
Abstract
South Africa’s Children’s Act 38 of 2005 requires health professionals to determine whether a child possesses ‘sufficient maturity’ and ‘mental capacity’ to make decisions about themselves in relation to surgery, treatment, and HIV testing. Similarly, the National Health Act 61 of 2003 requires a child to be ‘capable of understanding’ to provide informed consent in research. However, neither the Children’s Act nor the National Health Act defines these terms. Moreover, there is no common definition of ‘sufficient maturity’ among healthcare professionals in South Africa. Appreciating how foreign law interprets ‘mental capacity’ and how different healthcare professionals evaluate ‘maturity’ could prove illuminative in respect to how these terms could be interpreted by health professionals in South Africa, and elsewhere.
Healthcare decision-making requires individuals to exercise their right to autonomy (Singh, 2001). South Africa’s Children’s Act 38 of 2005 (as amended by the Children’s Amendment Act 41 of 2007) outlines the role of children, parents, and health professionals in making decisions about healthcare services for children (Mahery, Proudlock, & Jamieson, 2010; Republic of South Africa, 2005). While the Children’s Act of 2005 represents a significant attempt to protect and promote the rights of children in South Africa, the interpretation of some parts of the Act, such as those pertaining to consent by children for medical treatment, surgical operations, and HIV testing, is unclear. For instance, the Act makes several references to ‘mental capacity’ and ‘sufficient maturity’ and the child’s ‘capacity to understand the benefits, risks, social and other implications’ of treatment, surgery, and HIV testing. Similarly, the National Health Act 61 of 2003 requires a minor to provide their consent to participate in research if the minor is ‘capable of understanding’ (Republic of South Africa, 2003). However, ‘mental capacity’, ‘sufficient maturity’, and capability to understand are cognitive notions, and not defined in either of the Acts. Accordingly, what interpretation should be afforded to these terms?
The Children’s Act 38 of 2005
The Children’s Act 38 of 2005 specifies the child’s age of consent for medical treatment, surgical operations, HIV testing, and contraceptive use, as follows (Republic of South Africa, 2005):
(2) A child may consent to his or her own medical treatment or to the medical treatment of his or her child if- (a) the child is over the age of 12 years; and (b) the child is of sufficient maturity and has the mental capacity to understand the benefits, risks, social and other implications of the treatment. (Italics added for emphasis) (3) A child may consent to the performance of a surgical operation on him or her or his or her child if- (a) the child is over the age of 12 years; and (b) the child is of sufficient maturity and has the mental capacity to understand the benefits, risks, social and other implications of the surgical operation (italics added for emphasis); and (c) the child is duly assisted by his or her parent or guardian.
(2) Consent for a HIV-test on a child may be given by- (a) the child, if the child is- (i) 12 years of age or older; or (ii) under the age of 12 years and is of sufficient maturity to understand the benefits, risks and social implications of such a test. (Italics added for emphasis)
(1) No person may refuse to – (a) to sell condoms to a child over the age of 12 years; or (b) to provide a child over the age of 12 years with condoms on request where condoms are provided or distributed free of charge. (2) Contraceptives other than condoms may be provided to a child on request by the child and without the consent of the parent or care-giver of the child if- (a) the child is at least 12 years of age; (b) proper medical advice is given to the child; and (c) a medical examination is carried out on the child to determine whether there are any medical reasons why a specific contraceptive should not be provided to the child.
The above provisions highlight that the legislature imposes varying demonstrative burdens on children and health professionals in respect to different health procedures and interventions:
Treatment and surgery: (1) the child has to meet specified chronological age criteria, (2) demonstrate ‘sufficient maturity’, and (3) demonstrate ‘mental capacity’.
In the case of surgery, while the consent of the parent, guardian, or caregiver is not required for the surgery on a child over 12 years to proceed, the child lacks true autonomy as he or she must be ‘duly’ assisted by his or her parent, guardian, or caregiver in the decision-making process. The use of the word ‘duly’ places an obligation on the child’s parent, guardian, or caregiver to assist the child in an appropriate, proper, and meaningful manner in the decision-making process. Thus, a parent, caregiver, or guardian cannot simply rubber-stamp the child’s decision, but must properly apply his or her mind to the matter and advise the child accordingly. In a situation where the wishes of the child and parent/guardian/caregiver differ regarding surgery, the best interests of the child must be determined and a decision made accordingly, regardless of whether the child or parent is satisfied with the outcome.
