
Abstract
Bullying is an environmental workplace stressor that has severe implications for the bullied individual and the organisation. Nurses within Southern African hospitals face unique challenges, which can foster an environment within which bullying flourishes. In particular within public hospitals, there are shortages of doctors, equipment, and basic resources, and hospitals are grossly understaffed. This study investigated the effect of workplace bullying on nurses’ sense of well-being, their job satisfaction, and propensity to leave. The effectiveness of social support as a moderator of the impact of bullying was considered. A self-report questionnaire was completed by 102 nurses from a public hospital in Zimbabwe. Moderated multiple regression analyses were conducted on each of the outcomes of bullying. Workplace bullying was found to have a significant impact on the outcomes measured. Higher levels of bullying were associated with lowered job satisfaction and greater propensity to leave. Social support within the sample under study did not influence these outcomes, but did influence mental well-being as a moderator. At low and medium levels of experienced bullying, high levels of support promoted higher well-being than low and medium support. But this was not the case when there was a high level of bullying, where there was no difference in mental well-being as a function of the level of social support.
Nurses play a critical and central role within the health care sector. Yet, the health care organisations within which they are expected to function at an optimal level are characterised by a number of negative factors. Workplace bullying (WPB) has been identified as a particularly widespread negative factor that is evident within this sector (Kwan, 2016). Research on bullying conducted in the health care sector has indicated that it is a crippling and severe social problem for health care employees and organisations. While prevalence rates vary across countries and cultures, the mental and physical implications for individuals may be so devastating that the organisations in which such bullying is taking place are duty-bound to address them (Berry, Gillespie, Gates, & Schafer, 2012; Nielsen & Einarsen, 2012). Berry et al. (2012) note that bullying among nurses has been reported to be in the range of 27%–70% of samples questioned. Research has demonstrated a strong correlation between WPB and poor mental well-being, lowered job satisfaction and increased intention to leave (Nielsen & Einarsen, 2012). According to Hutchinson, Vickers, Wilkes, and Jackson (2010), as many as 80% of Australian nursing professionals have experienced bullying during their careers. Furthermore, WPB is 16 times more likely to occur in the health care sector as compared to other organisational sectors (MacIntosh, Wuest, Gray, & Cronkhite, 2010). The impact of bullying upon nurses may significantly undermine their ability to deliver safe and effective health care. In many instances, nurses may choose to leave the profession in order to escape its aftermath (Wright & Khatri, 2015).
Research has identified a number of antecedent environmental conditions that enable bullying behaviour to develop. Utilising Einarsen’s model (2000), organisations with a culture of tolerance towards bullying behaviours and a lack of protective policies and procedures can create an environment in which bullying can flourish. Within the nursing environment, lack of resources and work overload, in particular, are identified as exacerbating antecedent stressor conditions (Glazer & Gyruk, 2008). While inadequate resources are a worldwide problem within nursing environments, within African hospitals, the lack of resources has reached crisis level (Sibanda, 2015; Steenkamp, 2014). Extremely poor infrastructure and an overall lack of funding which contributes to a lack of medical supplies, equipment, or broken equipment are endemic in African public hospitals, and Zimbabwe is no exception. Furthermore, shortages of qualified nursing staff exacerbate the workload of those who are employed (Sibanda, 2015), creating an environment of excessive demand which enables bullying to thrive.
A number of researchers, including Einarsen (2000), have noted that organisational sources of social support can moderate the relationship between WPB and individual and organisational outcomes (Rodwell, Demir, & Flower, 2013; Schirey, 2004; Trépanier, Fernet, & Austin, 2016). However, most of this research has been carried out in countries where public hospitals are considerably better resourced than African hospitals. Very little research has examined the pervasiveness of bullying and the effectiveness of social support as a moderator in the bullying–outcome relationship within Zimbabwean hospitals. Considering the extreme crisis plaguing the nursing sector within Zimbabwean public hospitals (Sibanda, 2015), this research aimed to explore the extent of bullying in a Zimbabwean hospital and to test whether social support is effective in buffering the bullying–outcome relationship. Given the crisis of staff shortages in Zimbabwean hospitals (Sibanda, 2015), identifying effective resources that can moderate the bullying–outcome relationship is crucial in order to stem the flow of nurses leaving the profession.
Defining WPB
According to Nielsen and Einarsen (2012), WPB is defined as a form of aggression where direct or indirect acts lead to an employee being systematically subjected to degrading and disrespectful treatment. WPB takes place relatively often and over a period of time, and is, thus, a chronic stressor. Typical WPB behaviours entail exposure to verbal aggression, physical intimidation, being attacked personally or professionally, having one’s work obstructed, over-checking of one’s work, being given the ‘silent treatment’, being socially isolated from the rest of one’s work group, having rumours spread about oneself, and/or being made the ‘laughing stock’ by being subjected to belittling verbal or physical acts of humiliation and denigration. It is, thus, evident that WPB can be conceived of as a harsh form of social control that is experienced as cruel and even traumatic, exposing nurses to severe physical and psychological outcomes (Berry et al., 2012).
