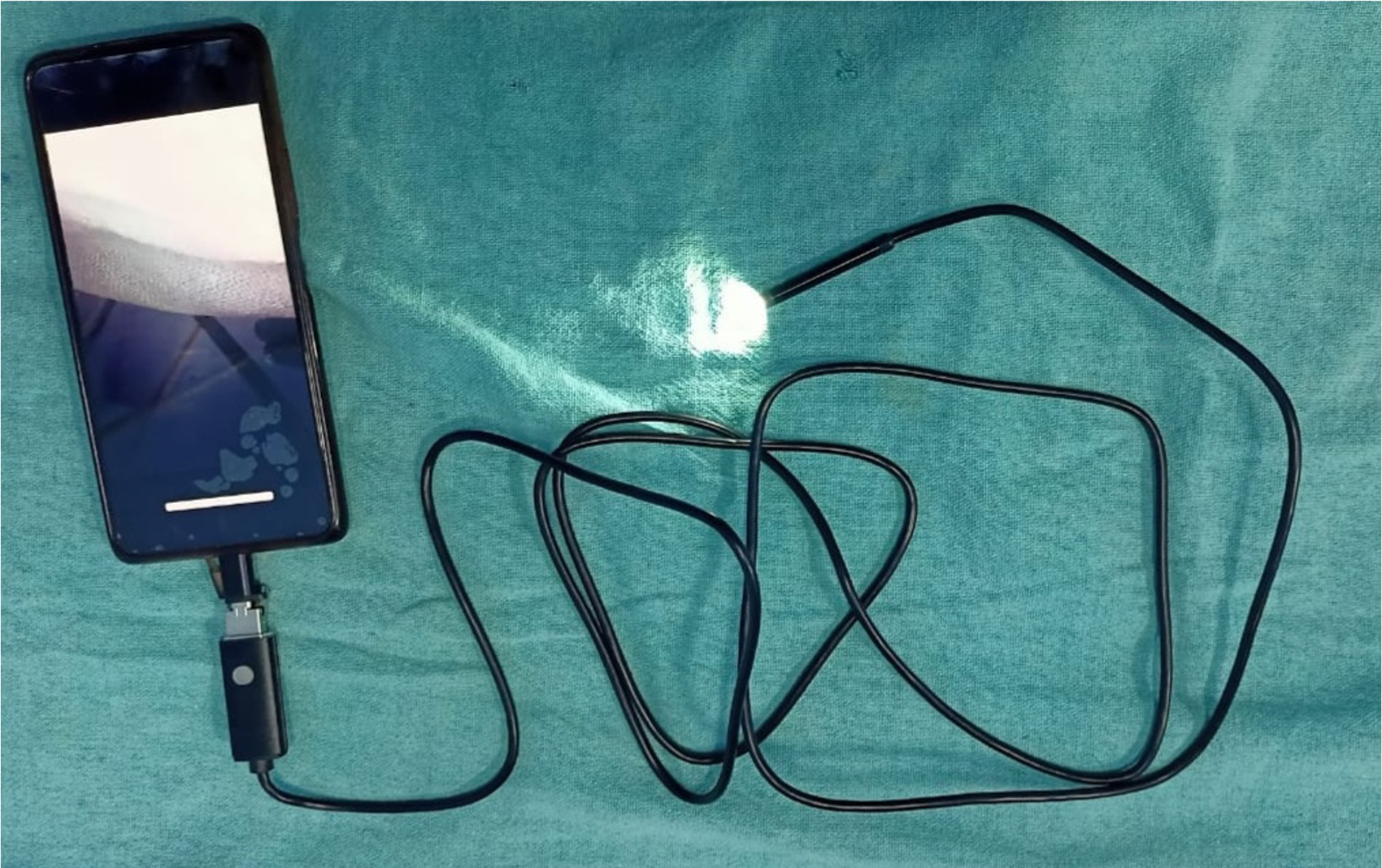
Low-cost device for vocal cord assessment.

Showing vocal cord image visualised and captured with the help of low-cost device.
Post-operative app based VC assessment of vocal cords was performed during or immediately after extubation in the operating room. (Supplementary Video).
Standard direct laryngoscopy via the nasal route was performed in all patients pre-operatively and during follow-up between day 7 and day 10 after surgery. All assessments were done by an experienced laryngologist who was blinded regarding pre-operative or post-operative app based VC assessment results and graded the results as described above; results of app based VC assessment were also compared with the results of IDL.
All patients underwent surgery by a single endocrine surgeon. Visualisation and preservation of the recurrent laryngeal nerves (RLN) was carried out. Intra-operative neuro-monitoring was not used in any patient.