HIV testing: (1) the child has to meet specified chronological age criteria and (2) demonstrate ‘sufficient maturity’.
Access to contraceptives: (1) the child has to meet specified chronological age criteria.
Participation in research: Where research or experimentation is to be conducted on a minor for a therapeutic purpose, the research or experimentation may only be conducted: (1) if the research is in the best interests of the child; (2) with the consent of the parent or guardian of the child; (3) in the manner and on such conditions, as prescribed (by the Minister); and (4) if the minor is capable of understanding, the research must be conducted with the consent of the minor. In addition to the above conditions being met, non-therapeutic research also requires the consent of the Minister (this function has since been delegated to Research Ethics Committees).
In the context of the National Health Act, ‘therapeutic research’ means ‘research that holds out the prospect of direct benefit to the participant’ while ‘non-therapeutic research’ means ‘research that does not hold out the prospect of direct benefit to the participant but holds out the prospect of generalizable knowledge’ (Republic of South Africa, 2013). These demonstrative burdens on the child occur in the context of the informed consent process. The ethical and legal elements of a valid consent process require the satisfaction of the following elements (Republic of South Africa, 2003; Singh, 2017):
Disclosure. The patient must be given comprehensive information including the risks and complications of the treatment as well as other diagnostic and alternative treatments options.
Understanding. The information should be simple and easily understood and communicated in way a way that is understood by the patient. This will include sensitivity to age, language, culture and disability.
Voluntariness. There should be no coercion or influence compelling the individual to consent or refuse treatment against his or her wishes or best interest.
Capacity refers to mental and legal capacity to consent. The individual should be in an appropriate frame of mind and intellectual capacity to be able to make an informed decision.
While the legal capacity requirements of the Children’s Act of 2005 are clearly defined with respect to specific contexts (treatment, surgery, contraception access, and HIV testing), the notion of ‘mental capacity’ is less clear.
What is ‘mental capacity’?
The notion of a child’s ‘mental capacity’ in relation to healthcare decision-making is not defined in South African law. Capacity in a health context relates to a clinical evaluation of an individual’s functional ability to make autonomous, authentic decisions about his or her own life (Derish & Vanden Heuvel, 2000). Put differently, the child’s mental capacity speaks to their decisional capability. It comprises two elements: (a) the capacity to assimilate relevant facts; and (b) appreciation or understanding by the patient of his or her situation as it relates to the facts (Derish & Vanden Heuvel, 2000). The child’s ability to communicate a choice has been proposed as an additional element (Appelbaum, 2007; Geist & Opler, 2010).
The United Kingdom’s Mental Capacity Act of 2005 provides helpful guidance in relation to how decision-making capacity can be determined (Table 1). In terms of Section 3 of that Act, to demonstrate decision-making capacity, a person should be able to
Understand the information relevant to the decision, including the purpose of any proposed course of action, the main benefits, risks and alternatives, and the consequences of refusing to follow the proposed course of action and of failing to make a decision.
Retain that information for long enough to make a decision.
Use or weigh that information as part of the process of making the decision.
Communicate his or her decision, whether by speech, sign language or any other means.
Additional recommended factors that should be considered in determining a child’s mental capacity.
