
Abstract
Globally, childhood sexual abuse is a public health problem that affects millions of people. Few studies have considered its long-term ramifications, especially among young adults in developing countries. This study assessed the influence of childhood sexual abuse on depression and behaviours in young adults. Data were obtained from 362 students enrolled at a university in Botswana (Age: M = 21.40, standard deviation = 2.48) using the Childhood Sexual Abuse Scale, the 21-item Beck’s Depression Inventory–II, Revised Sociosexual Orientation Inventory, and Alcohol Use Disorders Identification Test (AUDIT). The t test and chi-square test of independence were used to assess subgroup differences and regression analyses were used to assess the extent to which childhood sexual abuse predicted depression and risky behaviours. About 25% (n = 90) reported childhood sexual abuse, 18% reported harmful alcohol use (n = 66, 18.2%), 7.82% (n = 28) reported severe depression, and 24% (n = 101) reported failure to use contraceptives. Childhood sexual abuse significantly predicted depression and all the behavioural outcomes in the study. The effect sizes of the associations between childhood sexual abuse on the one hand and mental health and behavioural outcomes on the other were modest. Consequently, the current study is a precursor to further studies on the long-term outcomes of childhood sexual abuse in Botswana. Consequently, a history of childhood sexual abuse should be considered in planning interventions to mitigate depression and behavioural problems on university campuses.
Globally, childhood sexual abuse (CSA) is a significant public health issue that affects millions of people (Veenema, Thornton, & Corley, 2015). Survivors of CSA suffer not only from physical health problems such as chronic pelvic pain (Daigneault, Vézina-Gagnon, Bourgeois, Esposito, & Hébert, 2017) but also from mental health problems such as depression, anxiety, and post-traumatic stress disorder (PTSD) (Papalia, Luebbers, Ogloff, Cutajar, & Mullen, 2017; Seloilwe & Thupayagale-Tshweneagae, 2009); substance abuse (Berg, Hobkirk, Joska, & Meade, 2017); and problems with sexual functioning later in life (Meyer, Cohn, Robinson, Muse, & Hughes, 2017). Although the consequences of CSA have been widely studied in Western countries, such studies are scarce in low- and middle-income countries, including Botswana (Mathoma, Maripe-Perera, Khumalo, Mbayi, & Seloilwe, 2006). Many studies on CSA in low- and middle-income countries have been conducted in the context of war (Amone-P’Olak, et al., 2016; Amone-P’Olak, Ovuga, & Jones, 2015).
Both men and women experience sexual abuse before the age of 18. For example, in South Africa, 17.7% of males and 18.3% of females are reported to have experienced forced or coerced sex before the age of 16 (Andersson et al., 2012). Although more females report sexual abuse than males, CSA is said to have similar behavioural outcomes for both males and females (Abajobir, Kisely, Maravilla, Williams, & Najman, 2017). While CSA impacts sexual self-esteem similarly for both genders, females end up being victims of further sexual violence while males end up being perpetrators of sexual abuse (Whitfield, Anda, Dube, & Felitti, 2003). Furthermore, variations by gender may be based on factors such as a stressful family environment or the severity of the sexual abuse (Krahé & Berger, 2017).
In Botswana, empirical studies documenting the prevalence of CSA are rare. A survey of sexual violence in Botswana and Swaziland estimated sexual abuse of women at 10.3% (Tsai et al., 2011). Another study highlighted violence against children in general (Jankey & Maundeni, 2018) and mental health consequences of sexual abuse among adolescent girls in particular (Morna, 2012; Seloilwe & Thupayagale-Tshweneagae, 2009). Furthermore, social factors such as the high prevalence of HIV/AIDS (Lawler et al., 2011), domestic violence (Jankey & Maundeni, 2018; Morna, 2012), multiple concurrent sexual partners (Merrigan et al., 2015; Selepe, Ngwenya, Albers, & Jankey, 2017), and family dysfunction, all common in Botswana, may provide the context in which CSA thrives. In addition, a large number of orphans resulting from the HIV/AIDS pandemic are living with relatives or on their own (Jankey & Maundeni, 2018; Seloilwe & Thupayagale-Tshweneagae, 2009), and the high rate of intergenerational sex (Schaefer et al., 2017) may predispose children to the risk of CSA. Besides, the traditional belief that older men would revitalise their sexual life by having sexual intercourse with young girls (Santow, Bracher, & Watkins, 2017) and sex for monetary gain or material support (Varma, Gillespie, McCracken, & Greenbaum, 2015) are common in Botswana and may expose children, especially young girls, to the risk of CSA. In Botswana, 7 out of 10 children are reportedly living in families with a single parent, usually the mother (Dintwat, 2010). Moreover, women, particularly female-headed households, suffer disproportionately from poverty with 46% of them compared to 27% of male-headed households living in poverty (Dintwat, 2010). Young and poor women with children may resort to transactional sex to get additional income to look after their children (Selepe et al., 2017). Consequently, young children, especially girls, are raised in a sexually permissive environment that may put them at further risk of abuse. Thus, contextual factors exist that may expose children to CSA.