Outcomes of WPB
Agervold and Mikkelson (2004) note that bullied individuals suffer impaired psychological well-being, increased levels of anxiety and fear, lowered self-esteem, lowered self-efficacy, and lowered belief in their professional competence. Bullying has also been implicated in severe mental health problems such as major depressive disorder (MDE), symptomology that resembles post-traumatic stress disorder (PTSD), and even leads to suicide (Rugulies et al., 2012). Physiological outcomes may manifest in sleep disorders and musco-skeletal problems (Hoch, Mikkelsen, & Hansen, 2011). Such severe individual implications, in turn, have serious organisational outcomes as victims experience reduced job satisfaction, lower commitment to the organisation, and increased intention to leave, with many victims actually choosing to leave their jobs in order to escape victimisation. For those who stay, there is often evidence of increased absenteeism due to physical or mental illness or in order to avoid exposure to bullying incidents. These outcomes may severely impact on patient safety and the quality of care (Trépanier et al., 2016). Wright and Khatri (2015) reported significant relationships between WPB and medical errors. The impact of WPB on both victims and patients is, thus, of considerable concern, and research that is directed at determining mitigating factors is of profound importance.
Antecedents of WPB
There are a number of antecedent environmental conditions that can foster bullying. Wright and Khatri (2015) note that authoritarian management with its rigid rules and procedures are prevalent in the health care sector. They also note that the health care sector is characterised by a long-standing paternalism in which nursing staff are oppressed by management. This oppression leaves nurses feeling powerless, and in the face of such powerlessness, anger, aggression, and frustration are deflected towards others, particularly those who are less powerful than themselves. Typically, in such instances, senior nurses will bully lower level nurses or a group of nurses may target a single individual at the same job level.
Social support as a moderator of the bullying–outcome relationship
One possible resource that can moderate the WPB–outcome relationship is that of social support. Social support refers to behaviours that are given to recipients by ‘providers’ from within the recipient’s social network. Within the work context, support can be provided by colleagues, supervisors, and even subordinates. Such behaviours are, for example, showing caring and concern towards the recipient and being prepared to provide relevant information, positive appraisals, and even tangible, instrumental assistance to the recipient at times when the recipient is experiencing stress (Bernstein, 2013).
In the context of WPB, social support serves numerous functions: enabling venting to a sympathetic ear, feeling cared for, receiving relevant information, validating experiences, and suggesting ways of handling the problem. Such support can bolster the WPB targets’ self-esteem, calm their anxiety, and enable a source of resolution. A number of researchers have indicated that social support from work sources is inversely related to negative outcomes among nurses (Rodwell et al., 2013; Schirey, 2004; Trépanier et al., 2016). For example, in a study conducted on 1100 nurses within the United Kingdom, Quine (2001) found that bullied nurses who had a high degree of social support at work reported lower levels of depression, lower intention to leave, and higher job satisfaction as compared to those with a low degree of social support.
Based on the above review of the literature, the extent of antecedent environmental/economic stressors within the public health system in Zimbabwe, and the paucity of research on the topic, the aim of this study was to gauge the perceived prevalence of WPB in a public hospital in Zimbabwe. We aimed to investigate whether bullying affects a number of indices of mental and occupational well-being, namely job satisfaction, propensity to leave, and mental well-being. In addition, the effectiveness of social support in moderating the effect of bullying within this context is examined.
Methods
Participants
The sample consisted of 102 nurses from a hospital in Zimbabwe. The majority were female (79.4%) and Black (96.1%). Three participants described themselves as mixed race, and one nurse did not answer this question. The sample ranged in age from 21 to 64, with a mean of 32.5 (SD = 8.9) years. The majority (69.6%) reported their home language to be Shona, 15.7% spoke Ndebele, and 5.9% spoke English. Most of the nurses (83.3%) had worked in this hospital between 1 and 10 years, with 14.7% having worked there longer than 10 years and only 7.8% had less than 1 year tenure. This closely mirrored their general nursing experience, with 81.4% having nursed for between 1 and 10 years, 16.6% more than 10 years, and 2% less than 1 year. In the sample, 52% were senior nurses, 12.7% were junior nurses, and 35.7% were student nurses.
Instruments
The self-report questionnaire consisted of a section requesting demographic information followed by scales measuring experience of bullying, job satisfaction, mental well-being, propensity to leave, and social support.
