
Abstract
With the objective of decreasing the incidence of endotracheal tube occlusion (ETO) by 25% in our neonatal intensive care unit, we identified potential causes of insufficient humidification, identified a lack of knowledge regarding the use of humidifiers during ventilation, and established a standard procedure. Subsequent improvement of practice, viz. standardising gas flow, keeping adequate water levels in the humidifying chamber, eliminating defective probes and providing interactive nurse training, achieved sustained reduction of ETO by 40% over a period of 32 weeks.
Introduction
The introduction of mechanical ventilation has been attributed to higher rates of morbidity and mortality in critically ill neonates receiving care in a neonatal intensive care unit (NICU). 1 Endotracheal tube obstruction is its most feared complication. Partial tube occlusion, which is generally caused by secretions, renders breathing difficult. Complete blockage, whilst rare, is potentially catastrophic and necessitates immediate tube replacement.2–5 Risk factors of endotracheal tube obstruction include the duration of invasive mechanical ventilation, bacterial colonisation of the endotracheal tube with biofilm formation, and thick respiratory secretions. 6 Insufficient humidification of inhaled gases is the main cause.7–9
Complete humidification, in which the gas in the circuit is warmed to a specific target temperature with water vapour introduced from a heated water reservoir, is a necessary component of any effective ventilation strategy. Effective airway humidification is essential for mucociliary clearance, proper surfactant action, reducing airway resistance, and enhancing lung compliance. Theoretical justification and extensive clinical practice experience point to a design that simulates physiological conditions in the intubated airway.
Insufficient humidification causing endotracheal tube blockage was diagnosed on the presence of any of the following: (a) visible secretions in the endotracheal tube, (b) clinically audible secretions, (c) a reduction in air entry, (d) a see-saw pattern in the flow-volume loops of the ventilator's graphics, (e) a need for high peak inspiratory pressure and (f) a reduction in tidal volume during volume targeted ventilation.10,11
Indicators of inadequate gas conditioning are (a) insufficient humidifier water consumption, (b) extensive condensation in the inspiratory limb (rainout), (c) absence of condensate in the expiratory limb and (d) absence of condensate beading on the inner walls of the humidification chamber.
For neonates, endotracheal secretion suction is required every 6 h or as clinically indicated as part of regular care, using a closed suctioning device or, if the former is inadequate, an open suctioning system. This entire process should not take >15 seconds, and the suction pressure should not rise >100 mm Hg. Saline instillation during suctioning is not required, except in rare cases where secretions are very thick or clogged. 12
Methods
Our objective was to reduce the rate of endotracheal tube occlusion (ETO) during mechanical ventilation from an initial 85% to 60% over an 8-month period through standardisation of humidification. Non-respiratory morbidity and mortality were taken as balancing parameters. Patients were not directly involved in the design or implementation of our study. The team of healthcare providers engaged in the quality initiative consisted of the sister in charge, two senior nurses, one faculty doctor and two resident doctors.
We followed the WHO Point of Care Quality Improvement model in three phases:
An Observation phase of one month where baseline data on were reviewed, using a fishbone diagram to perform a root cause analysis (Figure 1). This determined the lack of a standardized protocol for humidifying gases during ventilation, doctors’ and nurses’ lack of awareness of warning signs, their lack of training in use of humidifiers, and their lack of motivation. The QI team proposed some prioritized correction activities afterwards (Figure 1). An Intervention phase of five months with an elaborate strategy to carry out several consecutive PDSA (Plan-Do-Study-Act) cycles to address issues highlighted. The creation of an extensive humidification checklist (Supplemental file), proficient training and active participation of healthcare personnel, the use of information, education and communication tools including posters, video recordings, targeted group discussions, informal peer group gatherings and multimedia – WhatsApp group formation were all components of these PDSA cycles. These were all evaluated, and accepted, modified, or rejected based on their practicality and results. A Sustenance phase of two months where the sustainability of QI project was examined by recording ETO rates.
