
Abstract
Melioidosis is caused by the environmental bacterium Burkholderia pseudomallei and may recur months after apparent cure with fatal consequences. We report a previously healthy 31-year-old man with incompletely treated bacteraemic melioidosis who presented eight months later with recurrent chest wall abscess and fulminant pneumonia progressing to ARDS and death despite aggressive treatment.
Keywords
Case report
A 31-year old manual labourer was referred to our tertiary centre after two days of fever, pleuritic chest pain and rapidly worsening breathlessness. He had no chronic illnesses. At the referring hospital, he had been treated for severe community-acquired pneumonia. Eight months earlier, he had been diagnosed with bacteraemic melioidosis. Unfortunately, he had not completed the proposed eradication phase of treatment. He was awaiting review at the surgical clinic.
On presentation, he was in shock: hypotensive, tachycardic and severely hypoxaemic despite high-flow oxygen. He had coarse lung crepitations and a firm, tender mass on the right lateral chest wall without discharge. This was situated at the site of an abscess drained two weeks before.
He was immediately intubated and ventilated. A post-intubation antero-posterior chest radiograph showed bilateral diffuse alveolar infiltrates consistent with acute respiratory distress syndrome (ARDS) (Fig. 1). Empiric meropenem was commenced after obtaining blood cultures that grew B. pseudomallei. Despite such aggressive treatment, he died within ten hours of admission.
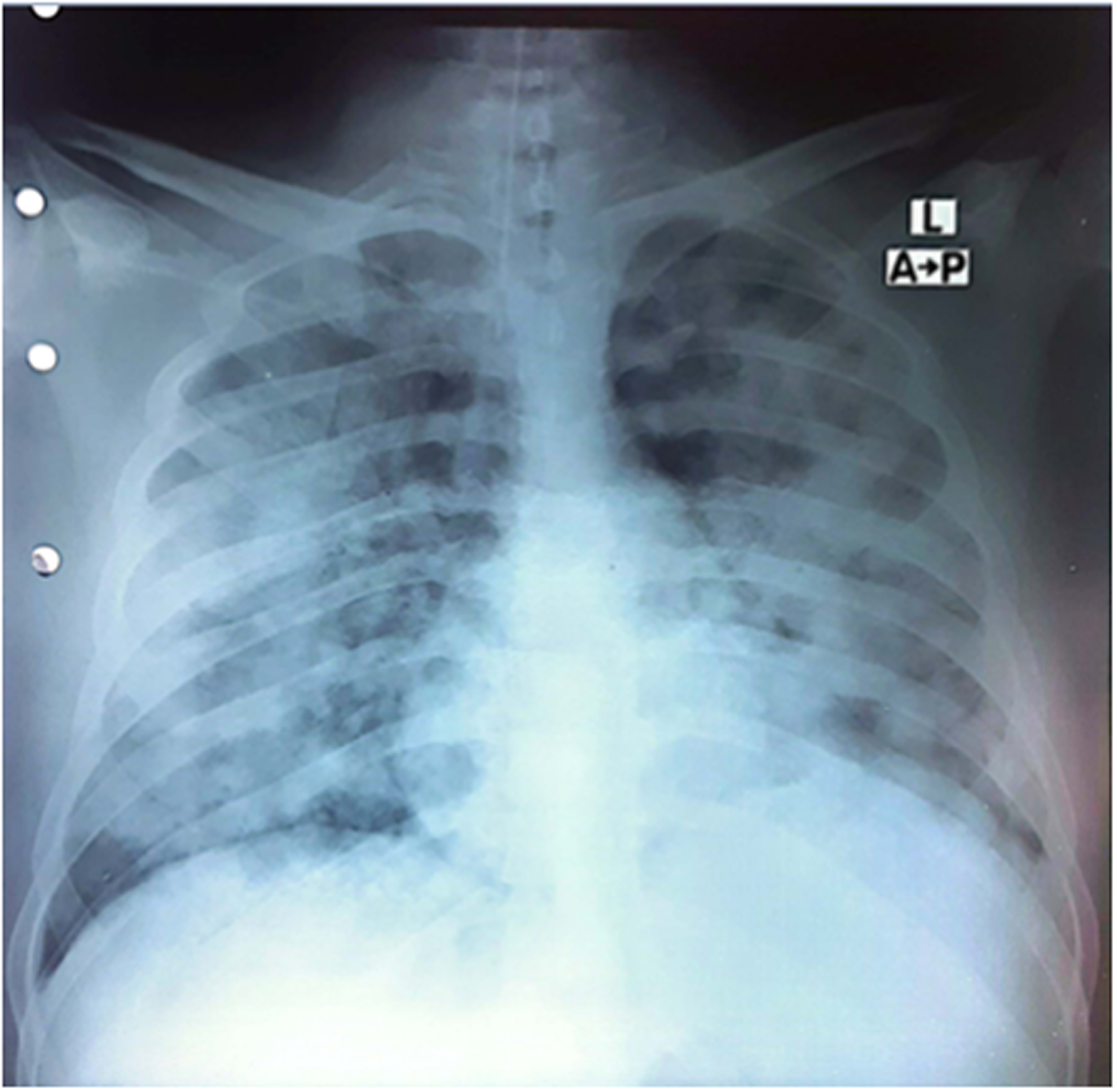
Anteroposterior chest radiograph showing diffuse alveolar infiltrates consistent with acute respiratory distress syndrome.
Discussion
Genotyping was unavailable, but the short interval between episodes and his premature cessation of therapy supported relapse rather than new infection. Melioidosis is an acquired infection through skin inoculation, inhalation or ingestion; clinical presentations include pneumonia, visceral or soft-tissue abscesses and septic shock. 1
Sri Lanka lies within the South-East Asian ‘melioidosis belt’, and cases occur across climatic zones. 2 Relapse most often follows premature discontinuation of oral eradication therapy. 3 Melioidosis carries a high case-fatality rate when presenting as severe pneumonia or septic shock. Standard care involves an initial intravenous phase (ceftazidime or meropenem for 2–4 weeks) followed by prolonged oral eradication therapy (usually co-trimoxazole for 12–20 weeks). Relapse occurs in 5–15% of cases despite appropriate therapy and is more frequent when oral therapy is curtailed. 4 Genotypic analysis of isolates from each episode is usually required to differentiate relapses from reinfections. 5
In our patient, the combination of a chest-wall abscess and rapidly progressive pneumonia should have prompted early consideration of melioidosis and immediate initiation of appropriate therapy. Completion of both treatment phases and regular follow-up is essential to prevent such relapse, which manifested as a fatal fulminant chest-wall abscess, pneumonia with ARDS in a previously healthy young man.
Footnotes
Acknowledgements
The authors thank the NIID intensive care unit (ICU) doctors and nursing staff for their dedicated patient care and the microbiology laboratory team for expeditious sample processing.
Ethics approval and consent to participate
Not applicable. This article reports a retrospective case; no experimental intervention was performed on the patient.
Consent for publication
As the patient is deceased, the patient's next of kin, as the patient's legal representative, provided written informed consent for publication of this case. No identifying personal details are disclosed in this report.
Author contributions
TP, DI, SM and TS were involved in the patient's clinical management. MK performed the laboratory diagnostics. TP, SM, NL and TS drafted the manuscript. NL provided critical revisions. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Not applicable. All data are contained within the case report.
Use of AI-assisted writing tool
ChatGPT (OpenAI) was used as an editorial aid for drafting and language refinement. All interpretations, analyses and final editorial decisions were made by the authors, who take full responsibility for the final manuscript.