Previous studies suggest that CSA is common and occurs in a family environment with a high density of conflicts, family volatility, parental psychopathology, and drug and substance use (Fergusson, Horwood, & Lynskey, 1997). Moreover, CSA is linked to adverse later mental health outcomes and risky sexual behaviours (Fergusson et al., 1997; Hillberg, Hamilton-Giachritsis, & Dixon, 2011). Such mental health consequences include depression, anxiety, and PTSD (Papalia et al., 2017; Seloilwe & Thupayagale-Tshweneagae, 2009). Similarly, CSA has been associated with later risky sexual behaviours that include increased rates of sexual activity and unsafe sexual practices such as failure to use contraceptives, having multiple concurrent sexual partners, and early sexual debut (Fergusson et al., 1997). These risky sexual behaviours may also put victims of CSA at an increased risk of victimisation later in life (Hannan, Orcutt, Miron, & Thompson, 2017).
The majority of studies draw their samples from minority or disadvantaged backgrounds without considering the possibility that CSA may affect people from all walks of life including students enrolled in colleges and universities. In this study, the sample was drawn from a population of university students in Botswana. The current study will focus on depressive symptoms, alcohol use, and sexual behaviours, all common phenomena among young adults. Regarding sexual behaviours, the study will specifically examine uncommitted sexual relations, contraceptive use, and early sexual debut. Identifying victims of CSA is vital for developing interventions to mitigate the negative consequences of CSA.
Theoretical and conceptual framework
This study will be embedded within the framework of the Four Traumagenic Dynamics Model (4TDM) postulated by Finkelhor and Browne (1988). In this model, four dynamics – traumatic sexualisation, stigmatisation, betrayal, and powerlessness – are used as a framework to explain the process and consequences of CSA (Figure 1). Traumatic sexualisation refers to the facilitative and formative factors that affect victim’s sexual thoughts, feelings, and behaviour leading to dysfunctional sexual development often associated with distorted sexual self-concept, confusion and misconception around sex norms, and a preoccupation with sex and sexual dysfunction (Finkelhor & Browne, 1988). A feeling of betrayal is engendered when the abuser holds a position of trust and on whom the victim depends. Betrayal shatters the victim’s faith and trust and may be associated with depression, lack of trust, and vulnerability to subsequent abuse and dysfunctional sexual relations (Pulverman & Meston, 2016). Moreover, close relatives or caregivers may blame CSA victims for enticing the abuser or bringing it upon themselves by behaving or dressing inappropriately, all of which may lead to stigmatisation (Finkelhor & Browne, 1988). Consequently, the victim may feel worthless, shameful, and guilty, and may resort to risky behaviours such as drug and substance abuse or having multiple concurrent sexual partners (Selepe et al., 2017). Finally, CSA diminishes the victim’s sense of self-efficacy and determination as their bodies have been violated against their will, thus producing a sense of powerlessness (Finkelhor & Browne, 1988).
