
Abstract
Heat stroke is a life-threatening heat-related condition. It is characterised by a core body temperature >40°C with central nervous system abnormalities or organ dysfunction. In our study of 32 adult patients, multiorgan dysfunction was present in 84%. Vasopressors, intensive care, and mechanical ventilation were required in 44%. Mortality was 6.2%. Aggressive pre-hospital cooling treatment may significantly decrease mortality; thus, preventive strategies need to be developed urgently to implement such cooling facilities in public places.
Introduction
Heat stroke is often characterised by a dangerously high body temperature (typically above 40°C) and is often associated with central nervous system (CNS) derangement, such as delirium, convulsions, and coma. 1 As the most severe form of heat-related illnesses (HRIs), heat stroke is associated with high mortality rates, varying between 10–50%. 2 It often involves multiple organ systems, and survivors may suffer from permanent neurological damage. 3 It is of two types: exertional and non-exertional (or classical). The former occurs from physical activity, typically labouring outdoors and running, while classical heat stroke typically affects individuals in high-temperature and high-humidity environments.
Risk factors for classical heat stroke include dehydration, advanced age, alcohol consumption, the use of antihypertensive or psychiatric medication, and previous neurological disorders.4–6 The primary cause is prolonged exposure to high temperatures, particularly in areas with high humidity and poor ventilation.
With the growing impact of global warming, the frequency of HRIs is expected to increase, posing significant public health challenges, especially in regions experiencing extreme weather conditions. 7
In India, official recording of heat wave-related deaths began in 1979. Reports documented 505 deaths across India in 2001. By 2015, the number had risen to 2040! 8 Heatwaves now start earlier in the year, and temperatures in various parts of India frequently reach 50°C, 9 particularly in Western Rajasthan, where our institute is situated. 9
Methods
Data were collected over a duration of two months from May to June 2024. We included all patients >18 years old who presented with suspected heat stroke after providing informed consent. Ethical clearance was obtained from the Institute Ethics Committee (Ref no: AIIMS/IEC/2024/5501, dated 31 December 2024). Patients were excluded if they had cerebrovascular accidents, CNS infections, intracranial lesions, sepsis with a known source or those who refused to give consent.
Various cooling techniques were used to treat the patients. Evaporative cooling involved placing the patient on the bed, removing their clothing, and covering their body with a bed sheet soaked in cool water (15°C). The warm air was directed towards the patient's longitudinal axis from a fan that was positioned on the patient's head side. To maintain the rectal temperature below 39C, the bed sheets were changed every 3–5 min. An infusion of 25 ml/kg (approximately 1000–1500 ml in total) cold saline at 4°C was delkivered within 60 min. The ice packs were placed on the groin, neck, and axilla and replaced every 10 min.
All data were collected on our preformed institutional heat-related illness preparedness proforma (Supplemental File 1), including demographic information, clinical symptoms, vital signs (at 0 and 4 h), Glasgow Coma Scale scores, findings of clinical examination, status of recovery, details of hospital stay, and outcomes such as need for mechanical ventilation, intensive care unit (ICU) admission, length of admission and mortality. Details of pre-hospital treatment received were noted. Supportive therapy, including fluid resuscitation, electrolyte imbalance correction, haemodynamic support and mechanical ventilation, was administered as necessary, with these more severe cases being treated in a specialised heat stroke ward.
Data were entered into a Microsoft Excel worksheet, and the results obtained were subjected to statistical analysis. This was conducted using the Statistical Package for Social Sciences for Windows (SPSS version 21, IBM Corp., Ltd, Newark, USA). Descriptive statistics were employed for all variables in the study. Categorical and continuous variables were compared for outcomes using Fisher's exact test and Student's t-test, respectively. All continuous data were expressed as mean with standard deviation (SD) unless the data were not normally distributed. A p-value of <0.05 was considered statistically significant.
Results
We studied 32 patients during the study period. Their mean age was 55.7 ± 18.2 years. The majority (26) were male. Most were labourers (47%), farmers (31%), or security guards (18%). Substance abuse was noted as follows: tobacco (59%), alcohol (40%), and opium (34%). Comorbidity found included hypertension (22%), diabetes mellitus (9.4%), chronic obstructive pulmonary disease (COPD) (3.1%), and psychiatric illness (6.3%).
