
Abstract

Keywords
Introduction
Paediatric sepsis is a leading cause of morbidity and mortality globally, more prevalent in low- and middle-income countries, with clinical presentations ranging from mild infection to septic shock and multiorgan dysfunction.1,2 While common organisms such as Streptococcus pneumoniae and Escherichia coli are frequently implicated, rare and emerging pathogens are also encountered. Robertmurraya beringensis is an aerobic, Gram-positive bacillus originally isolated from marine and environmental sources. It was reclassified from the Bacillus genus based on phylogenomic analyses but, until recently, has not been reported as a community-acquired human pathogen causing sepsis.3,4 R. beringensis has been described as a hospital-acquired organism with limited evidence of human pathogenicity, probably due to its environmental origin and the apparent absence of classical virulence factors, rendering infection uncommon. 4 However, emerging clinical reports, including this case, demonstrate that it can act as an invasive pathogen in both hospital and community settings. 5 The identification was made possible by MALDI-TOF (Matrix-Assisted Laser Desorption/Ionisation Time-of-Flight) mass spectrometry, a rapid tool improving detection of rare organisms not easily identified by conventional microbiology methods.5–8 Early pathogen identification remains critical for guiding targeted therapy in paediatric sepsis.
Furthermore, this case also highlights the importance of investigating coexisting conditions that may complicate clinical management—in this instance, fascicular ventricular tachycardia caused by a false tendon, unrelated to sepsis but critical to recognise for comprehensive care.
Case report
A 5-year old girl, the second child of non-consanguineous parents with no significant birth or past medical history, presented with a one-day history of high-grade fever, vomiting and multiple loose stools. There was no history of rash, abdominal pain, jaundice, bleeding, urinary, or respiratory symptoms. The illness followed the consumption of well water near her home. Several cousins who had consumed the same water developed similar complaints, and two required brief hospitalisation.
On arrival at the emergency department, the child was febrile (40 °C), pale and lethargic but alert and communicative. She was in cold hypotensive shock, with tachycardia of 160/min, hypotension (BP: 70/44 mmHg) (below the 5th centile for age), narrow pulse pressure, cold extremities and thready pulses. She had tachypnoea at 34/min with normal oxygen saturation. Systemic examination revealed no organomegaly nor focal findings.
Initial management included isotonic saline boluses (20 mL/kg followed by 10 mL/kg) with intermittent reassessment. Intravenous ceftriaxone (100 mg/kg) was administered after obtaining cultures. Despite resuscitation, perfusion remained poor, prompting initiation of dopamine infusion (10 µg/kg/min) for fluid-refractory shock. She was subsequently transferred to our paediatric intensive care unit (PICU). Here, the shock profile evolved from cold to warm hypotensive shock. She was intubated, dopamine was discontinued and noradrenaline infusion (0.1 µg/kg/min) was started. Over the next several hours, she developed six episodes of ventricular tachycardia (VT). The first three resolved spontaneously, while subsequent episodes required electrical cardioversion. The initial cardioversion (0.5 J/kg) restored sinus rhythm, but later arrhythmias were refractory, necessitating higher-energy shocks and antiarrhythmic therapy (Fig. 1). Recurrent fascicular VT episodes were managed sequentially with intravenous lignocaine, amiodarone and diltiazem. Once stable, treatment was continued with oral amiodarone and diltiazem for maintenance of sinus rhythm under cardiac monitoring. Supportive therapy included correction of metabolic acidosis, electrolyte replacement and vitamin D supplementation. Persistent hypotension required adrenaline (0.1 µg/kg/min), vasopressin (0.0005 U/kg/min) and dobutamine (10 µg/kg/min) infusions to maintain haemodynamics, which were titrated.
