
Abstract
India's Special Newborn Care Units are critical for reducing preventable neonatal deaths. Systematic evaluation of admission patterns provides evidence for targeted healthcare improvements. Birth asphyxia dominates rural neonatal morbidity. Focused investments in intrapartum monitoring, resuscitation training, and rapid referral systems are essential for reducing preventable deaths.
Introduction
Breaking the cycle of preventable neonatal mortality remains India's most pressing paediatric health challenge, with rural populations bearing disproportionate burdens of adverse outcomes. 1 Each year, approximately 600,000 Indian newborns die within their first month of life, representing nearly 25% of global neonatal deaths despite constituting <20% of global births. 2 This stark reality reflects complex interactions between healthcare access limitations, socioeconomic disparities, and systemic care delivery gaps that perpetuate intergenerational health inequities. 3
Special Newborn Care Units (SNCUs) have developed as a strategic response to this crisis, designed as intermediate-level facilities bridging primary healthcare and tertiary neonatal intensive care. 4 Established under the National Health Mission framework, these units target the critical care gap in rural and semi-urban settings where sophisticated neonatal intensive care units remain inaccessible. 5 The SNCU model represents a paradigm shift toward decentralised, evidence-based newborn care, potentially breaking traditional cycles of referral delays and treatment accessibility barriers. 6
Contemporary evidence suggests that well-functioning SNCUs can achieve mortality reductions comparable to higher-level facilities for appropriately selected cases. 7 However, significant variations exist in admission patterns, case mix complexity, and survival outcomes across different geographic and socioeconomic contexts. 8 Rural SNCUs face unique challenges including delayed presentations, advanced disease states at admission, and limited specialist support, necessitating context-specific evaluation of care delivery patterns. 9
Understanding the clinical epidemiology of SNCU admissions provides crucial intelligence for healthcare system strengthening initiatives. Systematic analysis of admission diagnoses, risk factor distributions and outcome determinants enables evidence-based resource allocation and targeted quality improvement interventions. 10 This approach supports the transition from reactive care models to proactive, prevention-oriented strategies that address root causes of neonatal morbidity.
Our study analyses comprehensive data from 500 consecutive SNCU admissions in rural northern India, seeking to identify such opportunities possible to break existing cycles of preventable neonatal mortality and morbidity.
Methods
Our prospective observational investigation was implemented at the SNCU of a tertiary care centre. This facility operates as a 12-bed intermediate neonatal care unit serving a predominantly rural catchment area encompassing five districts of western Uttar Pradesh, with a combined population exceeding 8.5 million.
The SNCU infrastructure includes temperature-controlled environments with radiant warmers, comprehensive phototherapy capability, mechanical ventilation systems, bubble continuous positive airway pressure (CPAP) devices, and facilities for advanced procedures including central vascular access and chest tube insertion. The unit maintains 24 h physician coverage with trained nursing staff experienced in neonatal care protocols.
We enrolled all neonates <28 days old admitted to the SNCU during an 18-month period from 1 January 2021 to 30 June 2022 to ensure an adequate sample size for meaningful statistical analysis.
Exclusions comprised neonates admitted to alternative hospital units because of SNCU bed constraints, newborns delivered within the facility but immediately transferred to external institutions, and cases where informed parental consent could not be obtained. These exclusions were systematically documented to assess potential selection bias.
We developed a comprehensive data collection instrument capturing multiple domains of clinical information. Maternal parameters included demographic characteristics, obstetric history, antenatal risk factors and delivery circumstances. Neonatal variables encompassed birth characteristics, clinical presentations, diagnostic evaluations, therapeutic interventions and clinical outcomes.
Systematic data collection occurred at admission, during hospitalisation, and at discharge or death. Clinical diagnoses were established using standardised criteria, with senior paediatrician verification for complex cases. Laboratory investigations and imaging studies were performed according to clinical indications and unit protocols.
