
Abstract
Dengue is a disease endemic to tropical countries such as India. In the past two years, cases of COVID-19 associated Mucormycosis have become a commonly encountered phenomenon. However, cases of dengue associated Mucormycosis have not found a significant mention in the literature yet. We, therefore, report two such cases in which Mucormycosis developed after recovery from Dengue fever and try to dig into the possible mechanism behind such an occurrence.
Keywords
Introduction
Dengue is a disease caused by single-stranded RNA viruses of the genus Flavivirus and its vectors are female mosquitoes of the species Aedes aegypti and Aedes albopictus. 1 Clinically, it is characterised by fever, joint pain, myalgia, rash, retrobulbar pain, thrombocytopenia and leucopenia. Mild types include undifferentiated fever, dengue fever (DF), and severe forms include dengue haemorrhagic fever (DHF) and dengue shock syndrome (DSS). 2
Mucormycosis is caused by fungi of the order Mucorales, the prime genera causing infections in humans being Rhizopus oryzae followed by Lichtheimia sp and Mucor sp. It is classified into six major clinical forms: rhino-cerebral, pulmonary, cutaneous, gastrointestinal, disseminated and rare forms, such as endocarditis, osteomyelitis, peritonitis, and renal infection. COVID-19 associated mucormycosis (CAM) is now a well-recognised phenomenon which occurs in patients suffering, recovering and recovered from COVID-19. The disease prevalence in India is predicted to be 140 cases per million. 3
The putative causes of this disease in COVID-19 patients include use of steroids, immune dysregulation, use of immunomodulatory drugs and effects on CD4+ and CD8+ T-cells and vitamin D deficiency. 4 However, the occurrence of Mucormycosis following dengue has only been mentioned in one published report of four cases. 5 We report two such cases where the rhino-cerebral variety of Mucormycosis was detected immediately after recovering from Dengue fever.
Case reports
Case 1
A 45-year old male presented with a chief complaint of pain in the right and left maxillary teeth over the previous 15 days. No history of diabetes or other systemic illness and no use of steroids or other immunomodulatory drugs was reported. He had a history of fever 34 days previously which lasted for three days and joint pain which lasted one week after which he was diagnosed with Dengue (IgM positive). He had a decreased platelet count (29 × 109/L) and leucocyte count of 3.39 × 109/L), and raised values of SGOT (176 IU/l) and SGPT (123 IU/l). RT-PCR for COVID-19 was negative. After treatment, his symptoms subsided and his platelet count (176 × 103/µL) reverted to normal by the 20th day of illness, as did his other parameters. On the 21st day, he started experiencing toothache followed by looseness of the teeth after a few days together with anterior and post nasal discharge. On clinical examination, a diffuse swelling was seen in the middle third of his face with normal overlying skin which was soft, warm and tender (Fig. 1(a)). Multiple pustules were visible on the buccal alveolar mucosa and the palate which yielded purulent discharge on palpation (Fig. 1(b), (c) and (d)). All maxillary teeth displayed grade III mobility and the patient's voice had a nasal twang. The patient had, however, no history of COVID-19 and had had two vaccinations with COVAXIN.

Case 1 (a) Diffuse facial swelling. (b) Pustules on the palate. (c and d) Pustules on buccal alveolar mucosa of maxillary teeth. (e) CT scan section showing a soft tissue density in the left maxillary sinus along with destruction of its medial and posterolateral walls and polypoidal thickening in right maxillary sinus. (f) Soft tissue thickening in the left sphenoidal and ethmoidal sinuses.
On the basis of the above findings, a diagnosis of invasive fungal disease involving the sino-maxillary region was made. A CT scan showed a soft tissue density in the left maxillary sinus with destruction of its medial and posterolateral walls (Fig. 1(e)). Polypoidal thickening was seen in the right maxillary sinus and mild soft tissue thickening in the left sphenoidal and ethmoidal sinuses (Fig. 1(f)). Mucormycosis was diagnosed after a potassium hydroxide wet mount examination. Our patient was treated with antral lavage and intravenous liposomal Amphotericin B 5 mg/kg with oral Posaconazole 300 mg BD for two weeks and 300 mg OD subsequently.