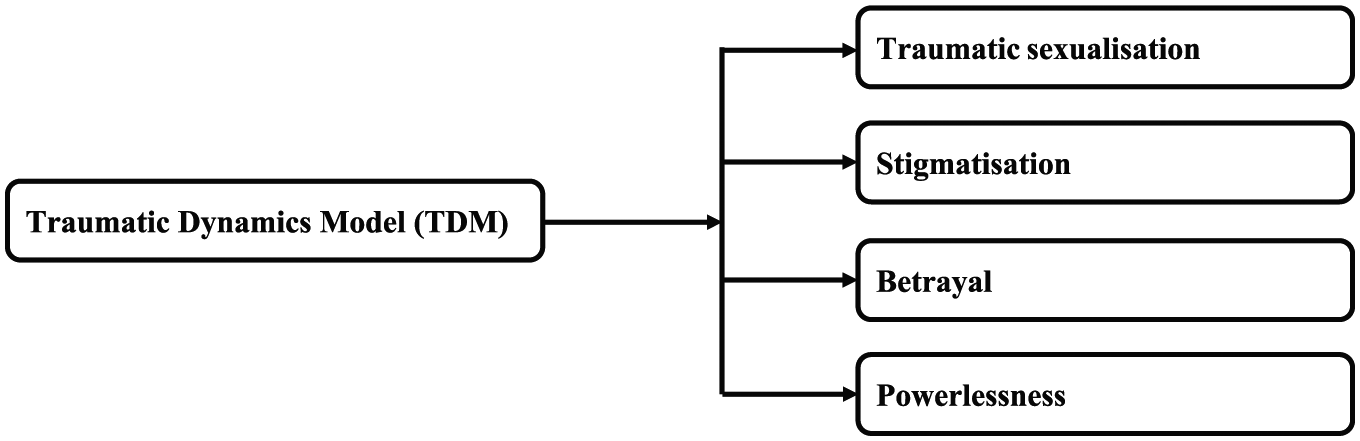
Traumatic Dynamics Model (TDM).
The current study aims to assess the influence of CSA on survivors in a sample of young adults. The specific objectives of the study were to (a) assess the prevalence of CSA, depression, and risky behaviours among young adults enrolled at a university in Botswana; (b) investigate gender differences in reporting CSA, risky behaviours, and depression; (c) assess the differences in reporting risky behaviours and depression in young adults with and without a history of self-reported CSA; and (d) assess the extent to which CSA predicts depression and risky behaviours. Based on the literature, it is hypothesised that self-reported CSA is associated with increased symptoms of depression and risky behaviours.
Method
Participants
A cross-sectional survey design was used in the current study. Participants were randomly drawn from a population of young adults pursuing various courses at a university in Botswana. Students in various years of study from all the faculties of the university were invited to participate in the study.
Instruments
The following instruments were used to collect the data:
Sociodemographic characteristics
The sociodemographic characteristics assessed were age, sex, year of study, and the educational levels of parents or guardians. Participants were also asked to indicate at what age they had their first sexual intercourse: ‘before 10’ (=1), ‘between 10 and 12’ (=2), ‘between 13 and 15’ (=3), ‘between 16 and 17’ (=4), and ‘above 18’ (=5). On contraceptive use, participants were asked to respond to how the following statement was true of them: ‘I normally engage in sexual intercourse without using contraceptives’. The response categories were ‘not at all true of me’ (=1), ‘slightly true of me’ (=2), ‘somewhat true of me’ (=3), and ‘mostly true of me’ (=4).
Revised Sociosexual Orientation Inventory
The number of sexual partners and uncommitted sex was assessed using the Sociosexual Behaviour subscale of the Revised Sociosexual Orientation Inventory (SOI-R), initially developed by Simpson and Gangestad (1991) and amended by Penke and Asendorpf (2008). The subscale consisted of three items (e.g., ‘How many different partners have you had sex within the past 12 months?’). The subscale is coded as 1 (0), 2 (1), 3 (2–3), 4 (4–7), and 5 (8 or more) with a higher score indicating more uncommitted sexual behaviours. The internal consistency of the subscale in the current study was Cronbach’s alpha = .91.
Symptoms of depression
Symptoms of depression were assessed using the 21-item Beck Depression Inventory–II (BDI-II; Beck, Steer, & Brown, 1996) rated on a 4-point scale ranging from 0 to 3 based on the severity of each item. The scores are categorised as follows: 0–13 (minimal depression), 14–19 (mild depression), 20–28 (moderate depression), and 29–63 (severe depression). Items on the BDI-II include ‘sadness’ (e.g., ‘I am so sad and unhappy that I can’t stand it’), ‘pessimism’ (e.g., ‘I feel I have nothing to look forward to’), and so on. The BDI-II is widely used with sound psychometric properties and correlates well with other measures of depression (Beck et al., 1996). In studies with similar samples in Botswana, the internal consistency reliability of the BDI-II ranged from .89 to .95 (Hetolang & Amone-P’Olak, 2017; Korb & Plattner, 2014).