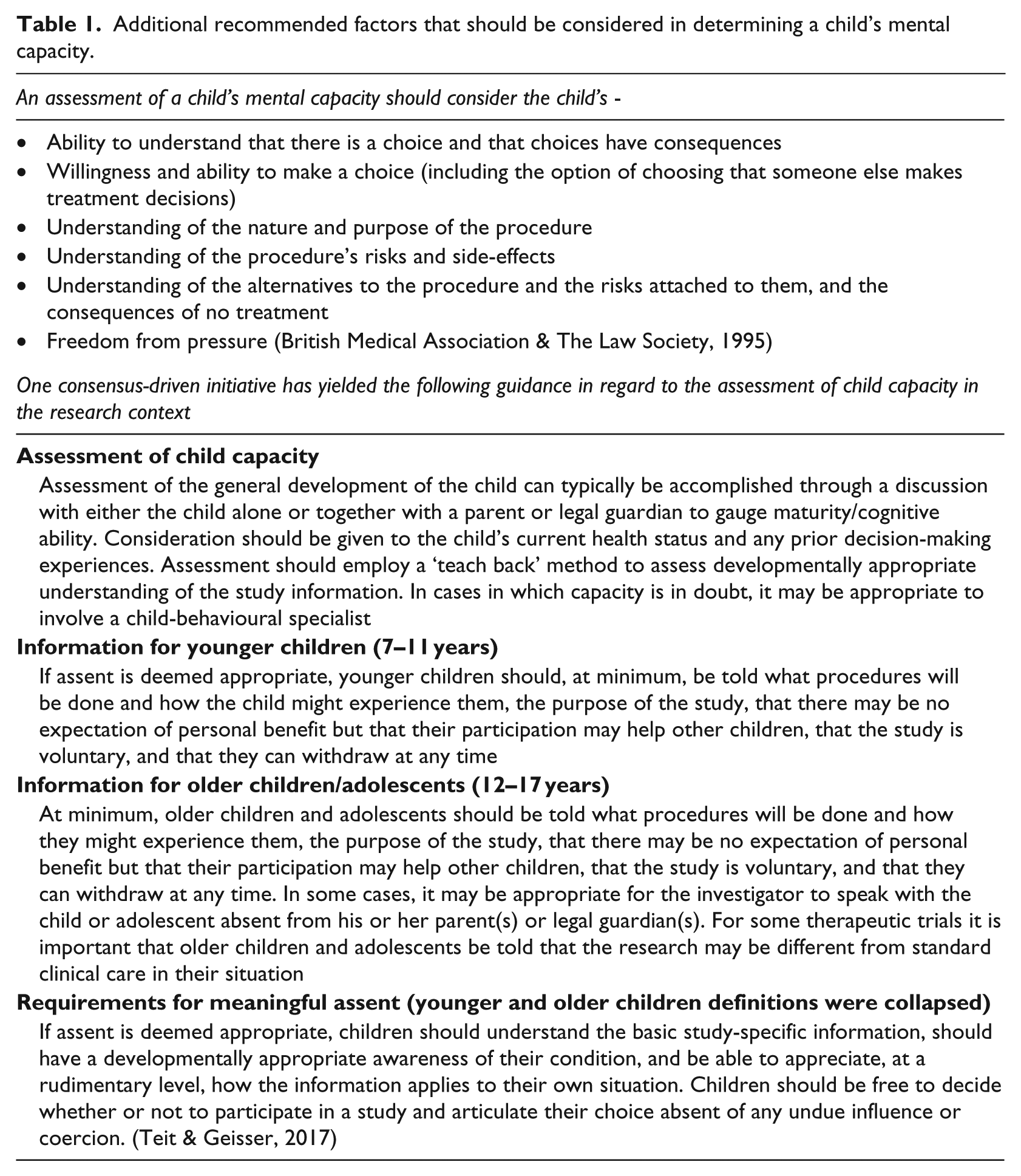
Health practitioners currently do not have clear guidelines on what determines decision-making capacity and rely on their clinical skills to make such judgements. The above criteria can serve as a useful guide to health professionals grappling with how to establish the mental capacity of a child in relation to healthcare and research decision-making.
What is ‘sufficient maturity’?
Article 12 of the Convention on the Rights of the Child (CRC) designates that ‘children shall be assured the right to express their views freely in all matters affecting them, their views being given due weight in accordance with the child’s age, level of maturity, and what is in their best interest’ (United Nations General Assembly, 1989). In terms of the CRC, ‘maturity’ refers to the ability to understand and assess the implications of a particular matter, and must therefore be considered when determining the individual capacity of a child. In the context of Article 12, it is the capacity of a child that allows him or her to express her or his views on issues in a reasonable and independent manner (United Nations General Assembly, 1989).
Although there is no common definition of ‘maturity’ among healthcare professionals, they generally subscribe to a developmental approach to maturity. The developmental approach, whether biological, psychological, or social, views the child as a developing organism who progresses from one stage to another in a sequential manner (Silvern & Fischer, 1985). The developmental progression ranges from infancy through early and later childhood, to adolescence, early adulthood, late adulthood, and old age. Particular developmental milestones and abilities accompany each developmental stage. These stages are often age-linked but there are instances where these stages are attained outside of the expected norm. Some children develop early (early developers), while others develop later (late developers). Various factors influence development, including gender, culture, the environment, and resources. Accordingly, it has been noted that there has been a shift in international thinking about decisional capacity away from age, to considering each child’s unique circumstances based on their experience and understanding (Alderson, 2007; Havenga & Temane, 2015).