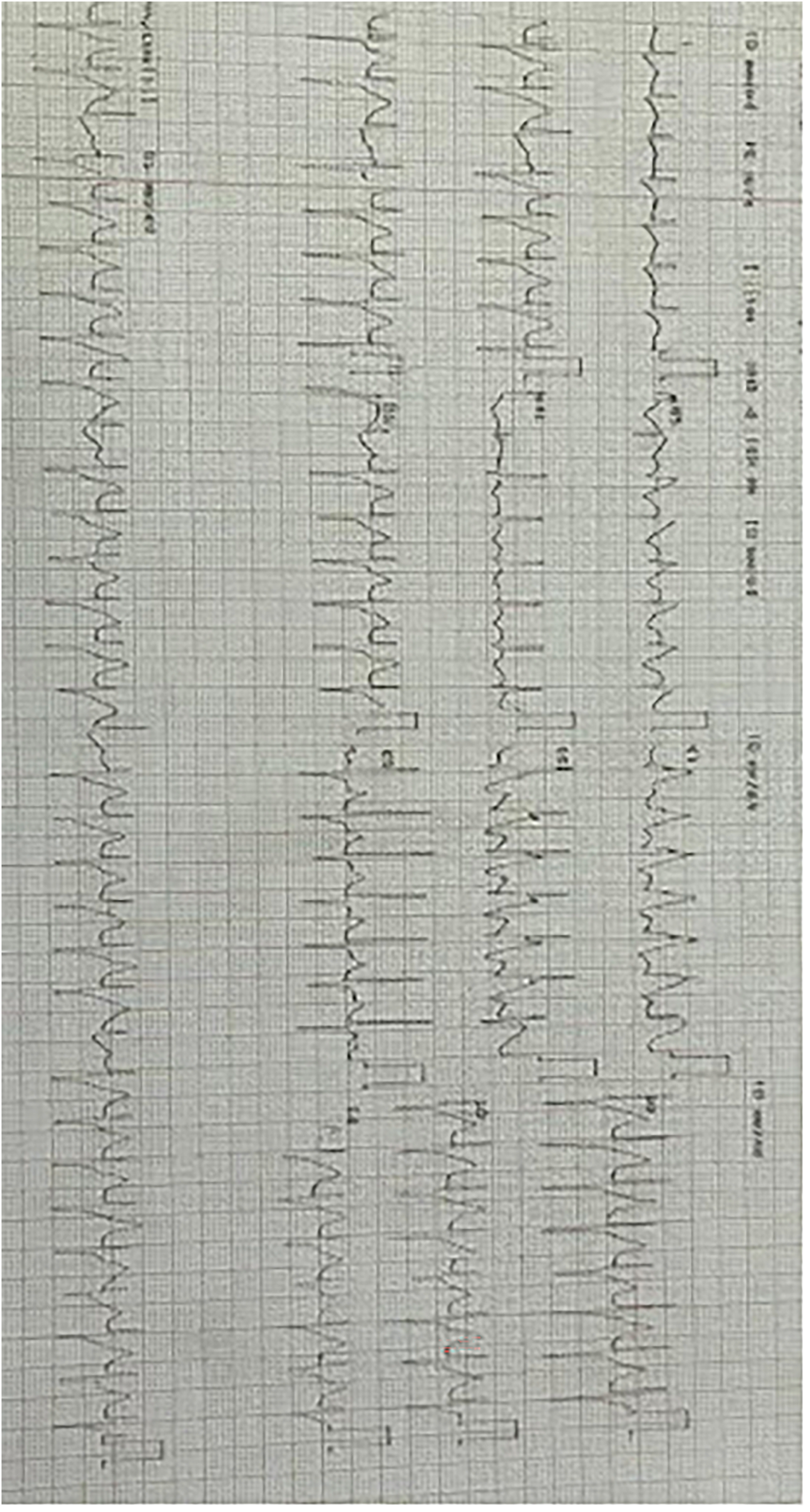
Twelve lead ECG showing fascicular ventricular tachycardia.
Laboratory results showed a normal complete blood count and peripheral smear initially, followed by mild thrombocytopenia. Serum electrolytes and renal and liver function tests were normal. Inflammatory markers were markedly elevated (CRP 220 mg/L, procalcitonin 78.8 ng/mL), while IL-6 was within normal limits (6.56 pg/mL). COVID-19 IgG was positive and IgM negative, suggesting prior exposure or vaccination. Blood culture, sent on admission, grew aerobic gram-positive bacilli, later identified as Robertmurraya beringensis using MALDI-TOF mass spectrometry within 24 h of culture positivity. Other cultures (urine, stool, endotracheal aspirate) and the tropical fever panel (including Dengue, Rickettsia, Scrub typhus, Leptospira, Plasmodium and Salmonella) were negative.