Results
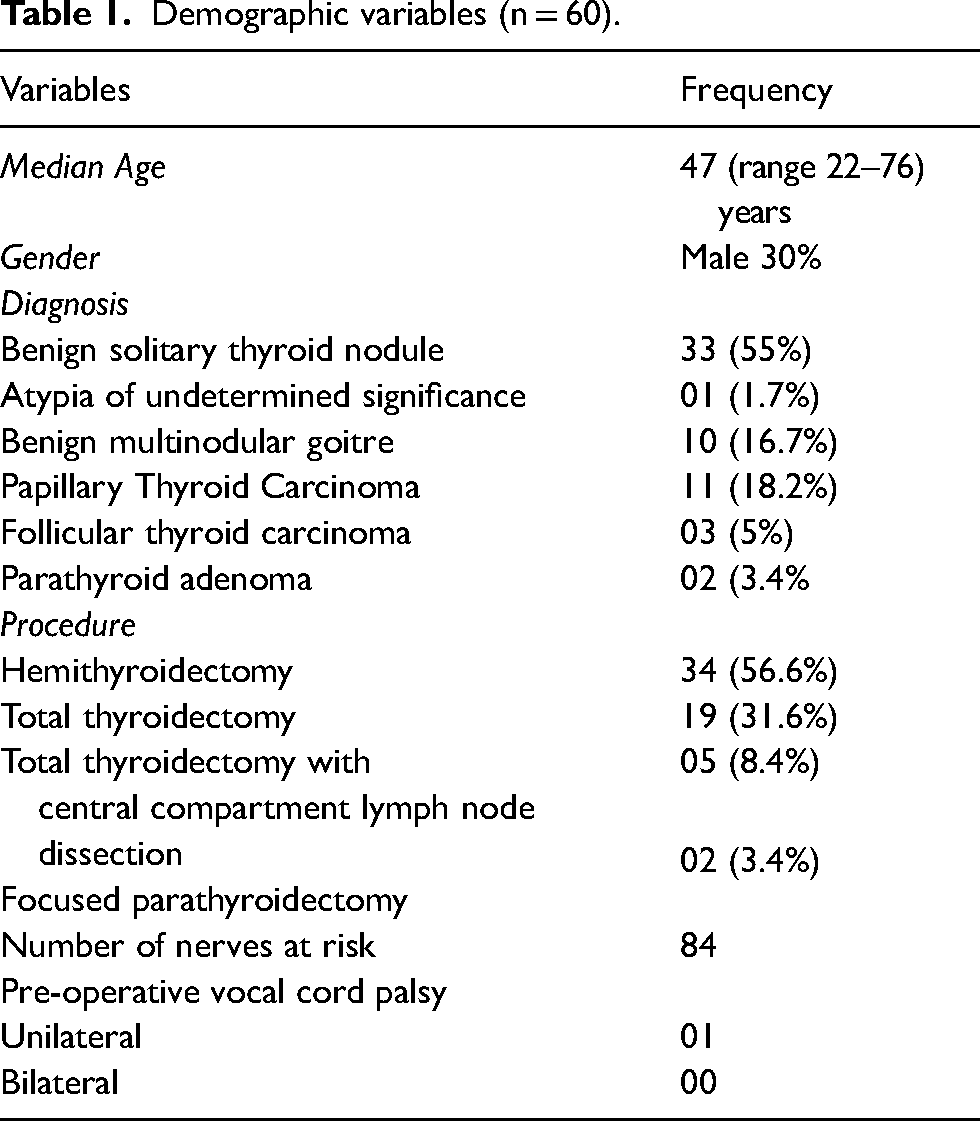
A total of 60 consecutive patients were included in our study. Demographics, clinical profile and intra-operative recurrent laryngeal nerve identification status are depicted in Table 1. Total number of nerves at risk was 84.
Demographic variables (n = 60).
Pre-operative vocal cord assessment:
Fifty six patients had successful app based VC assessment in the OPD (feasibility 93%). These patients had 79 nerves at risk. Four patients had gag reflex despite spray of topical Xylocaine and hence pre-operative app based VC assessment was not successful. These patients had five nerves at risk and had successful DL. (Table 2).
Comparison of pre-operative and post-operative IDL with app based VC assessment and standard DL.

IDL- Indirect laryngoscopy, DL- Direct laryngoscopy.
Post-operative vocal cord assessment:
All sixty patients had successful app based VC assessment immediately after extubation, making it 100% feasible. Post-operative DL on the 7th day was compared with post-operative app based VC assessment and there was 100% correlation. Hence, the accuracy of app based VC assessment was 100%. Grading of vocal cord movements too had 100% correlation. Four patients with failure of app based VC assessment pre-operatively, had successful visualization of vocal cords. Post-operative indirect laryngosocopy on day 1 was feasible only in 70% of patients (Table 3).
Correlation of vocal cord examination by different methods.