The term ‘sufficient maturity’ is not defined in South African law. South Africa’s National Department of Health’s HIV Counselling and Testing Policy guidelines states that children are considered to be sufficiently mature if they can ‘demonstrate they understand information on HIV testing and can act in accordance with that appreciation’ (Department of Health, South Africa, 2010). It has been noted that while this description seems to suggest that cognitive ability determines maturity, maturity also includes levels of physical, emotional, and moral development (Havenga & Temane, 2015). For instance, it has been argued that children with personal experience, such as exposure to surgery, illness and hospitalisation, and healthcare are likely to have a better understanding of health-related matters (Alderson, 2007; Havenga & Temane, 2015). However, this must be tempered by appreciating that, overall, children have less experience as decision makers (Havenga & Temane, 2015). While disability and chronic illness increase children’s vulnerability and need for protection and special care, it has been argued that healthcare providers also consider that ‘hardships associated with disability and illness may increase not only children’s knowledge but also their skills and courage to deal with these hardships’ (Alderson, 2007; Havenga & Temane, 2015). It has furthermore been argued that healthcare providers should not automatically assume that children with learning difficulties are unable to make decisions (Wellesley & Jenkins, 2012). The same may be argued in relation to children who are socially disadvantaged. Outside South Africa, several analogous terms may prove illuminative in regard to how ‘sufficient maturity’ could be interpreted.
Mature minor
In the United States, the term ‘mature minor’ is used for a minor (under the age of 16 years) who is allowed to consent or refuse to consent to his or her medical treatment if it is established that the minor is sufficiently mature to understand, discern, and appreciate the benefits and risks of the proposed medical treatment (Cardwell v. Bechtol, 1987). In order for a minor to be considered mature, and therefore to have the capacity to consent to or refuse his medical treatment, there must be clear and convincing evidence that the minor fully understands the consequences of his or her actions. In making a determination the courts consider several factors such as the age, ability, experience, education, training, and degree of maturity or judgment of the minor, as well as the conduct and demeanour of the minor at the time of the incident involved. However, the courts have also warned that the ‘mature minor’ exception is not ‘a general license to treat minors without parental consent’, and that its application will depend upon the particular facts and circumstances of each case (Cardwell v. Bechtol, 1987).
Gillick competence
In the United Kingdom, the concept of ‘Gillick competence’ (Gillick v West Norfolk Wisbech, 1986) is used. Here, the courts determine whether children, less than 16 years of age, have sufficient understanding and intelligence to enable them to understand fully what is involved in a proposed intervention and the capacity to consent to that intervention (Department of Health, UK, 2009). However, it is implied, though, that the understanding required for different interventions will vary considerably, that is, a child less than 16 years of age may therefore have the capacity to consent to some interventions but not others. In addition, the Gillick concept applies to consent and not refusal of treatment. If a child is ‘Gillick competent’ but refuses treatment, such a refusal can be over-ruled either by a person with parental responsibility for the child or by the court (Department of Health, UK, 2009). This concept may be particularly useful to health practitioners working with children given the burdens imposed on health professionals by the legislature and the lack of training to assess mental capacity or sufficient maturity.
Emancipated minor
Emancipation is the legal process by which a child is released from the custody, control, and authority of his or her parents. The emancipation may be by voluntary agreement of parent and child, or implied from such acts and conduct as informed consent, it may by conditional or absolute, complete or partial, temporary or permanent (Cady, 1979). The emancipated minor is
allowed to conduct a business or any other occupation on his or her own behalf or for their own account outside the influence of a parent or guardian. The minor will then have full contractual capacity to conclude contract with regard to the business. (Cady, 1979)
It has been argued that minors who are ‘emancipated’, such as those who live independently from their parents, have their own children, or are married, may be more experienced decision-makers than their peers of the same age (Havenga & Temane, 2015; Kling, 2011). South African law recognises the notion of emancipation (Republic of South Africa, 2006; Republic of South Africa, 2009). Emancipation is usually determined by the ‘best interest of the child’. This is also a notion that is used or recognised in South Africa (Republic of South Africa, 1996; Republic of South Africa 2005; Republic of South Africa, 2006; Republic of South Africa, 2008).
Deciding on whether a child is mature enough to give consent requires that the child have full knowledge of the procedure, and understands the nature of the risk of the treatment or surgery – including the social or other consequences of the treatment or surgery (Mahery et al., 2010). It is then assumed that the child will be able to evaluate all the information provided by the health professional, retain this information, and determine which course of action is believed to be best, and then gives his or her informed consent to undergo a particular treatment or not to undergo any treatment (Marques-Lopez, 2006). From the foregoing it is clear that this is a very complex cognitive task and ability for a child. It is also important that the child is not coerced or forced into a choice.