Experiences of bullying
This was measured using the revised Negative Acts Questionnaire (NAQ-R), developed by Einarsen, Hoel, and Notelaers (2009). The scale consists of 22 items. Participants are asked to indicate on a five-point time dimension whether, during the last 6 months, they had experienced the act in question: (1) Never, (2) Now and then, (3) Monthly, (4) Weekly, or (5) Daily. An example of a negative act is ‘Being humiliated or ridiculed in connection with your work’. The scale may be divided into a number of factors (work-related bullying, person-related bullying, and physically intimidating bullying). However, the developers argue that the 22 items may be combined into a single score, where a high score indicates the experience of high levels of bullying. Einarsen et al. (2009) obtained a Cronbach’s alpha of .90 for the full scale. In this study, the reliability of the scale using Cronbach’s alpha was found to be .947.
Job satisfaction
The Job Satisfaction Scale (JSS) developed by Warr, Cook, and Wall (1979) was used to measure this construct. This scale has been widely used across numerous countries. The scale has generally been regarded as encompassing two factors (intrinsic and extrinsic). However, recent research by Heritage, Pollock, and Roberts (2015) using confirmatory factor analysis suggests that the scale is best used as a single factor. In their study, they found a Cronbach’s alpha of .91. The scale consists of 16 items, each of which is responded to on a seven-point Likert-type type dimension, ranging from 1 (extremely dissatisfied) to 7 (extremely satisfied). An item example is ‘How dissatisfied or satisfied are you with your immediate boss’. A high average score indicates high satisfaction. The Cronbach’s alpha of this scale was found to be .940.
Mental well-being
This was measured using the Short Warwick-Edinburgh Mental Well-being Scale (Stewart-Brown, Tennant, Platt, Parkinson, & Weich, 2009). The authors report high structural validity and an internal consistency (using the Person Separation Index [PSI]) of .84. The scale consists of seven items, responded to on a five-point dimension, ranging from 1 (None of the time) to 5 (All of the time). A sample item is ‘I’ve been dealing with problems well’. A high average score indicates good psychological well-being. The Cronbach’s alpha of this scale was found to be .818.
Inclination to leave
The Propensity to Leave Scale, developed by Lyons (1971), was used to measure the nurses’ inclination to leave their jobs at the hospital. The scale consists of three items, responded to on five-point dimensions. Lyons (1971) found a Cronbach’s alpha of .87 for the scale. A high score indicates high propensity to leave. The Cronbach’s alpha in this study was found to be .848.
Social support
This was measured using the Revised Colleague and Supervisor Social Support Scale, which was adapted by Sham (2012) from the Workplace Social Support Scale developed by Caplan, Cobb, French, Van Harrison, and Pinneau (1980). The scale consists of 12 items, each responded to on a four-point dimension ranging from 1 (not at all) to 4 (very much). Six of the items measured social support from colleagues, and six measured social support from supervisors. Sample items include ‘How much can your colleagues be relied upon when things get tough at work?’ and ‘How much can your supervisor be relied upon when things get tough at work?’ The scale was used as full scale by Sham (2012), who found a Cronbach’s alpha of .94. In this study, the Cronbach’s alpha for the full scale was found to be .89.
None of these scales appear in published research from Zimbabwe. However, they have been used on diverse South African samples, including non-English first language speakers (c.f. Bernstein & Trimm, 2016; Sham, 2012).
Procedure
A quantitative, cross-sectional small-scale survey design was used. Permission to conduct this study was received from the medical superintendent of a public hospital in Zimbabwe. Information about the project was given to the nurses on paper, as well as in meetings at shift changes. The survey was presented as a paper questionnaire, which was distributed to the nurses by the researcher. The nurses were asked to complete this in their own time and place the completed questionnaire in a sealed box in the hospital canteen. Participation was voluntary, and the questionnaires did not require names. One hundred and two nurses chose to participate in the study.
The questionnaire measured job satisfaction, propensity to leave, and mental well-being (the outcome criterion variables); the amount of bullying experienced (the independent predictor variable); and social support from colleagues and supervisor (the moderating variable). The questionnaire was written in English, which is the language of education in Zimbabwe (Muchenje, Goronga, & Bondai, 2013).
Ethical considerations
The participants were assured of anonymity and confidentiality. Participation was voluntary, and there was no advantage or disadvantage to consenting or refusing to participate. A helpline for counselling services was provided in the event that the questionnaire elicited anxiety or problematic issues. The protocol for the study was given ethical clearance by the University of Witwatersrand Ethics Committee (Protocol Number MORG/14/010 IH).
Data analysis
The responses to the questionnaire were entered into a database, and analyses were conducted using IBM SPSS™ Version 24. The reliabilities of the scales were checked, and single scores representing each of the constructs measured were calculated by averaging the responses on the relevant items. If a participant failed to complete more than 25% of the items of a scale, their score was excluded from analyses. For less than 25% missing, mean replacement was used. Basic descriptive analyses were conducted including correlations, followed by multiple linear regression (MLR) analyses. The MLR analysis tested a simple moderated model, with a dependent variable (mental well-being, job satisfaction, or propensity to leave), a predictor (experience of bullying), and a moderator (social support from colleagues or social support from supervisors). These analyses were carried out using the PROCESS dialogue box in SPSS developed by Andrew Hayes (c.f. Field, 2014). The assumptions of the tests were checked prior to analysis. Assumptions checked included the normality of the residuals, outliers, and multicollinearity.