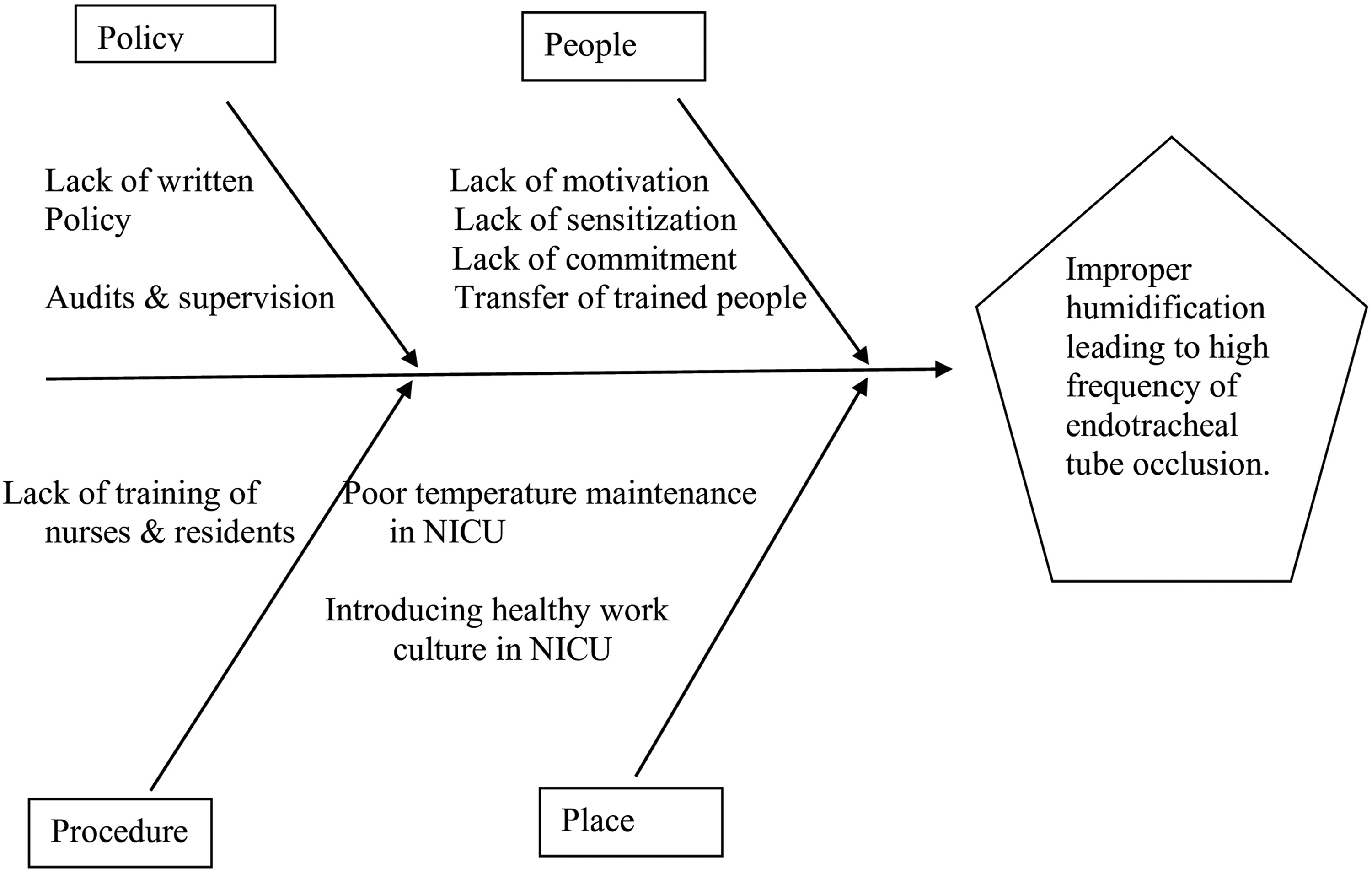
Details of root cause analysis. Fishbone diagram and its effect in neonatal intensive care (NICU).