Best interests of a child
Section 7 of the Children’s Act contains a long list of the factors to be taken into consideration when deciding on the ‘best interests of the child’. Some of these factors may be helpful determinants for ‘sufficient maturity’. These include:
7. (g) the child’s – (i) age, maturity and stage of development; (ii) gender; (iii) background; and (iv) any other relevant characteristics of the child; (h) the child’s physical and emotional security and his or her intellectual, emotional, social and cultural development; (i) any disability that a child may have; (j) any chronic illness from which a child may suffer; (k) the need to protect the child from any physical or psychological harm that may be caused by – (i) subjecting the child to maltreatment, abuse, neglect, exploitation or degradation or exposing the child to violence or exploitation or other harmful behaviour; or (ii) exposing the child to maltreatment, abuse, degradation, ill-treatment, violence or harmful behaviour towards another person; (iii) any family violence involving the child or a family member of the child; . . . .
Subsections k (i–iii) are important as children in abusive, violent, and traumatic environments and relationships are often powerless, and, accordingly, unable to make autonomous decisions. Psychologically, many children will not able to make choices independently. The powerlessness contributes to the victims of abuse trauma engaging in denial and repression. With their environment characterised by fearfulness, control, and emotional neglect, the victim is often without power, strength, control, and hope.
How do different professional disciplines evaluate the notion of ‘sufficient maturity’?
Healthcare professionals generally subscribe to a developmental approach to maturity (Jensen, 2008). The developmental approach, whether biological, psychological, or social, views the child as a developing organism who progresses from one stage to another in a sequential manner. Rutter and Rutter (1992) use the following as a working definition of development in relation to humans: ‘systematic, organized, intra-individual change that is clearly associated with generally expectable age-related progressions and which is carried forward in some way that has implications for a person’s pattern or level of functioning at some later time’. The developmental progression ranges from infancy through early and later childhood, to adolescence, early adulthood, late adulthood and old age (Hurlock, 2001). Particular developmental milestones and abilities accompany each developments stage. These stages are age-linked and there are often age discrepancies as to when these stages are attained. Some children develop prematurely (early developers) while others delayed (late developers). Various factors influence normal development including gender, culture, environment, and resources. For those who do not successfully achieve a stage, developmental delays occur and sometimes the child may never attain the milestone or proceed to the next stage. In some instances, a child who may have developed normally may regress to an earlier stage as a result of stressors, traumatic events, or illnesses (Cunningham, Kliewer, & Garner, 2009; Evans, Kim, Ting, Tesher, & Shannis, 2007; Kliewer & Sullivan, 2008; Lengua, 2002). Developmental stages are usually based on particular theories that form the bases for evaluating delays or deviation from normal milestone development (Salkind, 2002).
There is no common definition of ‘sufficient maturity’ among healthcare professionals in South Africa or elsewhere. However, understanding how healthcare professionals of different disciplines evaluate this concept could prove illuminative in respect to how ‘sufficient maturity’ could be interpreted.
General medical practitioners
The medical practitioner’s assessment of a child focuses mainly on the physical development of the child (de Onis, Garza, Onyango, & Martore, 2006). Usually a medical evaluation, which includes a thorough history of the child’s development from caregivers and observations, provide the basis for the evaluation. As part of the history, emotional and scholastic aspects of the child may be gleaned. This evaluation is referenced against an acceptable norm for the child (Kaliski, 2006). Medical practitioners, particularly those trained to work with children who have been abused, should evaluate the child’s mental ability to understand the benefits, risks, social, and other implications of the treatment based on verbal feedback from the child, caregivers, and other individuals associated with the child. They will also evaluate abuse by physically examining the child and on information asked or provided to them. While this may be largely associated with physical and sexual abuse, emotional abuse may also be considered. The clinician will try to establish if the child’s physical and emotional functioning is within the norms that are acceptable for the child’s age, and if the child has an understanding of the procedures and outcomes based on what the child reports back (Pearce, 2002). While the medical examination provides very useful information about the bio-physical condition of the child, determining mental capacity or ‘sufficient maturity’ of the child is a subject determination based on the knowledge and experience of what is expected of children at various developmental stages.