Echocardiography demonstrated global left ventricular dysfunction (ejection fraction 35%) without valvular disease and revealed a false tendon traversing the left ventricle, serving as the substrate for fascicular VT (Fig. 2). Troponin-I, CPK-MB and BNP were within normal limits.

2D echocardiogram depicting false tendon in the left ventricle (marked with arrow).
The child was promptly started on empirical broad-spectrum antimicrobial therapy with intravenous ceftriaxone and clindamycin (antitoxin action), targeting both Gram-positive and Gram-negative organisms, including potential anaerobes. However, considering her unrelenting fever and rapid haemodynamic deterioration, intravenous ceftriaxone was omitted and intravenous meropenem was added with oral azithromycin (suspecting Campylobacter jejuni). Despite this, fever proved to be persistent and according to hospital protocol and local antibiotic stewardship, IV antibiotics were escalated to intravenous colistin with meropenem.
In lieu of rapid clinical deterioration and shock at presentation, and persistent fever despite appropriate broad-spectrum antibiotics and poor response to escalating vaso-active support, COVID-19 IgG positivity with markedly elevated inflammatory markers, and malignant arrhythmias refractory to pharmacological and electrical therapy, a hyper-inflammatory state was strongly suspected. Immuno-modulatory therapy was therefore initiated with intravenous methylprednisolone (10 mg/kg/day), followed by intravenous immunoglobulin (2 g/kg).
Over the next 7–10 days, her condition improved steadily. She was extubated on day 8 and gradually weaned off vasoactive infusions. Fever subsided, inflammatory markers declined and ventricular function normalised. No further VT episodes occurred after initiation of maintenance antiarrhythmics. At discharge, she remained haemodynamically stable on oral diltiazem and amiodarone, with plans for outpatient follow-up. She was referred for ongoing rhythm monitoring and consideration of ablation if VT recurred, and for amiodarone surveillance. Her parents were counselled regarding medication adherence, recognition of arrhythmia symptoms and precautions during physical activity.
Discussion
The primary differential diagnoses considered in this case included toxic shock syndrome, given the rapid progression to shock with multiorgan involvement. Other tropical infections such as Dengue shock syndrome and Rickettsial infection were also considered but ruled out by a negative tropical panel. Campylobacter jejuni infection was entertained owing to the classical presentation of fever with multiple loose stools. Viral myocarditis was suspected because of left ventricular dysfunction and arrhythmia. Electrolyte-induced ventricular arrhythmias were also evaluated as possible contributors, given the coexisting hypocalcaemia, hypokalaemia and hypophosphatemia. Ultimately, fascicular ventricular tachycardia was attributed to a false tendon in the left ventricle, acting as a structural substrate for reentrant arrhythmia rather than being directly related to the septic pathophysiology.
Our case had two rare co-existing findings in a critically ill paediatric patient: septic shock caused by Robertmurraya beringensis and fascicular ventricular tachycardia (VT) attributed to a left ventricular false tendon. Each condition posed unique diagnostic and management challenges.
Robertmurraya beringensis is a rare, gram-positive, aerobic bacillus with limited literature describing its clinical pathogenicity in humans. It was previously isolated from the Bering Sea and classified under the genus Bacillus, later redefined through phylogenomic studies. 3 Notably, the patient's cousins presented with milder complaints following consumption of water from a well near their residence, two requiring brief hospitalisation, indicating an environmental origin and community acquisition of this infection.