We employed internationally recognised definitions for key variables. Gestational age classification utilised the World Health Organisation criteria: extremely preterm (<28 weeks), very preterm (28–31 weeks), moderate preterm (32–33 weeks), late preterm (34–36 weeks) and term (≥37 weeks). Birth weight categories included extremely low birth weight (<1000 g), very low birth weight (1000–1499 g), low birth weight (1500–2499 g) and normal birth weight (≥2500 g). 11
Birth asphyxia diagnosis incorporated clinical assessment, Apgar scoring and cord blood gas analysis when available. Sepsis classification followed standard early-onset (<72 h) and late-onset (≥72 h) with laboratory confirmation when possible. 12
Data management utilised Microsoft Excel with subsequent analysis in SPSS version 24.0. Descriptive statistics summarised demographic and clinical characteristics using frequencies, percentages, means and standard deviations as appropriate. Categorical variable associations were evaluated using χ2 testing, with Fisher's exact test for small cell counts. Statistical significance was defined as p < 0.05 with 95% confidence intervals reported for key associations.
The investigation received approval from the Institutional Ethics Committee. Written informed consent was obtained from parents or legal guardians following detailed explanation of study objectives and procedures. Participant confidentiality was maintained throughout data collection and analysis processes.
Results
Our analysis encompassed 500 consecutive neonatal admissions, revealing distinct demographic and clinical patterns (Table 1). The gender distribution suggests potential cultural factors favouring healthcare-seeking behaviour for male infants in rural settings.
Demographic and clinical characteristics of study population (n = 500).
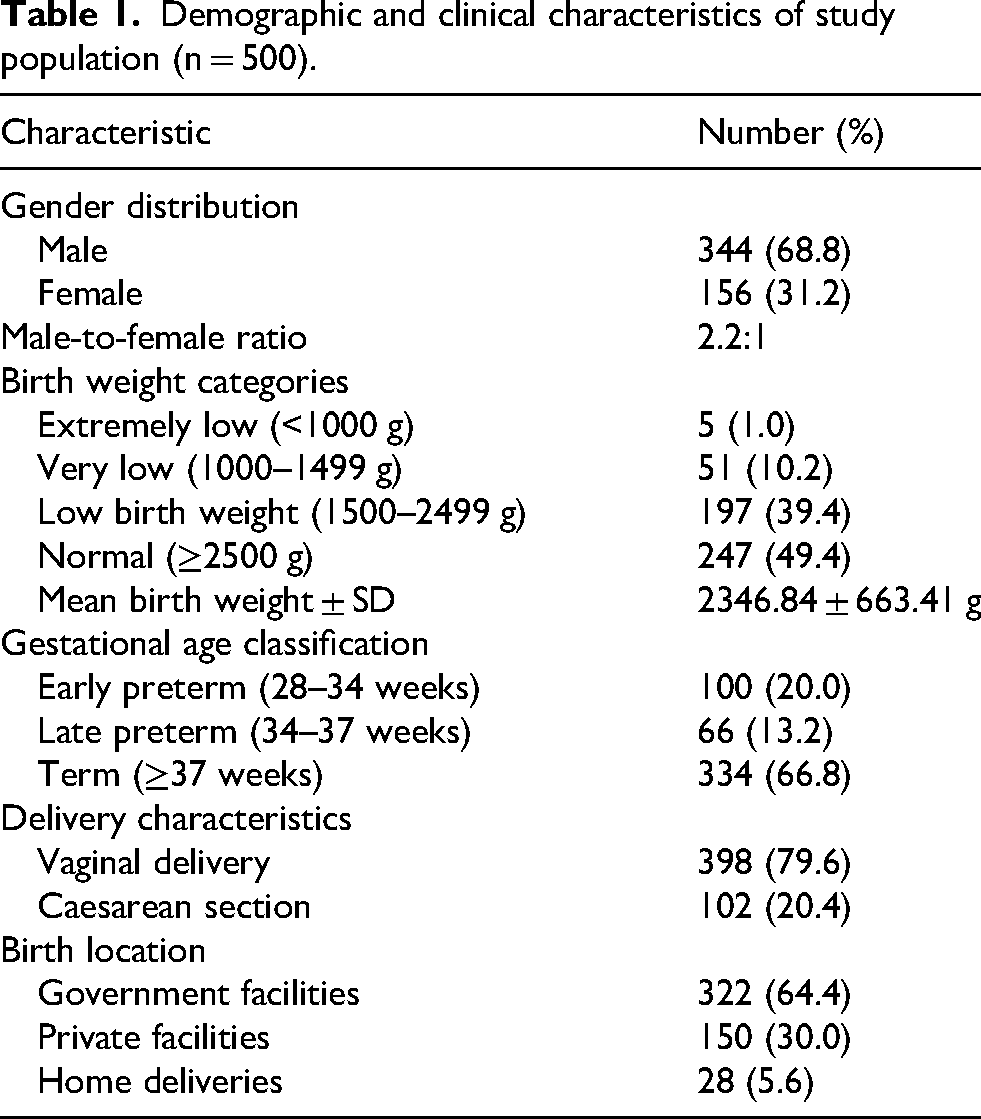
Birth asphyxia emerged as the overwhelmingly dominant admission diagnosis, affecting almost 50% of neonates. This represents a critical finding, as birth asphyxia typically reflects preventable intrapartum complications. Prematurity-related conditions constituted the second leading category (23.4%), followed by central nervous system infections including meningitis (11.2%).