Psychiatrists
Psychiatrists, being medically trained, may undertake a physical evaluation of the child. However, their assessment is usually based on the Clinical Interview and Mental Status Examination (MSE) and collateral information. The information is gathered through verbal feedback from the child, caregivers, and sometimes from other collateral sources. Key concerns for the psychiatrist are the presence or absence of a psychiatric disorder, how the psychiatric condition impacts on the function of the child and whether it will affect the child’s decision-making capacity. A psychiatrist will evaluate mental capacity to understand the benefits, risks, social, and other implications of the treatment (Munro, 1998), which is done by corroborating the information obtained with the expected development for the child. Psychiatrists also evaluate abuse because some psychiatric disorders may be associated with abuse, may contribute to regressed functioning, and often present as a co-morbid disorder.
Social workers
Social workers routinely assess children for the courts (Holland, 2000). Their assessment is based largely on an interview with their client and other relevant people. Information is obtained from several social and relational sources. Other methods include observations in group contexts and visits to various environments, such as the home, school, and areas that the child frequents. Maturity is determined by establishing whether the child’s social behaviour and functioning is in keeping and commensurate with development of other children the same age, and is in keeping with what is expected for the child stage of development. Social workers routinely evaluate for all forms of abuse (Howe, 1992; Munro, 1999; Tredoux, Foster, Allan, Cohen, & Wassenaar, 2005). The validity and reliability of such an evaluation is similar for any interview method and is dependent on the skill of the practitioner and information sources used.
Clinical psychologists
Clinical psychologists, in addition to the use of a Clinical Interview, MSE and collateral history, usually administer several psychological measures and assessments (Groth-Marnat, 2003). Such measurements are questionable on the grounds of reliability and validity. Intellectual assessment, using both objective and projective assessments and/or developmental scales, are basic measures employed, particularly as this evaluation directly determines the child’s capacity to understand and make decisions. An intellectual assessment will also provide a good indication of the mental age of the child. Chronological age is not always consistent with mental age. For psychologists, maturity involves the child’s stage of development and this necessitates evaluating intellectual, emotional, physical, social, cognitive, moral, and cultural functioning. In addition, culturally sensitive personality and neuropsychological tests are used (Anastasi, 1988; Lezak, Howeison, & Loring, 2004). Mental capacity to understand the benefits, risks, social, and other implications of the treatment also involves formal, objective assessment of psychopathology, cognitive maturity, cognitive impairment, judgment, and personality influences (Boyer, Hitelman, Knolls, & Kafkalas, 2003; Spreen & Strauss, 1998). Disability and vulnerability are evaluated and considered with regard to the impact of the physical and psychological disabilities (Birmes et al., 2009), all forms of abuse, history of violence and trauma (Boals & Schuettler, 2009; Bokszczanin, 2007; Breslau, 2009; Christian Lawyers Association v. Minister of Health and Others, 2005), risk and resilience, and personality factors predisposing and/or exacerbating the child’s functioning. In this regard, psychologists will determine aspects such as intellectual ability, memory, attention and concentration, reasoning, information processing, verbal comprehension, communication (receptive and expressive), cultural influences, social context, and the ability to communicate. However, such assessments are not as simple and straightforward as they may appear given challenges with test reliability and validity. Therefore, substantial work is still needed to develop and adapt psychological tests to enable adequate and accurate measurements of the concepts outlined here (such as the notion of ‘maturity’) (Lezak, Howeison & Loring, 2004).
From the forgoing discussion, other than the clinical psychologist, most healthcare practitioners rely exclusively on interviews and collateral information to assess a child’s maturity and the focus of the assessment is very specific to their training and discipline. While the clinical interview involves a heterogeneous collection of techniques, there is a dependence upon the verbal reflections of the individual, on contingent questioning, and on the creativity of the individual interviewer. These techniques do raise many controversial methodological questions, since reflection, contingency, and creativity are unorthodox from the perspective of the standardised objective, replicable scientific method (Swanson, Schwartz, Ginsburg, & Kossan, 1981). In addition, while the skills of some health professionals, especially those working with abuse and trauma may be better honed, their scope of practice may preclude them using such information.