Case 2
A 34-year old male reported with the chief complaint of pain in his right upper posterior dentition and had noted a right facial swelling for the past three days. No history of diabetes or other systemic illness and no use of steroids or other immunomodulatory drugs was reported. He had a history of fever, chills and pain behind the eyes 10 days previously and was diagnosed with dengue fever. PCR for COVID-19 was negative. His symptoms subsided within seven days of illness and on the 8th day, he started experiencing pain in the right maxillary posterior teeth which was followed by facial swelling, paraesthesia and epistaxis from the right nasal orifice the following day. On examination, a diffuse erythematous swelling was seen in the right infraorbital and zygomatic region of 3.5 × 2.2 cm size draining pus medial to the medial canthus of the eye (Fig. 2(a)). On palpation, the swelling was firm, warm and tender. A MRI brain and orbit scan showed periorbital soft tissue thickening on the right side, but no intra-orbital nor intracranial involvement (Fig. 2(b)). CT scannig showed the right maxillary sinus to be atrophic with complete opacification by mucosal thickening and with a blocked osteomeatal complex (Fig. 2(c)). The frontal, sphenoid, ethmoid and left maxillary sinuses also demonstrated mucosal thickening (Fig. 2(d)). Again, a diagnosis of Mucormycosis was confirmed on potassium hydroxide wet mount examination. Surgical debridement was carried out with administration of the same medications as for the first patient.
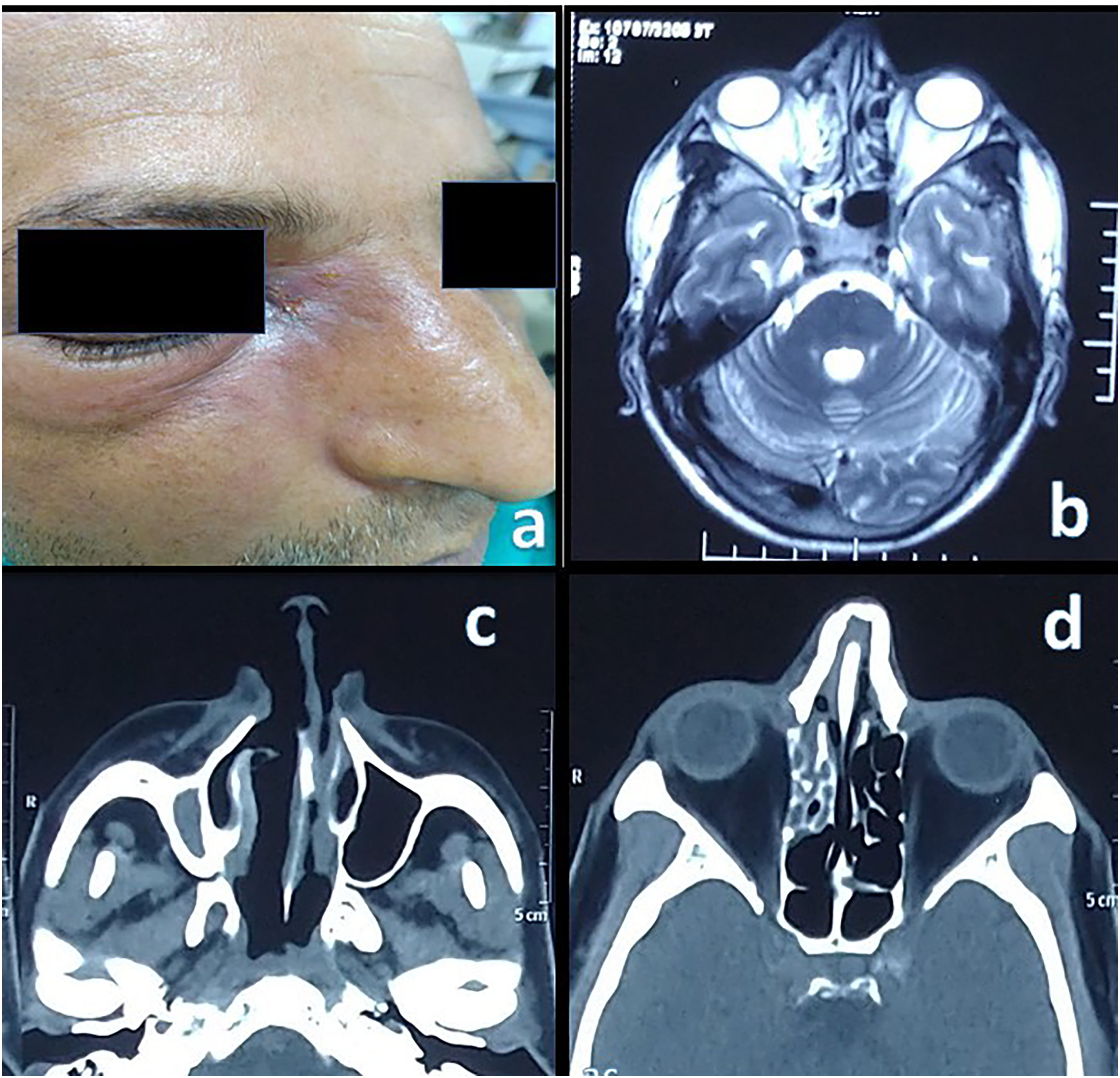
(a) Diffuse facial swelling with draining sinus medial to medial canthus. (b) MRI showing periorbital soft tissue thickening right eye. (c) Right maxillary sinus atrophic in size with complete opacification by mucosal thickening and blocked osteomeatal complex. (d) The frontal, sphenoid, ethmoid and left maxillary sinus demonstrating mucosal thickening.
Discussion
Dengue and fungal co-infection (disseminated candidiasis) was first reported in 2007. 6
One report from India from the post COVID-19 era mentions three cases of Dengue associated invasive fungal infections where histopathology revealed aspergillosis and mucormycosis in cases 1 and 2 and only Mucormycosis in the third patient. There was no previous history of diabetes and steroid use, as in our cases. The age and gender were different. The presenting symptoms were similar to ours, though intracranial involvement was not seen in our cases. Dengue was detected through NS1 antigen positivity. The duration between symptoms of dengue and mucor ranged slightly more broadly in our cases. Another case report from India had no intracranial involvement and in all these six cases, the occurrence of Mucor immediately followed subjective recovery to dengue, signalling a possible association between the two. 5