Additional diagnostic categories included neonatal jaundice (28, 5.6%), meconium aspiration syndrome (24, 4.8%), respiratory distress syndrome (17, 3.4%), the high concentration of these preventable diagnoses underscores significant opportunities for upstream interventions (Table 2).
Disease burden and primary admission diagnoses (n = 500).

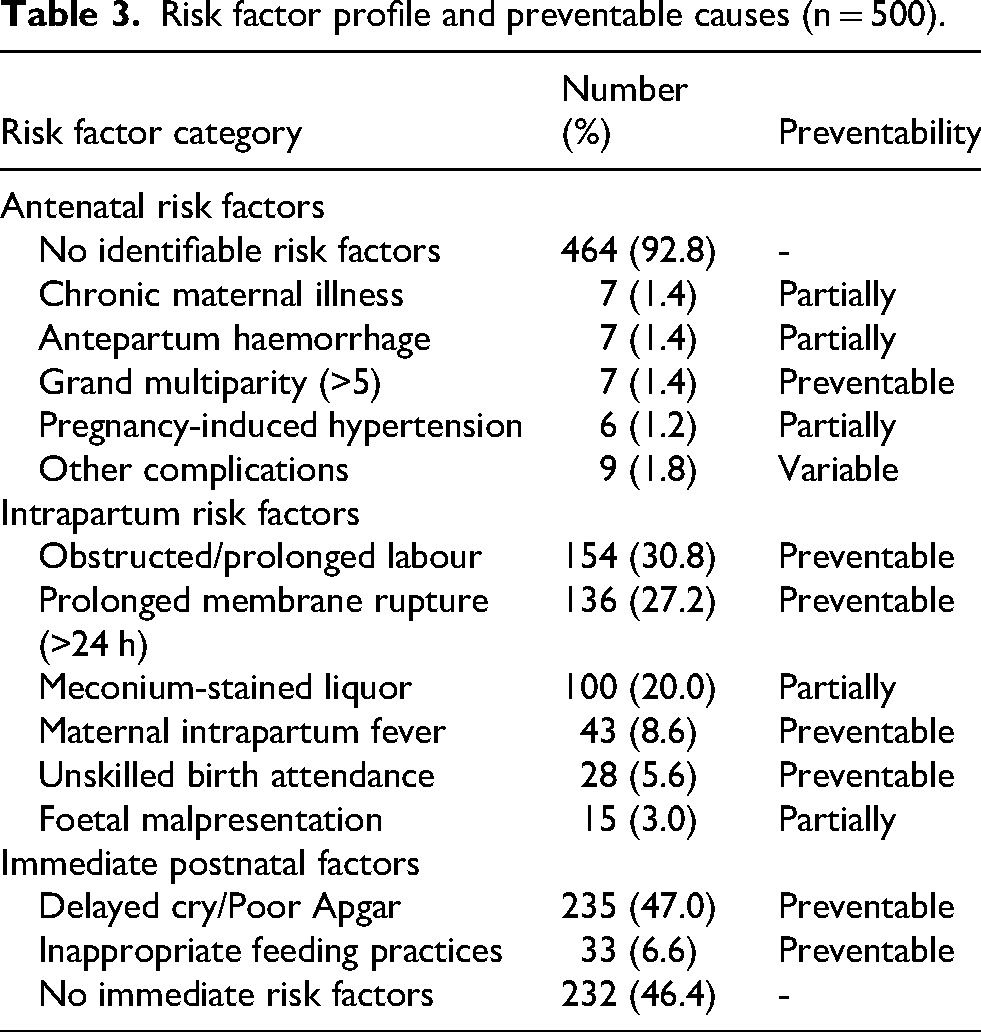
Maternal risk factor evaluation revealed that most (92.8%) mothers had no identifiable antenatal complications, suggesting that intrapartum and delivery-related factors play predominant roles in adverse neonatal