A critical object of determining ‘sufficient maturity’ is cognitive ability and functioning. Clinical psychologists, in addition to the clinical interview and collateral history, use psychological assessments and tests to measure cognitive abilities and functioning. While sufficient maturity may be ‘inferred’ from cognitive functioning, it is important to acknowledge that not all developmental tests are apt for low and middle-income countries, such as South Africa. Furthermore, such tests do not necessarily produce results that equate to, or are calibrated to correspond with, the notion of ‘sufficient maturity’ articulated in law. Further work is needed to synergise the understanding of this notion in the fields of law and psychology. Unfortunately, there are insufficient psychologists in South Africa to attend to the huge number of sexual abuse and other child forensic cases. In order to improve the access of children to such services, a simple approach to determine sufficient maturity is required and which most healthcare workers may easily use.
Determining ‘social maturity’
The notion of ‘maturity’ also has sociocultural dimensions. In Bangladesh, for example, the age of maturity is considered to be 18 years of age extendable to up to 21 years, and is akin to the legal age of Majority (when the individual is deemed to be an autonomous adult). However, in terms of Hanifi law in that country, the age of maturity is 15 years of age, which is the notion that is used in the context of marriage, divorce, and dowry (Nemat, 2006). From the foregoing discussions on maturity, it appears that certain assumptions are made about capacity to consent. For a patient to have the capacity to consent or refuse medical treatment he or she must be able to understand the information relevant to the decision, retain the information long enough to make a decision, weigh the information and make a choice, and communicate the decision. For ‘mature minors’ or ‘emancipated minors’ and precedent in case law governing consent to treatment, as in the case of Gillick (Gillick v. West Norfolk and Wisbech, 1986) and Christian Lawyers Association v Minister of Health and Others (Christian Lawyers Association v. Minister of Health and Others 2005) ability, experience, education, training, and degree of maturity or judgment of the minor, as well as the conduct and demeanour of the minor is considered, as well as if the minor has sufficient intelligence and understanding to enable him or her to understand the treatment and implications of treatment. Furthermore, information provided to a child must be relevant, in a format that is accessible, and giving due consideration to the needs of the disabled (Republic of South Africa, 2006).
In the light of the above in order to provide an evaluation of ‘sufficient maturity’ the following factors must be considered:
Intellectual functioning (to establish intellectual capacity so as to fully comprehend the nature of the situation at hand, so as to develop apposite insight and respond appropriately).
An evaluation of abnormal behaviour or psychopathology (identify psychopathology that may interfere with the child’s ability to adequately understand as well as treat the condition so that the child may be able to do so).
Cognitive functioning (which would include memory, attention and concentration, reasoning, information processing, verbal comprehension).
Social and emotional functioning (to consider whether the child has stage-appropriate social and emotional development to understand and make an informed decision. This will include moral development).
Personality development – which will include an assessment of impulse control, expressive acts, interpersonal conduct, cognitive style, self-image, object representations and regulatory mechanisms.
Disability and vulnerability (being aware that a child with disability including mental and cognitive disorders is not automatically excluded).
Cultural practices and concerns including the evaluation processes and norms.
Ideally, a multidisciplinary team should conduct such an evaluation. However, this is not always possible as some situations may require a health professional to see the patient for the first time at a health facility and determine maturity. At other times, given the complexity of the issue, intervention or procedure, a child may have the capacity to consent to some interventions but not others. If any health professional is not confident that he able to determine maturity in respect of the seven points above, then he should solicit the help of other healthcare professionals to assist in the decision (see Table 2 for an overview of how different disciplines determine maturity of a child).
Professional assessments of ‘sufficient maturity’.