Results
Descriptive statistics
Using the criteria that skewness and kurtosis coefficients should be between −1 and +1 (Huck, 2009), the Job Satisfaction, Mental Well-being, Social Support, and Propensity to Leave scales could be taken as normally distributed. The Experience of Bullying scores were positively skewed, indicating that the bulk of the scores were at the lower end of the scale, with the skewness and kurtosis coefficients being higher than 1.00. A log transformation was conducted on experiences of bullying, which resulted in the coefficients meeting the normal distribution requirement.
The means and correlations between the variables are presented in Table 1. This table indicates that experience of bullying had a medium strength (statistically significant) negative correlation with job satisfaction, indicating the more bullying experienced, the lower the job satisfaction. It also had a medium positive, statistically significant correlation with propensity to leave, indicating that the more bullying experienced, the greater the propensity to leave. There was no zero-order correlation between bullying experiences and mental well-being.
Descriptive statistics of the scales.
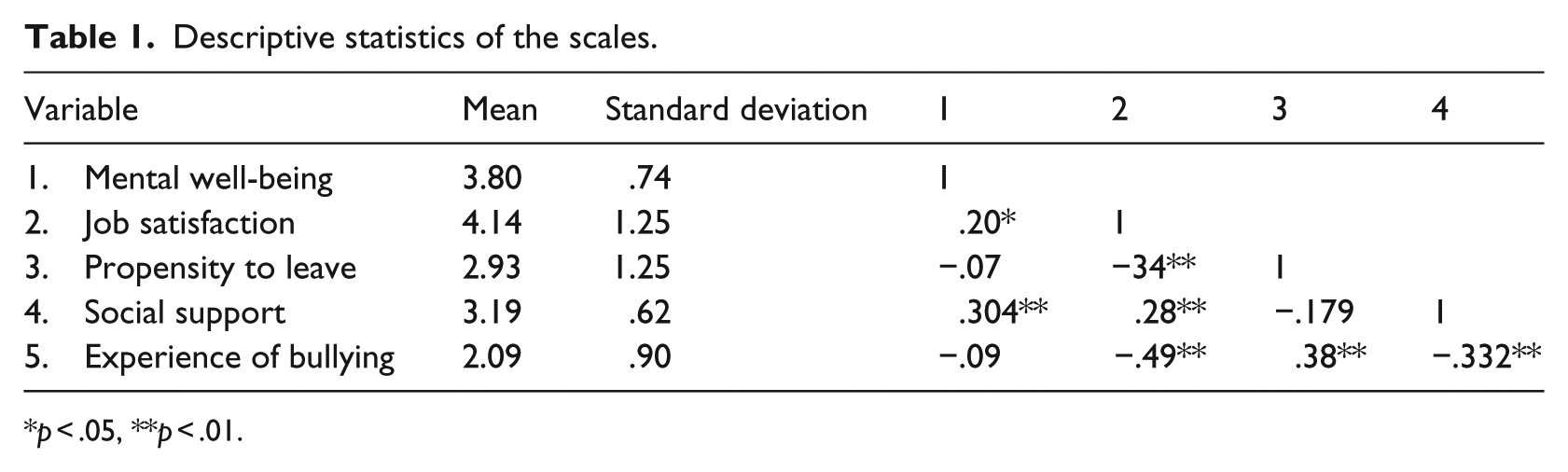
p < .05, **p < .01.
Social support had medium strength, statistically significant positive correlations with mental well-being and job satisfaction, indicating the more support perceived, the greater the level of mental well-being and job satisfaction. Among the predictors, social support had a medium strength, statistically significant negative correlation with experiences of bullying, indicating that the more bullying experienced, the lower the social support perceived.
Prevalence of bullying
To estimate the prevalence of bullying acts experienced, the averaged score over the 22 bullying acts was categorised into an ordinal scale where a mean of 1–1.5 was classified as ‘Never’, 1.6–2.5 as ‘Now and then’, 2.6–3.5 as ‘Monthly’, 3.6–4.5 as ‘Weekly’, and 4.6–5 as ‘Daily’. Table 2 provides the frequencies of nurses in each category.
Prevalence of bullying acts experienced.