outcomes, contributing 30.8% of deliveries. Prolonged rupture of membranes >24 h affected 27.2%, while meconium-stained amniotic fluid was documented in 20.0%, highlighting critical deficiencies in intrapartum monitoring and timely intervention capabilities (Table 3).
Risk factor profile and preventable causes (n = 500).
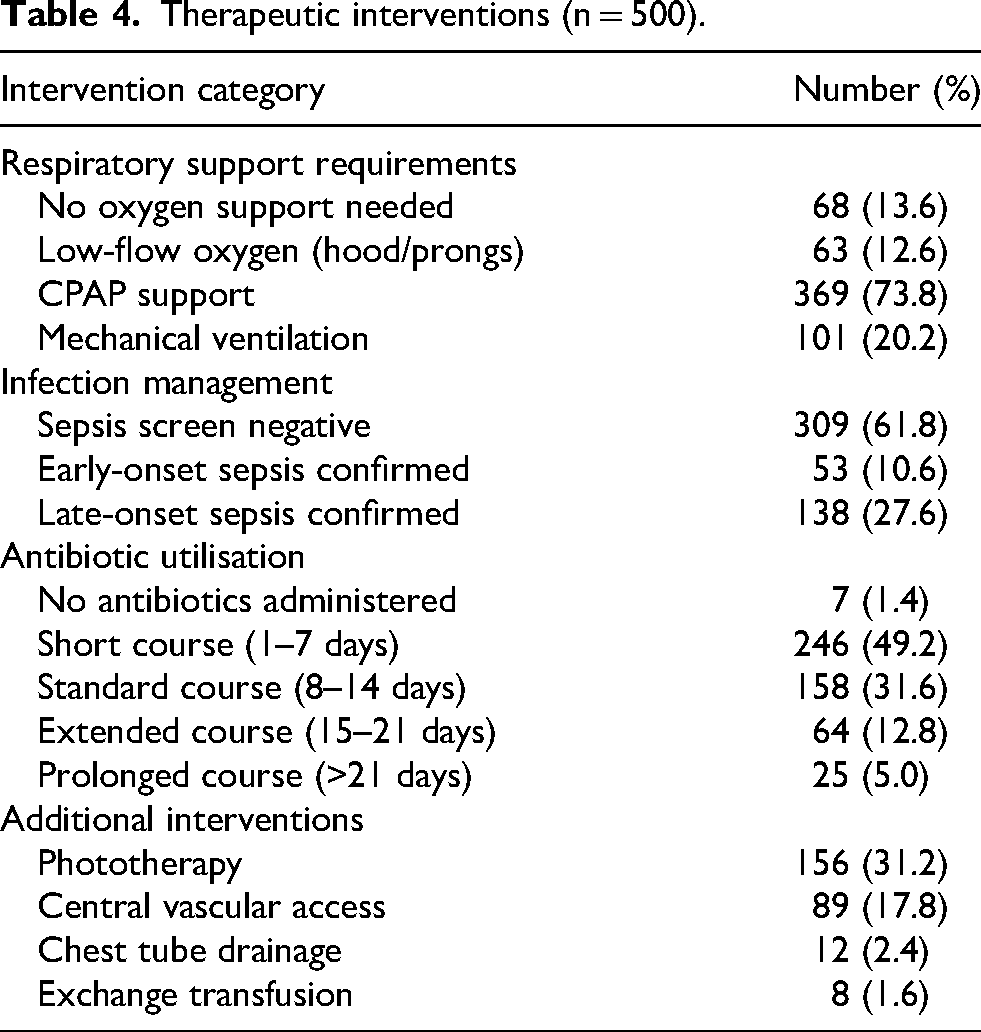
Respiratory support requirements were substantial (86.4%), with CPAP provided to 73.8%, while mechanical ventilation was necessary for 20.2%, reflecting both disease severity and the potential for successful intervention with appropriate technology.