Results
The QI initiative was implemented between January and August 2022. A total of 1474 neonates were admitted, of whom 84 required invasive mechanical ventilation. Figures 2 and 3 illustrate the chart of ETO rates with PDSA cycles alongside, showing a decreasing trend in ETO rate. At the end of the fifth PDSA cycle, this had dropped to 46%. Our sustainability assessment showed that this trend of decreasing ETO rates decreased remained at c.45% per week over the next 2 months. Mortality as well as non-respiratory morbidity used as balancing measures during the study period remained unchanged.
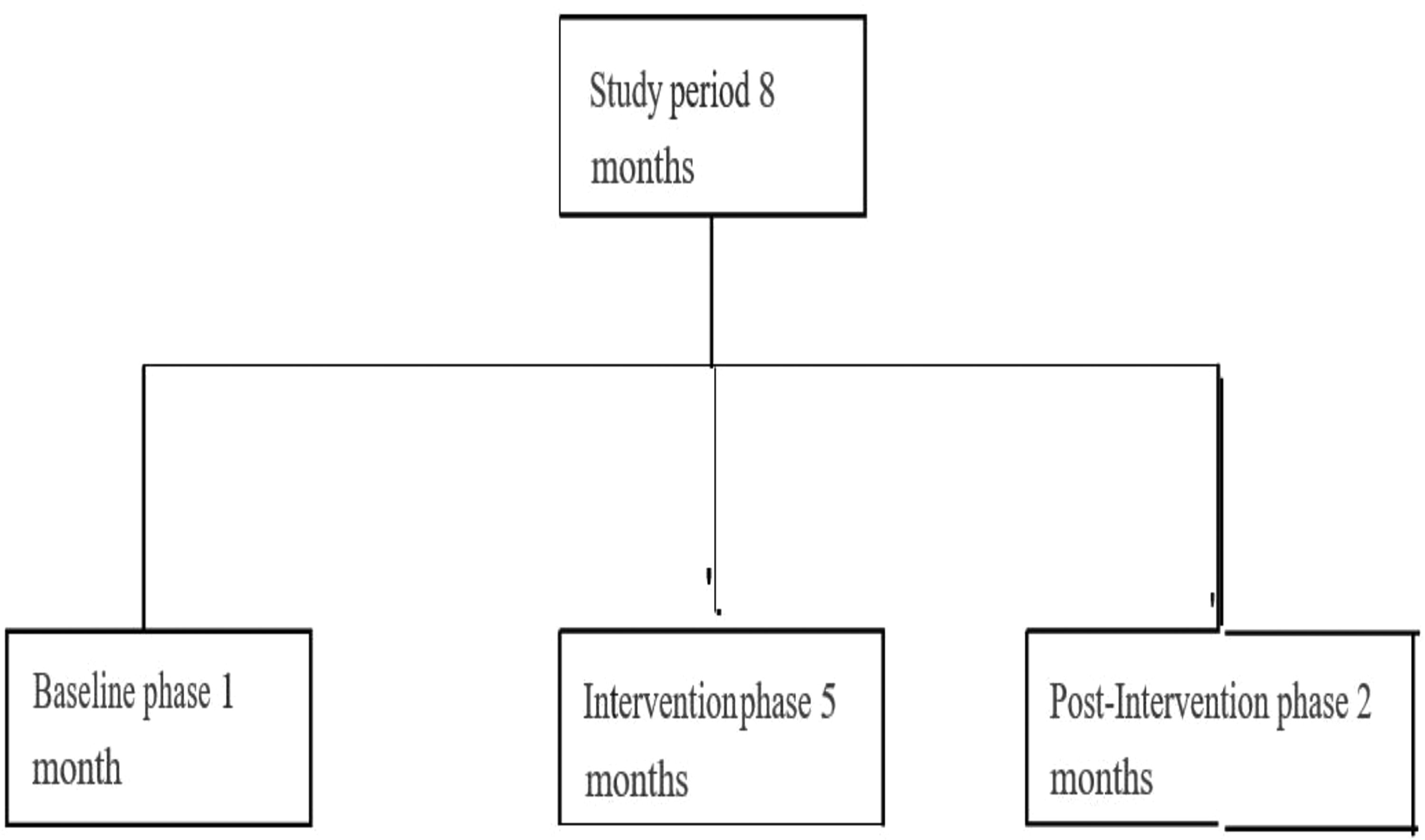
Study flow diagram describing total duration of study with base line phase of 1 month followed by intervention of 5 months and final post intervention for 2 months.