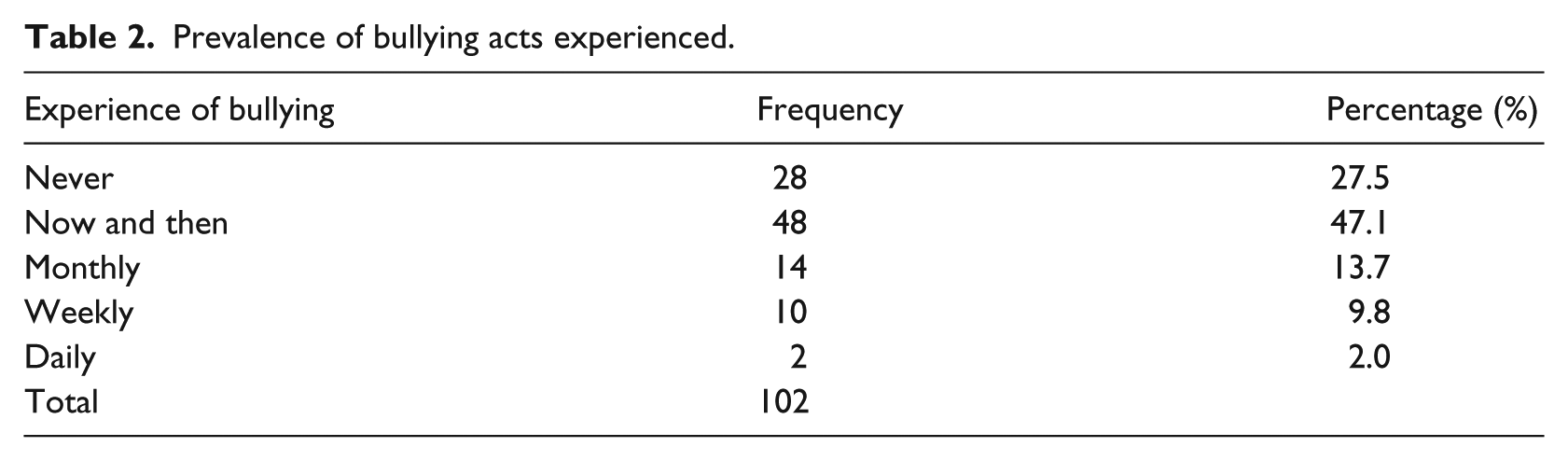
This analysis suggests that 72.5% of the sample had experienced bullying acts in the last 6 months, with 25.5% experiencing these on a regular basis (monthly to daily).
The participants’ mean scores on the 22-item negative acts scale was correlated with the question which asked explicitly whether they had been bullied at work. The correlation was of medium strength, r(102) = .465; p < .001. Thus, 22% of the variability of the bullying experiences was explained by the participants’ belief that they had been bullied. This supports the research which has argued that asking directly whether a person has been bullied does not provide as good an indication of his or her experiences as asking about acts (Einarsen, 2000).
The influence of social support on the consequences of bullying
To investigate whether social support subscales moderate the effect of bullying experiences on job satisfaction, mental well-being, and propensity to leave, three MLR analyses were conducted. Prior to running these tests, the assumptions of MLR were checked: normality of residuals, linearity, homoscedasticity, and multicollinearity. These were all satisfactory. The MLR analyses were conducted with the three outcome variables as the dependent variable and experience of bullying as the independent variable, with social support entered as a moderator.
Mental well-being
The full-moderated regression model was statistically significant, F(3, 92) = 4.88, p = .003, explaining R2 = 13.5% of the variability. The parameters of the linear model are presented in Table 3.
Linear model of predictors of mental well-being.
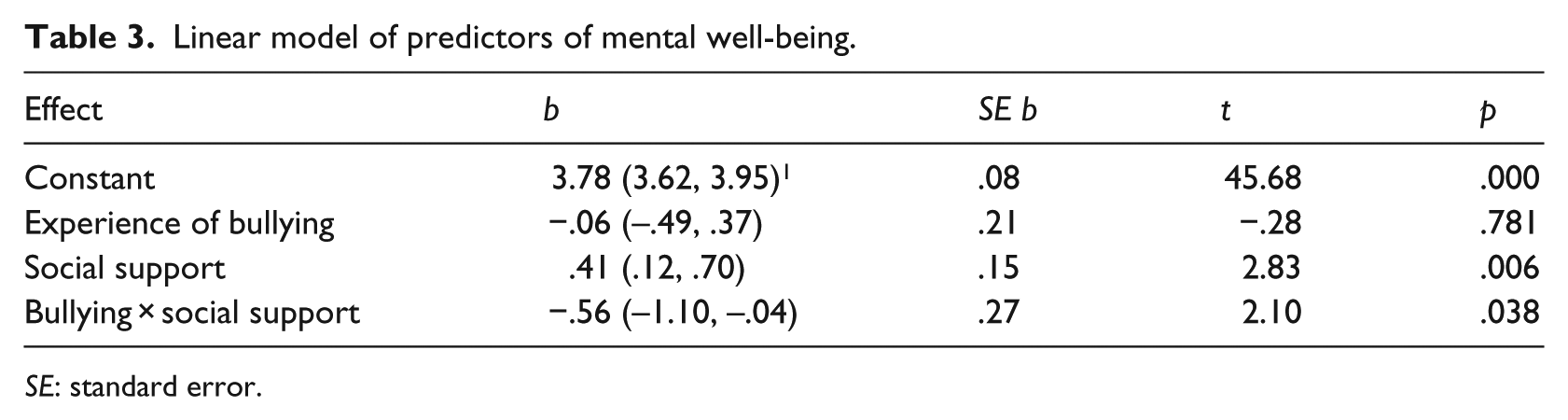
SE: standard error.