Sepsis with positive screening was found in 38.2%, with late-onset sepsis predominating (27.6%) over early-onset sepsis (10.6%). Antibiotic therapy was administered to almost all (98.6%), with short courses (1–7 days) in c.50% cases to prolonged therapy (>21 days) in 5.0% (Table 4).
Therapeutic interventions (n = 500).
Successful discharge was achieved in 78.2%. Birth asphyxia was the leading cause of death (41.0%), followed by sepsis (30.1%) and respiratory distress syndrome (16.9%). Some 83/101 (82.2%) ventilated patients died but those not ventilated patients all survived (p < 0.001). This stark difference reflects both illness severity and potential limitations in advanced life support capabilities.
Timing of admission significantly influenced outcomes, with neonates presenting within 24 h experiencing highest mortality rates (34.3%), while those admitted later (3–7 days) had lowest mortality. Birth weight demonstrated strong inverse correlation with mortality risk across all weight categories (Table 5).
Survival outcomes and critical mortality determinants.
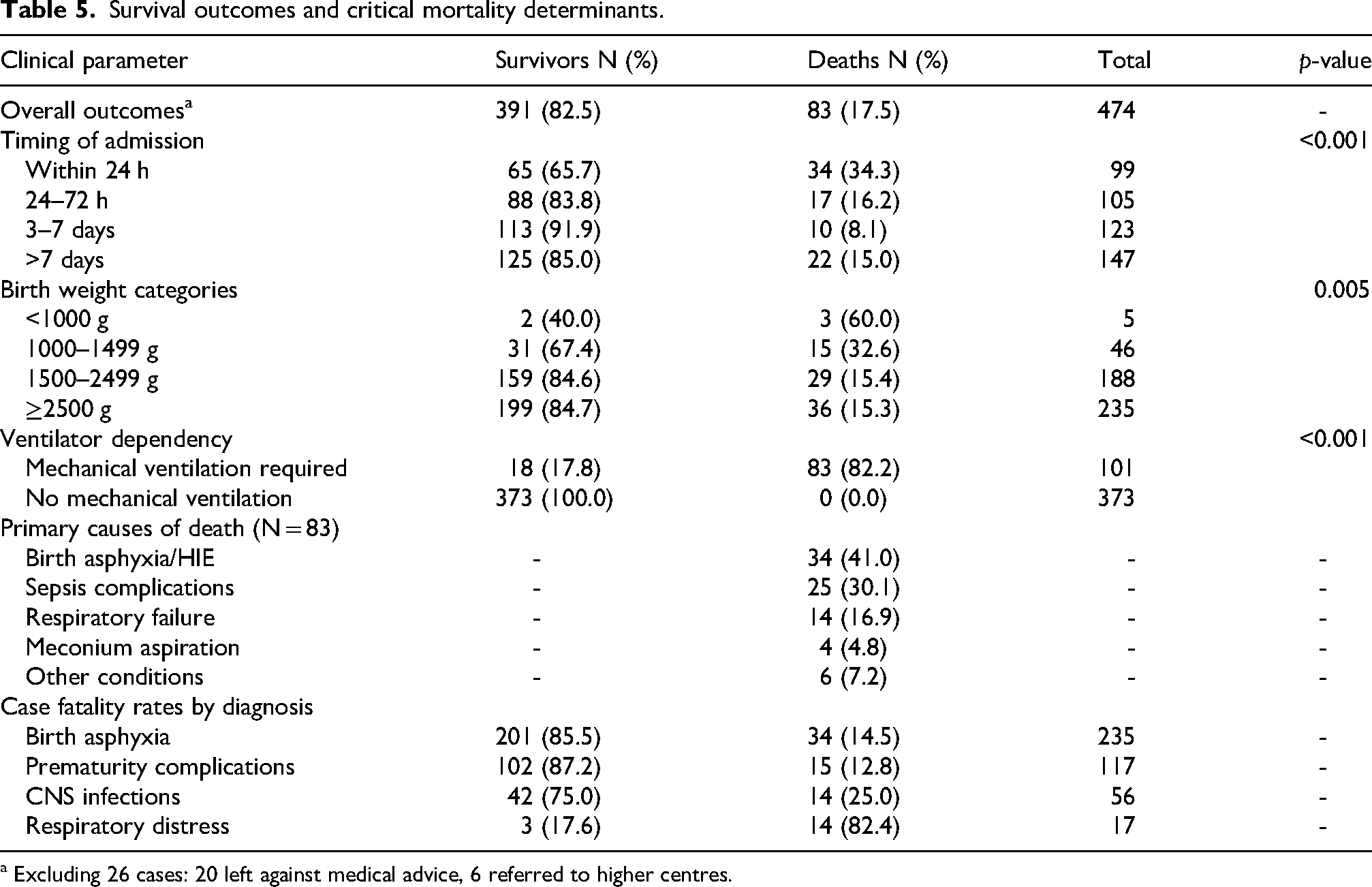
a Excluding 26 cases: 20 left against medical advice, 6 referred to higher centres.
Discussion
Birth asphyxia emerges as the dominant driver of both neonatal morbidity and mortality in rural India, dramatically exceeds national averages reported in urban tertiary centres, highlighting profound rural–urban healthcare disparities. 13 The concentration of asphyxia cases represents a critical intervention opportunity, as birth asphyxia is largely preventable through improved intrapartum care and immediate neonatal resuscitation. 14
An important limitation of our birth asphyxia classification is the lack of systematic encephalopathy assessment using standardised criteria. While 65–70% of cases classified as birth asphyxia demonstrated clinical signs consistent with hypoxic-ischaemic encephalopathy, the absence of prospective Sarnat staging means our 47% birth asphyxia prevalence may overestimate