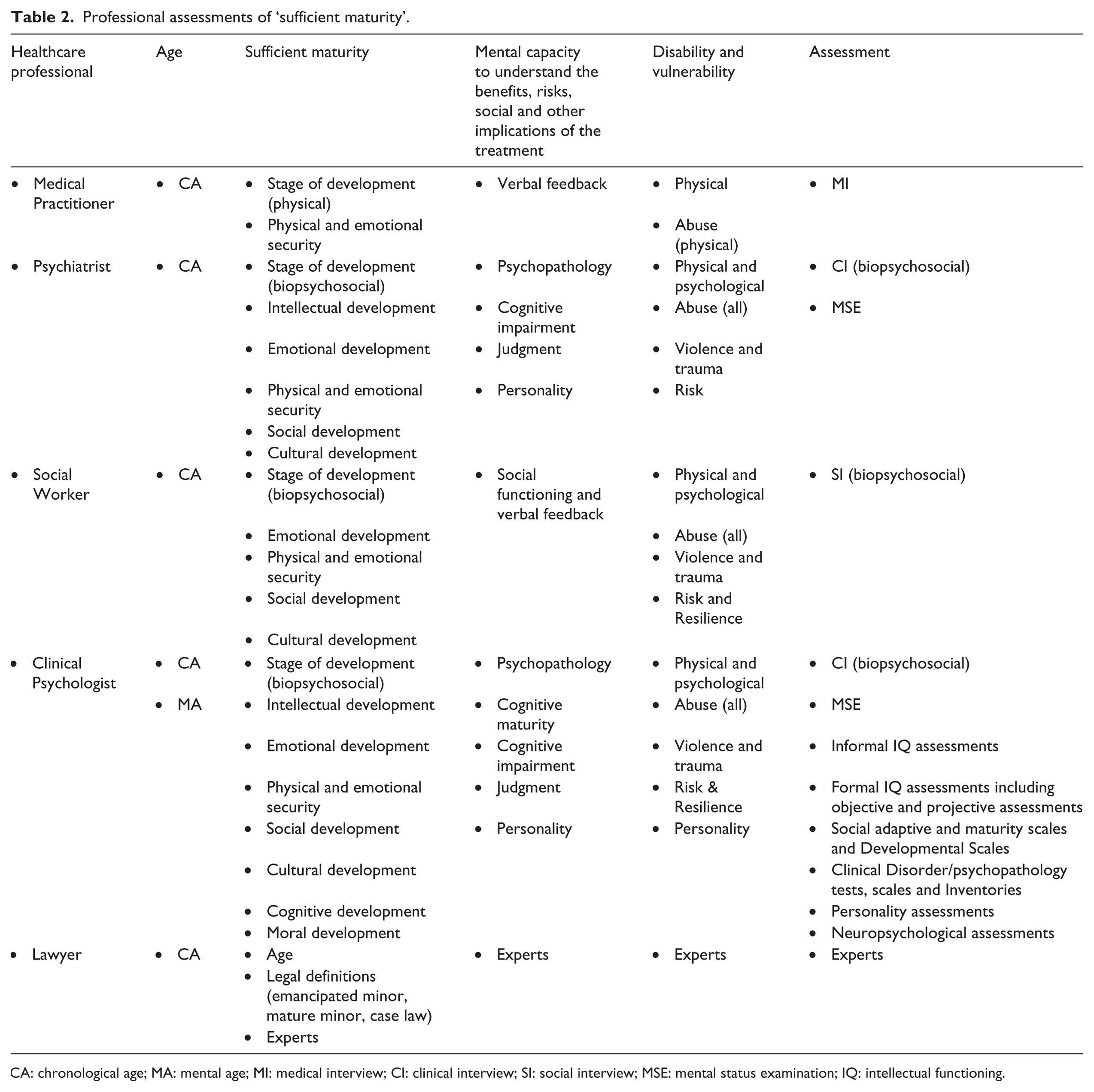
CA: chronological age; MA: mental age; MI: medical interview; CI: clinical interview; SI: social interview; MSE: mental status examination; IQ: intellectual functioning.
Other factors to consider
Several other factors may impact on a child’s decision-making capacity (Havenga & Temane, 2015). This includes the health professional’s personal beliefs and attitudes about children’s rights, and involving children in treatment-related decision-making. These belief and attitudes are sometimes shaped by the health professional’s own sociocultural, demographic, and religious characteristics. Parental involvement, attitude, and support may also influence children’s capacity to consent. Finally, the complexity and magnitude of the diagnostic test, medical treatment or surgical procedure influences the level of maturity required by children. In this regard, different levels of understanding and responsibility are required for different types of treatments or procedures (Havenga & Temane, 2015).
Conclusion
The terms ‘mental capacity’ and ‘sufficient maturity’ are not defined in South Africa law. However, knowledge of how international law, other countries legal systems, proposed clinical guidelines, and different disciplines of health professionals approach these concepts, could prove illuminative to practitioners grappling with these notions.
Footnotes
Acknowledgements
The authors thank Arisha Balkaran and Faadiela Jogee for their editorial assistance in preparing this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Jerome Amir Singh receives support from the Centre for the AIDS Programme of Research in South Africa (CAPRISA), which forms part of the Comprehensive International Program of Research on AIDS funded by the National Institute of Allergy and Infectious Disease at the National Institutes of Health and the US Department of Health and Human Services. He also receives support from the Bill and Melinda Gates Foundation and the HIV Prevention Trial Network. None of these funders funded this study.