The interaction term was statistically significant, indicating that the effect of bullying on mental well-being varies over the different levels of social support. Figure 1 represents the manner in which the interaction operates:

Graph of the effect of bullying on mental well-being at different levels of social support.
For individuals with low or medium social support, the slopes of the lines are not statistically significant, indicating that mental well-being is not affected by the level of bullying experienced. However, for individuals with a high level of social support, the slope is significantly negative. At low levels of bullying, their mental well-being is higher than those with medium and low levels of social support. However, as the amount of bullying increases, the mental well-being of individuals with strong social support decreases so that at high levels of bullying, the effect of social support is negligible.
However, given the relatively low R2, it is clear that there are other factors that are important for understanding mental well-being among the nurses.
Job satisfaction
The full-moderated regression model was statistically significant, F(3, 92) = 10.84; p < .0001, explaining R2 = 26.8% of the variability. The parameters of the linear model are presented in Table 4.
Linear model of predictors of job satisfaction.
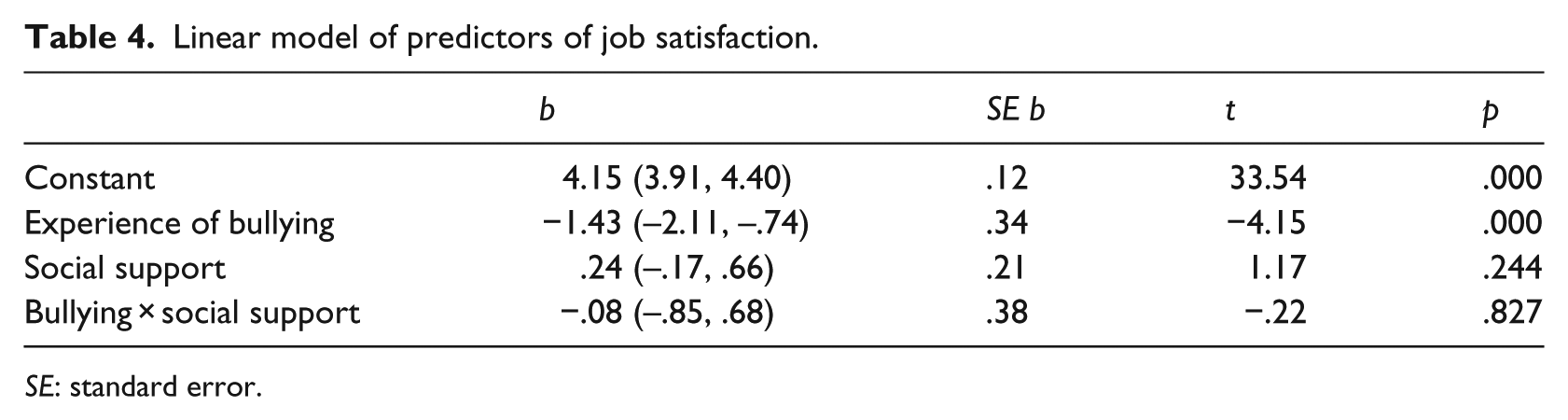
SE: standard error.
The experience of bullying was the only factor influencing job satisfaction, indicating that the higher the level of bullying experienced, the lower the job satisfaction of the nurses. The influence of social support did not reach significance and no interaction effect was present.
Propensity to leave
The full model was statistically significant, F(3, 92) = 7.00; p < .001, explaining 16.3% of the variation in propensity to leave. The parameters of the linear model are presented in Table 5.
Linear model of predictors of propensity to leave.