true intrapartum hypoxic-ischaemic injury. Low Apgar scores without subsequent encephalopathy may reflect transient adaptation issues, maternal medication effects, or other perinatal factors rather than clinically significant hypoxia-ischaemia. Future studies should incorporate standardised encephalopathy grading (Sarnat or modified Sarnat staging) within the first 6–24 h to identify more accurately neonates with genuine hypoxic-ischaemic injury requiring targeted neuroprotective interventions. This distinction is clinically critical, as true HIE cases require different management approaches and prognostic counselling compared to neonates with low Apgar scores who demonstrate normal neurological examination findings.
The reliability of birth asphyxia diagnosis varies by gestational age. Clinical signs of encephalopathy become diagnostically reliable only from approximately 35 weeks’ gestation onwards, as very preterm infants commonly present with low Apgar scores owing to respiratory immaturity, poor muscle tone and cardiovascular instability related to prematurity itself rather than intrapartum hypoxic-ischemic injury.
In our study, birth asphyxia classification was predominantly applied to late preterm (≥35 weeks) and term infants (85–90% of cases), with very preterm neonates with low Apgar scores generally classified under prematurity complications unless clear intrapartum hypoxic events were documented. However, diagnostic ambiguity exists in the 35–37 week gestational age window, where both prematurity-related factors and genuine hypoxic-ischaemic injury may contribute to clinical presentation. This overlap may have resulted in some misclassification, potentially inflating our birth asphyxia prevalence while underestimating prematurity-related complications. Future studies should employ gestational age-specific diagnostic algorithms and distinguish between true hypoxic-ischemic encephalopathy in near-term/term infants versus prematurity-associated low Apgar scores in preterm populations.