Classical heat stroke was present in 40% and exertional in 60%. All patients presented with altered mental status, while seizures, loss of consciousness, and breathlessness were noted in 15%, 25%, and 25% of patients, respectively. Core body temperature at presentation was 40.7± .0.9°C. Vital signs are noted in Table 1.
Demographic characteristics of patients with heat stroke (n = 32).
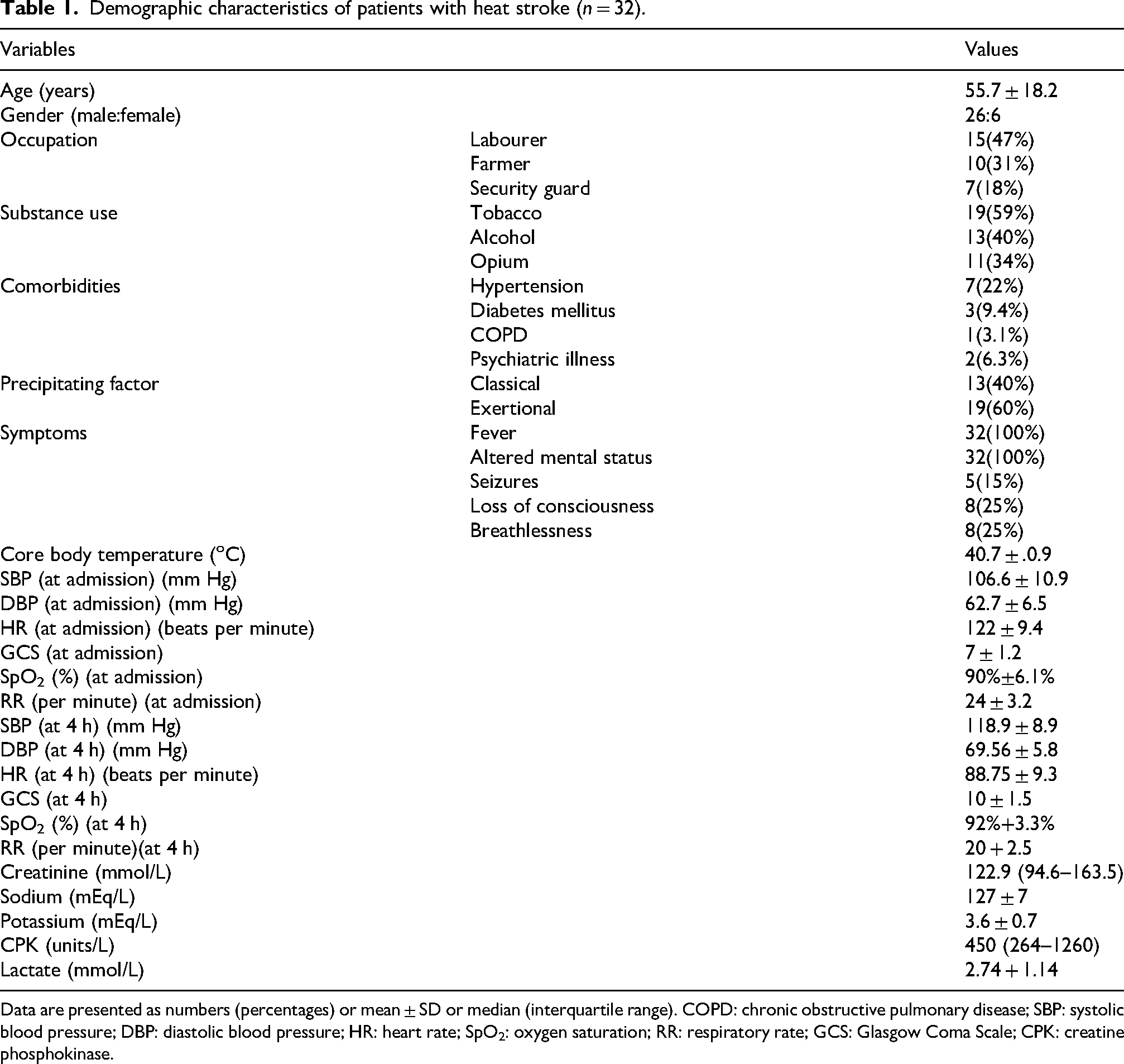
Data are presented as numbers (percentages) or mean ± SD or median (interquartile range). COPD: chronic obstructive pulmonary disease; SBP: systolic blood pressure; DBP: diastolic blood pressure; HR: heart rate; SpO2: oxygen saturation; RR: respiratory rate; GCS: Glasgow Coma Scale; CPK: creatine phosphokinase.