Run chart displaying average endotracheal tube occlusion rates in percentage on y-axis and duration of study in weeks on x-axis, furthermore figure narrates details of PDSA cycles with the interventions done. PDSA: Plan-Do-Study-Act.
Discussion
Our study was conducted in response to a pilot study which had revealed a consistent pattern of clinically significant ETO rate in our NICU. Standardisation of humidification was carried out using a checklist to regulate the ventilator gas flow rate, to check that the humidifier chamber contained sufficient water, to ensure that the airway temperature probe and chamber outlet probe were operating effectively, and to maintain the ambient air temperature in the NICU.
Typical errors made were updated for residents and nursing personnel. The ability to track each incident in real-time increased staff knowledge enabled the identification of correct practice, as well as monitoring adherence to defined process improvements.
Placing the airway temperature probe (ATP) outside the heated field of radiant warmer leads to negligible condensation (Figures 4 and 5). The unheated section of the inspiratory circuit distal to the ‘airway temperature probe’ (near the Y adaptor) experiences rapid cooling of inspiratory gases. This is primarily the result of prolonged low ambient temperature and low ventilatory flow rate. At high ambient room temperatures, the humidification of the gases is in fact quite poor. 13 Additionally, a humidifier lacks the ability to humidify inspired gases at high flow rates. 14 ‘Rainout’ in the ventilatory circuit is eliminated if the ambient room temperature is maintained between 24°C and 6°C and flow rates between 6 and 8 L/min. In fact, the ATP may register a higher temperature than the effective inspiratory gas temperature if it is placed in a heated field beneath a radiant warmer owing to radiation or convection heat produced by the warmer. This can bring about ‘rainout’ within the circuit as a consequence of the servo-controlled reduction of humidification chamber output (Figure 4). 15 Healthcare professionals need training on the significance of a variety of humidifier alarms (such as low-temperature alerts and alarms caused by malfunctioning humidifiers) and troubleshooting techniques.
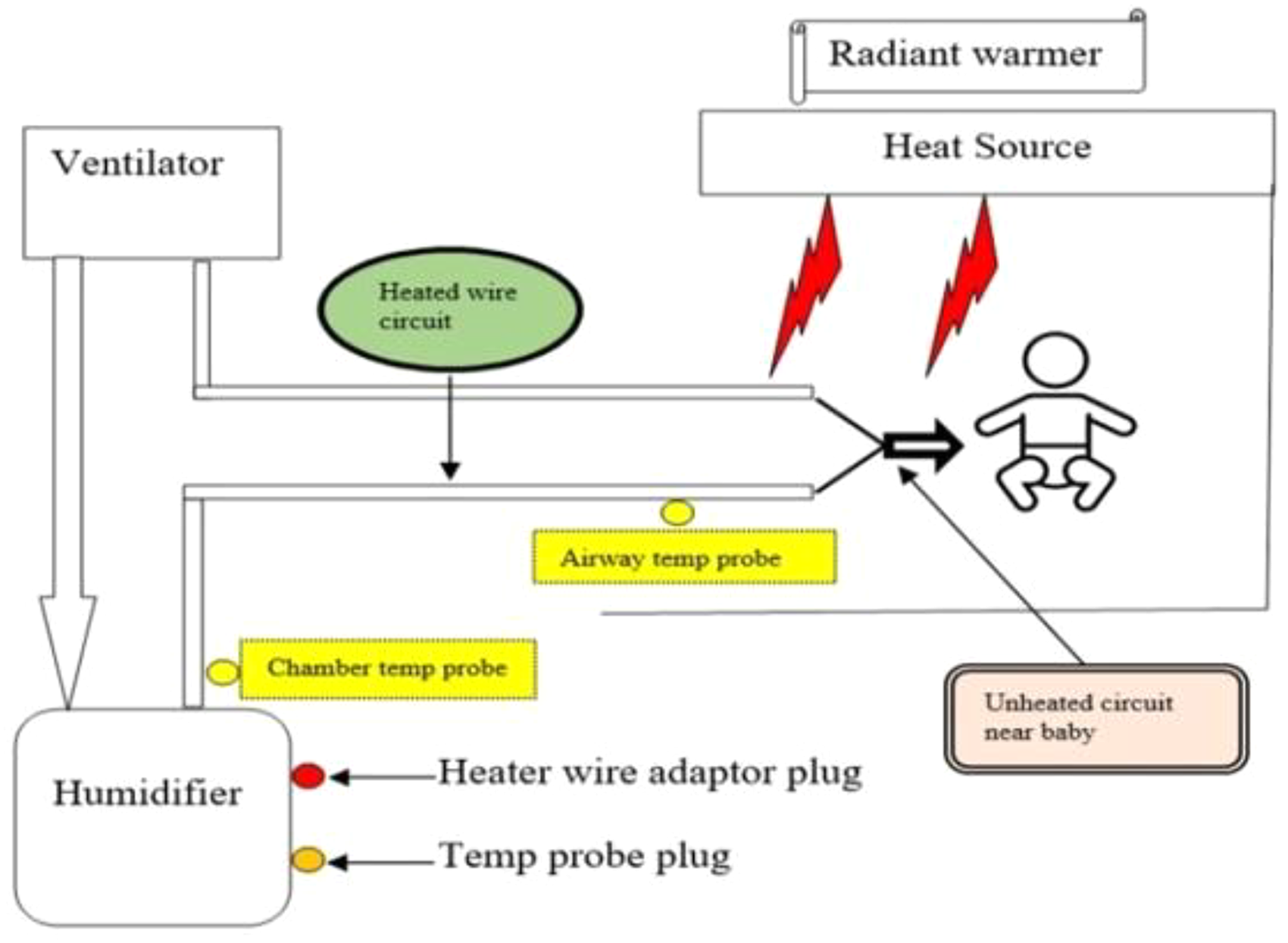
Components of humidification system and placement of air temperature probe away from the heat source (radiant warmer) to avoid condensation in the ventilatory circuit.