The strong association between obstructed labour (30.8%) and subsequent neonatal asphyxia demonstrates clear causal pathways amenable to systematic intervention. Evidence from similar settings suggests that enhanced foetal monitoring during labour, timely recognition of foetal distress and rapid decision-making for operative delivery can significantly reduce asphyxia rates. 15 However, implementing these interventions requires substantial investments in healthcare workforce training and infrastructure development.
Our findings that neonates admitted within 24 h experienced mortality rates of 34.3% reflects complex interactions between disease severity, quality of immediate postnatal care and referral timing. Firstly, severe disease drives early admission, which inherently carry high mortality risk regardless of care quality. Secondly, inadequate immediate resuscitation and stabilisation at delivery points may worsen outcomes in severely compromised neonates who might have achieved better results with optimal delivery room management and immediate postnatal care. Thirdly, delayed presentations (3–7 days) predominantly represent less severe conditions such as late-onset sepsis, feeding difficulties or jaundice, which carry intrinsically lower mortality risk.
This complexity has important pragmatic implications. While strengthening neonatal resuscitation capabilities at delivery points remains essential, improved resuscitation alone cannot fully address the underlying problem. The high burden of severe intrapartum compromise requiring immediate intensive intervention reflects fundamental deficiencies in intrapartum care quality. Preventing severe birth asphyxia requires:
Enhanced intrapartum foetal monitoring to detect foetal distress early Timely recognition and management of obstetric complications (obstructed labour, placental abruption, cord prolapse) Rapid decision-making and access to emergency Caesarean delivery when indicated Skilled birth attendance with capability for both obstetric intervention and immediate neonatal resuscitation, that is, investment in comprehensive emergency obstetric and newborn care (EmONC) capabilities at delivery points
Thus, breaking the cycle of preventable early neonatal mortality requires integrated improvements spanning both intrapartum obstetric care and immediate neonatal resuscitation, rather than focusing solely on newborn stabilisation after delivery.16,17
The dramatic mortality of mechanically ventilated neonates reveals critical technology-outcome relationships in resource-limited settings. While this disparity partly reflects illness severity, it also suggests potential limitations in ventilator management expertise and supportive care capabilities. 18 With appropriate training and protocols, mechanical ventilation outcomes in resource-limited settings can, however, approach those achieved in high-income countries. 19
Birth asphyxia and sepsis, as leading causes of death, represent preventable mortality, amenable to improved intrapartum care and neonatal resuscitation for asphyxia prevention, and enhanced infection control practices for sepsis reduction. 20
Furthermore, the high sepsis burden, particularly late-onset sepsis, suggests opportunities for infection prevention improvements within SNCU environments. Implementation of standardised infection control bundles and antimicrobial stewardship programs could significantly reduce sepsis-related mortality.
Our study's strength lies in its comprehensive prospective design and focus on a rural population representative of India's demographic majority. Its limitations include single-centre design and absence of long-term neuro-developmental outcome assessment, which would provide additional evidence for intervention prioritisation.
Conclusion
Our evidence supports a multi-level intervention strategy focusing on: (1) strengthening intrapartum care capabilities at peripheral delivery points, (2) enhancing immediate neonatal resuscitation skills among birth attendants, (3) improving rapid referral systems for critically ill neonates, and (4) advancing SNCU care quality through standardised protocols and staff training.
Footnotes
Acknowledgements
We extend our gratitude to nursing staff and paediatric residents whose meticulous patient care and data documentation made this investigation possible.
Ethical clearance
The study was approved by UP University Of Medical Sciences Ethics Committee vide letter 1915/UPUMS/dean(M)/Ethical/2020-21 date: 21.6.2021, number: 183/2020-21 with written informed consent obtained from all parents.
Author contributions
Study conception and design: RC, MA; data collection: NS; analysis and interpretation of results: MA, RAR, NKS; draft manuscript preparation: MA, RAR; all authors reviewed the results and approved the final version of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Anonymised datasets supporting the study conclusions are available from the corresponding author upon reasonable request, subject to institutional ethics committee approval and applicable data protection regulations.