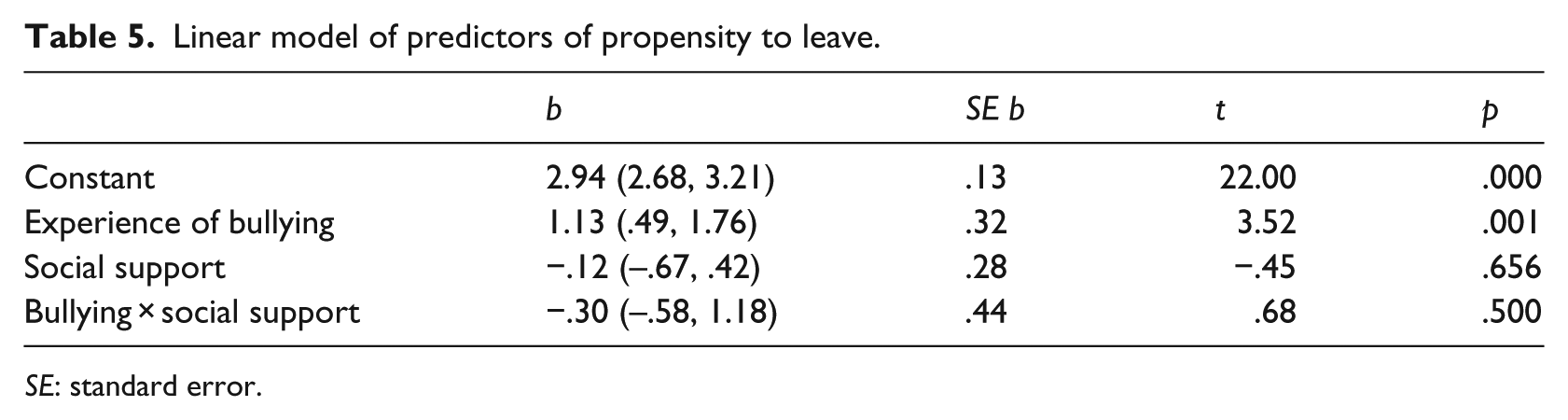
SE: standard error.
As with job satisfaction, only experience of bullying affected propensity to leave, indicating that the more nurses experienced bullying, the higher their propensity to leave their job. Social support did not influence this, and there were no interaction effects present.
Discussion
First, this study aimed to investigate the pervasiveness of bullying within the nursing sector. Considering the number and frequency of the bullying behaviours experienced, our findings suggest that a majority of nurses are affected, although only 25% indicated that this occurred often enough to be described as continuous.
Second, we investigated the effect of bullying on the specified outcomes – nurses’ mental well-being, job satisfaction, and intention to leave, and whether social support moderated the bullying–outcome relationship. Our analysis indicated that job satisfaction and propensity to leave were both strongly affected by the degree of bullying the nurses had experienced, but this was not moderated by social support. In the case of mental well-being, experiences of bullying were moderated by social support, indicating that at low and moderate levels of bullying, higher levels of social support led to greater mental well-being. However, at high levels of bullying, the amount of social support did not affect mental well-being.
Previous research has demonstrated that bullying erodes self-esteem and has deleterious organisational outcomes. For example, Nielsen and Einarsen (2012) in a meta-analyses of 66 independent studies (N = 77,721) indicated that WPB resulted in poor psychological well-being, as well as increased intention to leave, absenteeism, lowered job satisfaction and organisational commitment, and lowered job performance and productivity. The lack of direct or moderating effects evidenced for social support in the case of job satisfaction and propensity to leave was unexpected, although similar findings have appeared in the WPB–outcomes literature. We suggest that explanations for this centre around coping strategies.
A number of different types of coping strategies have been described. Coping strategies may be either active or passive (Ólafsson & Jóhannsdóttir, 2004). Seeking out and utilising social support (along with confronting the bully and asserting oneself) are considered to be an active coping strategy. Active strategies may be more effective and constructive than passive strategies such as doing nothing, avoiding the situation, and escaping the situation by resigning (Bernstein & Trimm, 2016). However, the effectiveness of active strategies rather than passive is, to some extent, contested. Some studies have indicated that active coping strategies of seeking help may fail to buffer the negative health effects of bullying (Hewett, Liefooghe, Visockaite, & Roongrerngsuke, 2016; Reknes et al., 2016). Furthermore, other studies have suggested that passive strategies seem to be the most commonly used in bullying situations as they are an easier option (Djurkovic, McCormack, & Casimir, 2005). Research has found that targets of bullying more often used avoidance behaviours (taking sick leave or quitting the job) and doing nothing (ignoring the problem or waiting in the hope that the negative behaviour will stop) (Ólafsson & Jóhannsdóttir, 2004; Zapf & Gross, 2001).
This more common choice of a passive strategy may be contingent on the degree of perceived control that the person has in the situation (Hogh & Dofradottir, 2001; Reknes et al., 2016). In situations where bullied individuals feel that they cannot control the stressor situation, they may prefer to do nothing as opposed to seeking out help or confronting the bully. Depending on the situation, active or passive strategies may be more or less effective in moderating the relationship between WPB and outcomes (Dewe, O’Driscoll, & Cooper, 2010). It is, thus, possible that nurses, although they perceive that they may have support resources available to them, do not enact them as they feel that calling for help will not be effective in changing the behaviour of the bullying perpetrator.