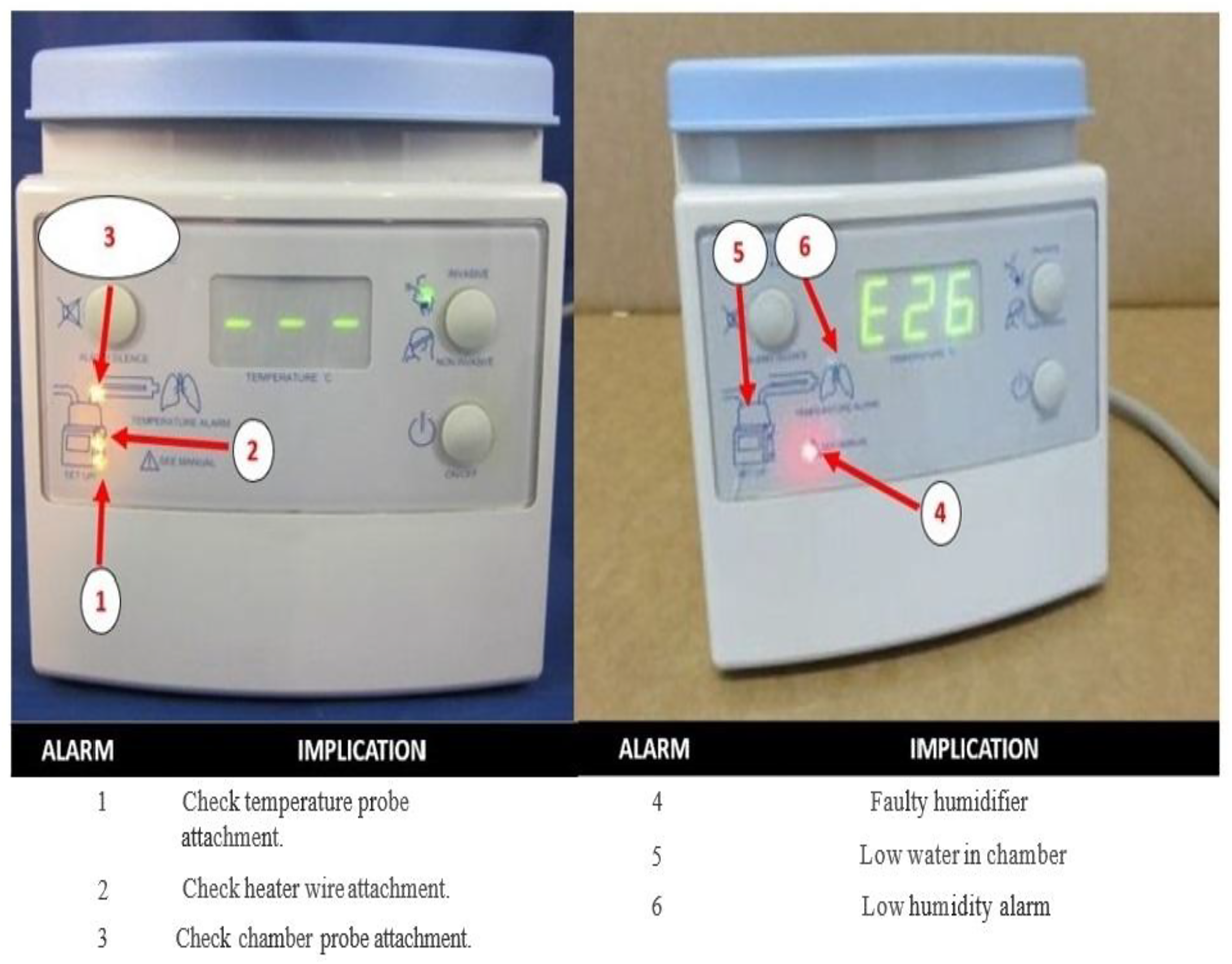
Displays various alarms of humidifier and its implications: (1) check temperature probe, (2) check heater wire, (3) check chamber probe, (4) faulty humidifier, (5) low water level in chamber and (6) low humidity alarm.
A change in ethos of shared responsibility in the unit thus developed. Implementing practical training sessions for healthcare workers, together with ongoing interactive educational training sessions, was the third driving force behind this quality improvement project.
We employed an audit and feedback approach to track alterations in team members’ behaviour and assess clinical performance. 16 By a fortnightly audit to determine what was accomplished, what was still needed to be done, where improvements were possible, and how the medical staff perceived their own performance, we could inspire team members by designating fortnightly quality champions and rewarding them with gifts as a token of appreciation. 17 To find new approaches to solve problems, we continued actively seeking new thoughts and feedback from new members.
Conclusion
Our study only involved one institution; we did not see problems such as ventilator-related pneumonia, prolonged ventilation and broncho-pulmonary dysplasia. However, we have demonstrated that a straightforward and practical quality improvement programme that can be implemented with currently available resources can have a beneficial impact on reducing the ETO.
Footnotes
Ethical approval
This project was registered as QI initiative and clearance from the institutional ethical committee was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.