A recent case series in neonates described clinical features such as lethargy, refusal to feed, apnoea and temperature instability, the only other human cases so far found for this organism, demonstrating its ability to cause late-onset sepsis in vulnerable populations. 5
The use of MALDI-TOF has transformed microbial diagnostics in tertiary care settings. The identification of R. beringensis in this case was facilitated by Matrix-Assisted Laser Desorption/Ionisation Time-of-Flight Mass Spectrometry (MALDI-TOF MS). This technology has revolutionised pathogen identification by rapidly analysing microbial protein profiles and comparing them to extensive reference libraries. 5 Unlike traditional biochemical methods, which take 24–72 h and may misidentify or misclassify rare species, MALDI-TOF can yield accurate results within minutes after culture growth, even for uncommon environmental organisms. It offers rapid turnaround time (typically <1 h post-isolation) and high sensitivity and specificity, making it especially valuable in critically ill patients where timely, targeted therapy is essential. 6 Its increasing use in PICUs has shortened diagnostic timelines and enabled early targeted therapy, as demonstrated in our case,7,8 where within 24 h of initial culture growth, the organism was identified.
In parallel, the patient exhibited recurrent episodes of fascicular ventricular tachycardia, which was unusual in the context of septic shock. This type of idiopathic left ventricular tachycardia (ILVT) is usually seen in structurally normal hearts of children and young adults. However, echocardiography in this case revealed a false tendon in the left ventricle, a recognised dysrhythmogenic substrate. False tendons are fibromuscular bands within the ventricular cavity that can harbour Purkinje fibres and facilitate reentry circuits, predisposing to fascicular VT. 9 While typically benign, these structures have been implicated in sustained monomorphic VT, often confused with supraventricular tachycardia but unresponsive to adenosine, especially when precipitated by triggers such as fever, inflammation, or electrolyte imbalances.10–12 In this case, the arrhythmia was refractory because of the combination of sepsis, electrolyte abnormalities and the pre-existing false tendon, complicating management. Treatment with intravenous amiodarone, diltiazem and later oral maintenance therapy successfully controlled the dysrhythmia. The long-term prognosis of fascicular VT is generally favourable with treatment; recommended therapy includes calcium channel blockers and antiarrhythmics, with catheter ablation reserved for refractory cases. 10
The use of IVIG and methylprednisolone contributed to resolution of systemic inflammation and myocardial irritability, although their precise roles cannot be independently determined.
Our case emphasises maintaining a broad differential diagnosis in paediatric septic shock, particularly in atypical presentations or poor therapy response. It reinforces the value of advanced diagnostics like MALDI-TOF and echocardiography to uncover rare aetiology and the importance of multidisciplinary collaboration in achieving favourable outcomes.
Key messages
Robertmurraya beringensis, an environmental bacillus, can occasionally cause community-acquired paediatric sepsis; correlation with clinical context is essential before inferring pathogenicity.
MALDI-TOF mass spectrometry enables rapid identification of rare organisms, guiding timely and targeted antimicrobial therapy in critically ill children.
Fascicular ventricular tachycardia may coexist with sepsis due to independent structural or metabolic triggers, such as a false tendon in the left ventricle.
Multidisciplinary management addressing both infectious and cardiac components is crucial for favourable recovery in complex paediatric shock presentations.
Footnotes
Acknowledgements
The Department of Pediatrics and Cardiology at Bharati Vidyapeeth Medical College, Hospital and Research Centre, Pune.
Ethical consideration
Written informed consent was obtained from the patient's parents/legal guardians for publication of this case report and accompanying images. All efforts were made to ensure patient anonymity.
Ethical approval and consent
Informed consent was obtained from the patients’ caregivers or legal guardians prior to inclusion in this study. Ethical approval for this case was granted by the Institutional Review Board of Bharati Vidyapeeth (Deemed to be University), Medical College and Hospitals prior to the commencement of the case report and manuscript preparation.
Author contributions
Bhanuja Bhagwat: Drafted the case report, acquisition and interpretation of clinical data, manuscript drafting, and critical revision for intellectual content. Bhakti Sarangi: Conception of the case report, supervision of patient management, contribution to data collection, and substantial input in manuscript editing and review. Noopur Kulkarni: Assisted in clinical data acquisition, literature review, and preparation of the initial draft of the manuscript with editing. Ajay Walimbe: Provided critical input in patient management, microbiological correlation, and contributed to manuscript revision and approval of the final version. Chandrakant Chavan: Provided cardiology expertise, contributed to the interpretation of arrhythmia findings, echocardiographic correlation, and reviewed the manuscript for accuracy and clinical relevance. All authors approved the final version of the manuscript and agreed to be accountable for its contents.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Bhakti Sarangi