CSA scale
The CSA scale is a self-report measure developed by Aalsma, Zimet, Fortenberry, Blythe, and Orr (2002) to assess the occurrence of CSA in child and adult samples. It consists of four items binary-coded as ‘0’ for non-occurrence and ‘1’ for an occurrence. In previous studies, the CSA scale demonstrated excellent internal reliability of .81. In this study, the reliability was acceptable at Cronbach’s alpha = .85. The total score is obtained by summing up the scores of the four items with a score of ‘1’ and above indicating sexual abuse. The items include ‘being touched in a sexual way against one’s will’, ‘being made to touch someone in a sexual way against one’s will’, ‘believing that you have been sexually abused’, and ‘being threatened by someone that they will tell lies or hurt you unless you did something sexual with them’. Internal consistency of .89 was achieved for this study.
Alcohol problems
Alcohol problems were assessed using the Alcohol Use Disorders Identification Test (AUDIT; Saunders, Aasland, Babor, de la Fuente, & Grant, 1993). The 10-item AUDIT is a screening instrument for excessive alcohol use in primary health care. Each item is scored 0 to 4, with total scores ranging from 0 to 40. Scores of 8 and above are generally considered indicative of hazardous or harmful alcohol use as well as possible alcohol dependence (Babor, Higgins-Biddle, Saunders, & Monteiro, 2001).
Procedure
Participants completed the questionnaire anonymously in different lecture rooms in the various faculties. The research assistants obtained permission from Faculty Administrators and lecturers to collect data from the respective lecture rooms in the eight faculties of a university in Botswana. Participants included students registered at all levels of study (i.e., Year 1 till Year 5). Participants took between 10 and 15 min to fill in the questionnaire in the presence of a research assistant, who was on standby in the classroom to answer any query that the students could have. Altogether, 352 students (65% female; n = 229) with an average age of 21.37 (standard deviation [SD] = 2.41, minimum 18 and maximum of 25).
Ethical considerations
The Research Ethics Committee of University of Botswana approved the study. Participants signed informed consent after the purpose of the study was explained to them. Participants were assured of confidentiality and that their responses would be treated anonymously and were asked not to write anything on the questionnaire that would identify them. The debriefing was carried out after data collection, and information on support services within and outside the university were provided for those who may require psychological support. The contact numbers for the Psychology Clinic and Counselling Centre, both within the University of Botswana campus, were provided.
Data analyses
Descriptive statistics were used to compute sociodemographic characteristics and prevalence of self-reported CSA, symptoms of depression, risky behaviours, and age at first sexual intercourse. The t test and chi-square test of independence were used to assess subpopulation differences. Univariable regression analysis was used to assess the extent to which CSA predicted symptoms of depression and the risky behaviours outlined above. Given the gender differences regarding some of the outcome variables such as alcohol use and depressive symptoms, gender was adjusted for in all the analyses. The effect sizes of the associations between self-reported CSA on depression and all the risky behaviours were computed using eta-squared (η2). Also, the effect sizes of the gender differences on CSA, depression, and risky behaviours were calculated using phi (φ) coefficients. Statistical analyses were conducted using IBM SPSS statistical software, version 24.0 (IBM Corp., 2015). The p values of less than .05 were considered statistically significant.
Results
Sociodemographic characteristics and prevalence of CSA, depression, and risky behaviours
Sociodemographic characteristics of study participants are presented in Table 1. Altogether, 362 students participated in the study, 229 (65%) of whom were female students. On average, participants were aged 21 (SD = 2.41, minimum 18 and maximum 25). The prevalence rate of CSA, depression, and other risky behaviours is presented in Table 1. Overall, 24.9% (n = 90) of the participants reported CSA, 7.8% reported severe depressive symptoms, 26.2% (n = 95) reported having sexual intercourse before 18 years of age, 18.2% (n = 66) reported hazardous use of alcohol, and 43% (n = 101) reported that they were sexually active (n = 235) and used contraceptives intermittently or not at all. There were no gender differences on age at first sexual intercourse, contraceptive use, and depression. However, uncommitted sexual behaviours and alcohol use yielded gender differences, with the male gender, on average, scoring higher than their female counterparts.
Sociodemographic characteristics of the study variable stratified by gender.