Plausible mechanisms leading to post-dengue Mucormycosis are: (1) COVID-19 and Dengue Antigen cross reactivity; various case reports and cross-sectional studies across the globed have observed either or two or all three of NS1 antigen, anti-dengue IgM and anti-dengue IgG to be positive in confirmed cases of COVID-19. False positive COVID-19 tests have been found in Dengue. 7 This could be possibly explained by the fact that SARS-CoV-2 spike protein and dengue envelope protein are actually similar, of course false positivity cannot be totally ruled out. 8 The reduction in platelet count and its subsequent recovery in case 1 does however suggest Dengue.
(2) COVID-19 and Dengue co-infection. This possibility in tropical and sub-tropical regions, where mosquito borne diseases such as dengue are endemic, is self-evident. 9
(3) Endothelial dysfunction and altered vascular permeability caused by dengue may pave the way for Mucor. The major hallmark of dengue, especially dengue haemorrhagic fever, is an increase in vascular permeability, leading to plasma leakage at the microvascular level in pleural and abdominal cavities. 10 Electron microscopic studies of capillaries in skin biopsies from patients show marked distortion, mildly damaged vessels, perivascular mononuclear cell infiltration, swelling and degeneration of endothelial cells. 11 In the pathogenesis of Mucormycosis, epithelial cell damage plays a key role as the extracellular matrix proteins can be exposed for direct interaction with inhaled or ingested spores leading to its dissemination. 12
Dengue has been endemic since ages, far before COVID-19 came into existence; however, such cases have not been reported earlier, suggesting that COVID-19 might be the real culprit coming under the guise of Dengue. However, it should also be emphasised here that dengue and COVID-19, despite their clinical similarities, follow different courses, require different management and may give rise to potential complications if irrational pharmacotherapy is administered. Hence, correct identification of the disease preceding Mucormycosis is very important.
Conclusion
Dengue fever should find a place in the list of risk factors associated with occurrence of Mucormycosis. Clinicians should show the same amount of vigilance and suspicion in a dengue recovered patient like for a COVID-19 patient when encountering even the faintest signs of invasive fungal disease.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article: We did not receive any funding for the above work.
Informed consent
Appropriate informed consent was taken from the patients for publishing.