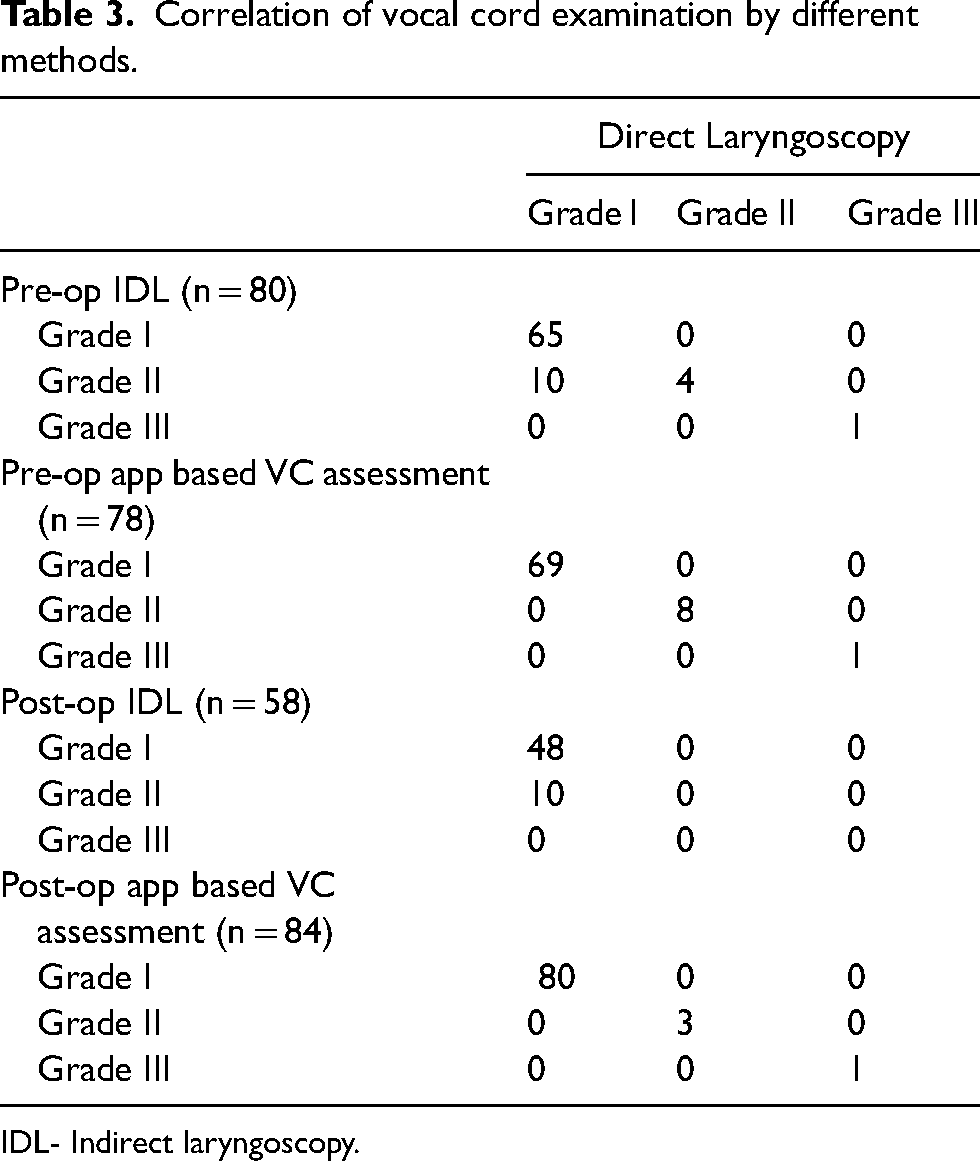
IDL- Indirect laryngoscopy.
Discussion
Our study showed that low cost app based vocal cord assessment technique is feasible.
The status of the RLN before and after thyroid surgery has major consequences and may lead to catastrophic outcomes in some situations. For this purpose, direct visualization of VCs with the help of flexible laryngoscopy is considered a gold standard. 2 However, the non-availability of fibreoptic laryngoscopes is a major limitation for most low resource settings. Even if it is available, it is usually only available in the operation theatre complex or in specialist laryngologists’ hands and not in the out-patient department.
A common method used by anesthetists is to visualize the vocal cords while extubating a patient, using a standard laryngoscope with a Macintosh blade, but inadequate or partial visualization are significant problems with this method. 12
Our method of direct visualization was universally applicable and reliable. It is also the cheapest and easiest to perform.
Supplemental Material
Footnotes
Acknowledgement
N/A
Author contributions
MG: Data collection and analysis
SKY: Writing, editing, review of literature
PA and DS: Revision and editing.
Data availability
Data can be obtained from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Approved by the Ethics committee of the NSCB Medical College, Jabalpur (No. IEC/2023/6466).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.