Furthermore, the lack of moderator effects may be a function of factors unique to the nursing environment, that is, the culture of bullying that is so pervasive within this sector. Research suggests that bullying behaviour within nursing has deep roots that go as far back as the training of student nurses from their first year onwards. In a study conducted by Englebracht, Heyns, and Coetzee (2017), it was shown that of 680 students under study, all had experienced severe bullying, mainly from registered nurses under whose supervision they had been working and training throughout the years of their degree. They note that bullying among nurses has deep roots in nursing education, with student nurses frequently being subjected to bullying and hazing behaviours during their training. Thus, by the time a student nurse qualifies, their exposure to bullying has been so prolonged that they may, to some extent, have become tolerant of and inured to such behaviour and may even have built up resilience in the face of such a stressor. This may, to some extent, explain the finding that at high levels of bullying, all levels of social support do not improve mental well-being.
Research has also indicated that one of the ways in which nursing students cope with bullying is by deflecting their victimisation onto others, that is, by becoming perpetrators themselves (Lewis, 2004; Woelfle & McCaffrey, 2007). Thus, a cycle of violence and intimidation between target and perpetrator, and target as perpetrator permeate throughout the profession, becoming part and parcel of cultural norms within the profession (Woelfle & McCaffrey, 2007).
Within an organisational culture, where there is a high degree of tolerance for bullying behaviour, the utilisation of social support may not be a viable option (Englebracht et al., 2017). In such an environment, bullying behaviour may become normative, and nurses must learn to deal with this targeting by simply accepting it or by deflecting their emotions onto others and by becoming bullying perpetrators themselves. Thus, the adoption of defensive and deflective strategies as opposed to seeking help through social support would be considered to be the more appropriate coping strategy. It is, thus, possible that nurses, although they perceive that they may have support resources do not enact them as the culture of the profession is one in which seeking of help is not encouraged (Colduvell, 2017).
Linked to this discouragement of seeking help within an organisational culture tolerant of bullying, for those who do use this mechanism, they may find that this leads to an undermining of their self-esteem, sense of agency, and autonomy. In an environment where you need to ‘hang tough’, drawing on social support may worsen the situation by ‘drawing attention’ to the individual’s problem (Aoyama, Yanagida, & Wright, 2017; Seidman, Shrout, & Bolger, 2006; Shrout, Herman, & Bolger, 2006). The perception that one needs support to deal with the problem may leave the individual feeling incompetent and devalued and therefore inhibit them from seeking out social support in times of stress (Shrout et al., 2006). Consequently, for some individuals, social support will be too costly to use (Seidman et al., 2006; Shrout et al., 2006). In such a situation, those who are unable to cope by defensive deflecting may feel that the only alternative may be to resign from their current position or to leave the profession.
There are also some suggestions that an individual’s culture may also play a role in terms of whether social support is utilised or not (Taylor, Welch, Kim, & Sherman, 2007). Taylor and colleagues noted that in ‘collectivist cultures a person is expected to avoid bringing their personal problems to attention of others because such an act can undermine harmony or make inappropriate demands on the social group’ (p. 832). They also distinguish between implicit and explicit support, with implicit support being a form of ‘emotional comfort’ that one can obtain without disclosing one’s personal problems, while explicit support refers to that which is actively sought out and utilised. While this research was carried out comparing Asians to American Caucasians, the same distinctions may hold for African culture. To the authors’ knowledge, no research comparing ethnic groupings on cultural perceptions of social support has been done within the African context. It may be possible that the predominantly Black African Zimbabwean sample in this study was reluctant to activate explicit support for personal cultural reasons.
Finally, another inhibitor to actually enacting social support may pertain to norms of reciprocity. This refers to the fact that those who receive support are expected to also provide support to those in their support network. Thus, recipients of support receive both benefits and costs which may be incurred concurrently (Seidman et al., 2006; Shrout et al., 2006). Costs of reciprocity may reduce the probability that one will ask for help, particularly in times of stress when one is already overburdened. The knowledge that one will have to repay later may be overtaxing for the person currently under duress.
Limitations of this study are, first, that a small number of the nurses responded to the questionnaire. This could be due to their being overwhelmed with work, or to fears that supervisors or hospital management might see the questionnaires. Second, the data were collected utilising self-report measures, which embody a number of possible biases, such as social desirability (prestige) bias and common variance bias (Siemsen, Roth, & Oliveria, 2010).
Conclusion
This research on nurses in a Zimbabwean hospital found that the amount of bullying they experienced influenced their job satisfaction and propensity to leave. Social support only improved mental well-being at lower levels of bullying. The finding that social support did not influence job satisfaction or propensity to leave may speak to the unique environment of nursing, which is particularly tolerant of bullying. Future research should therefore examine environmental factors within the health care sector that allow bullying to flourish. This may inform interventions aimed at changing this organisational culture. This is vital if one is to stem the tide of nurses leaving the profession, which, in turn, places enormous strain on those nurses who choose to remain.