Multiorgan dysfunction syndrome (MODS) was present in 84% and vasopressor support, ICU requirement, and intubation were required in 44%. Two patients demised.
Patients who developed MODS had a significantly lower SpO2, higher creatine phosphokinase (CPK) levels, higher need for mechanical ventilation, more need for vasopressor support and higher mortality (Table 2).
Comparing patients with heat stroke with and without MODS.
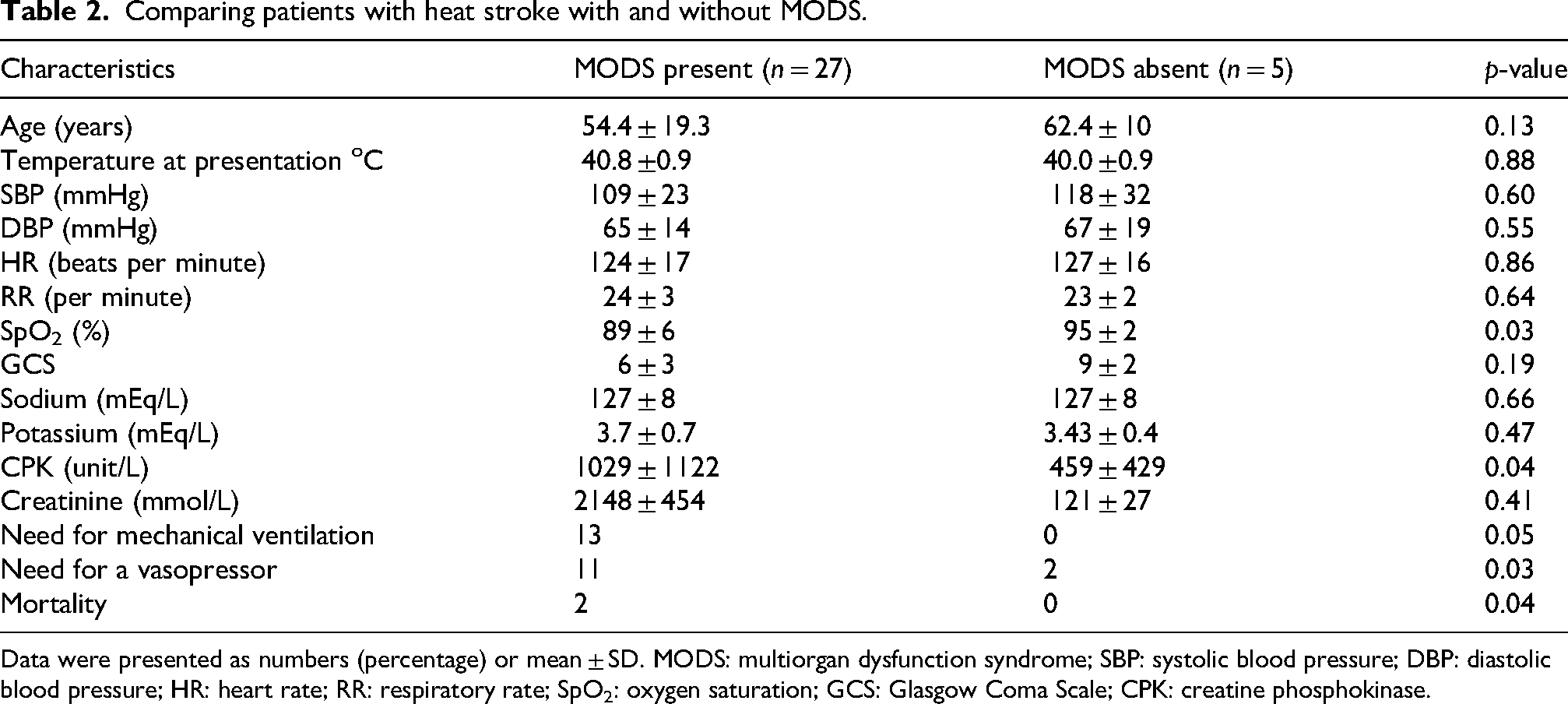
Data were presented as numbers (percentage) or mean ± SD. MODS: multiorgan dysfunction syndrome; SBP: systolic blood pressure; DBP: diastolic blood pressure; HR: heart rate; RR: respiratory rate; SpO2: oxygen saturation; GCS: Glasgow Coma Scale; CPK: creatine phosphokinase.
Discussion
Rajasthan's monthly average temperature peaks at 47°C in May and June. 8 Hence, important preventive measures to protect the population are necessary, including the installation of water spraying fans in public places, provision of free potable cold water, and long-term measures such as increased tree plantations, shaded areas, and education on proper hydration.
The majority of victims of heatstroke were outdoor labourers, many of whom admitted to substance abuse, and many also had significant co-morbidity. Indeed, exertional heat stroke was found more than classical heat stroke, underlining the need for public preventive measures.
There was a significant improvement in vital parameters at the end of 4 h of initial treatment. This suggests that the majority of patients can be saved if cooling is initiated as early as possible. MODS indicated an obvious deterioration.
Our institute has a dedicated heat-related hospital preparedness plan that includes creating special beds in our red zone area of trauma and emergency department, and uses a separate data collection proforma (Supplemental File 1) for heat-related illness to identify their severity and speed up cooling measures. If these are started early, further organ dysfunction and mortality can be reduced.
Heat-health preparedness and response activities, recommended by the Government of India, suggest a “cool first, transport second” policy 10 ; cooling should be continued in an ambulance en route. 11
Our study has a few obvious limitations, being a single-centre observational study with a relatively small sample size, but its conclusions are self-evident.
Conclusion
Heat stroke is becoming ubiquitous in certain parts of the world, particularly in low-resource settings. Several places have reported extreme temperatures: Turbat (Pakistan): 53.7°C, Basra (Iraq): 53.9°C, Mitribah (Kuwait): 53.9°C, Tirat Tsvi (Israel): 54°C, Ahvaz (Iran): 54°C and Kebili (Tunisia): 55°C. 12
Our small study highlights the importance of preventive measures and aggressive management, particularly for outdoor labourers. Public awareness of organ decompensation, particularly cerebral, is important. Most cooling methods do not require medical expertise, except where MODS occurs. 13
Supplemental Material
sj-pdf-1-tdo-10.1177_00494755251389720 - Supplemental material for Emergency department perspective of patients with heat stroke in a tertiary care centre of western Rajasthan: An observational study
Supplemental material, sj-pdf-1-tdo-10.1177_00494755251389720 for Emergency department perspective of patients with heat stroke in a tertiary care centre of western Rajasthan: An observational study by Ankur Sharma, Anil Kumar, Abhishek Sharma and Rahul Chouhan in Tropical Doctor
Footnotes
Acknowledgments
We thank Dr Amit Rohila, Dr Mahaveer Rodha, Dr Jiss V Peter and Dr Avanshu Bansal for their help in conducting this study.
Informed consent
Informed consent was obtained from all individuals included in this study, or their legal guardians. The data of patients is used only for research and educational purposes. The procedures followed the guidelines laid down in the Declaration of Helsinki 1964, and as revised later.
Author contributions
AS conceptualised the study. The methodology was developed by AS, AK and AS. RC conducted a formal analysis and investigation. AS and RC prepared the original manuscript, and all authors participated in the review and revision process. The manuscript has been read and approved by all the authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The manuscript includes all necessary data. The datasets used and/or analysed in this investigation are accessible from the author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.