SD: standard deviation; Cohen’s d: a measure of effect size; CSA: childhood sexual abuse; significant values are highlighted in
Differences in reporting depression and risky behaviours among those who did and did not report CSA
Participants who reported CSA scored significantly higher on depression and risky behaviours than those who did not report CSA (Table 2). The effect sizes of the differences ranged from small (depression, φ = .17) to moderate (uncommitted sexual behaviours, φ = .32).
Risky behaviours and depression stratified by self-reported CSA.
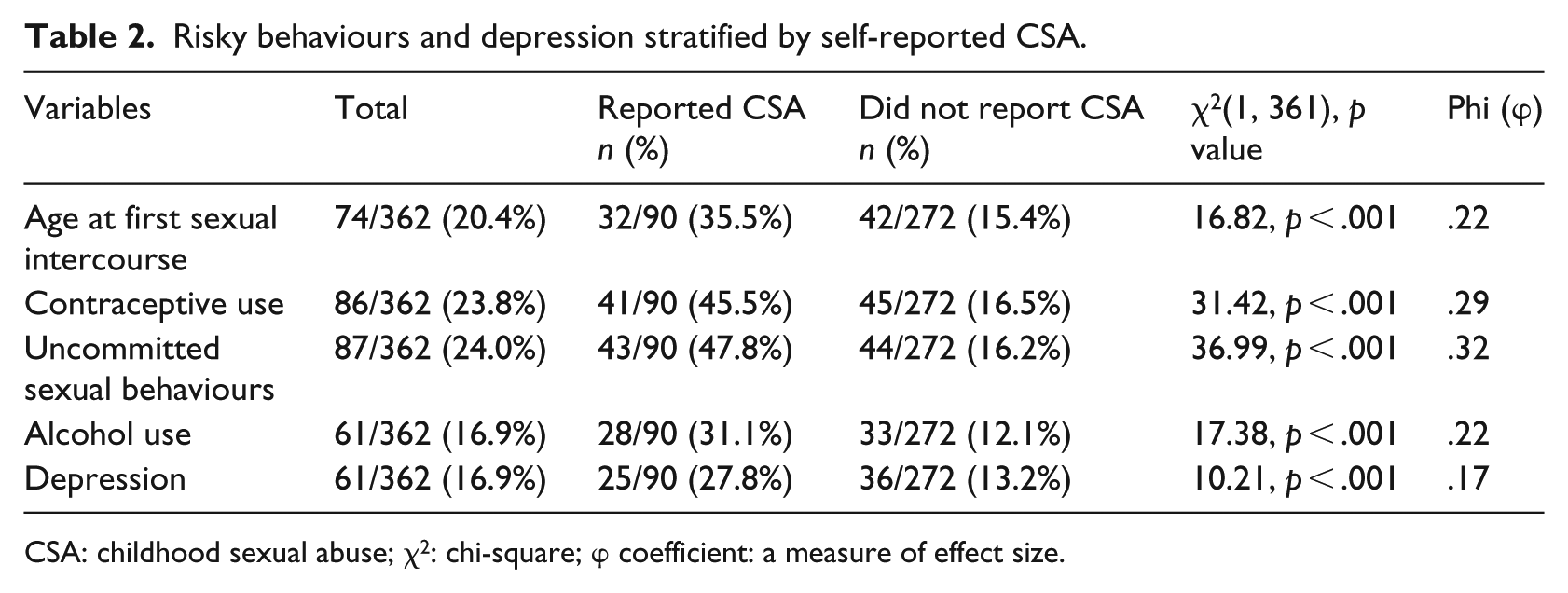
CSA: childhood sexual abuse; χ2: chi-square; φ coefficient: a measure of effect size.
The associations of CSA with depression and risky behaviours
Overall, self-reported CSA significantly predicted depression and all the risky behaviours (based on a continuous scale) in univariable regression models (Table 3). The regression coefficients ranged from β = .18, 95% confidence interval [CI] = [.02, .24] for age at first sexual intercourse to β = .26, 95% CI = [.04, .46] for symptoms of depression (Table 3). Each regression coefficient represents the number of SD change in the dependent variable per SD change in the independent variable. For example, the regression of alcohol on self-reported CSA indicates that a change of 1 SD is associated with a 0.21 SD change in depression. The effect sizes of the associations ranged between η2 = .03 for age at first sexual intercourse and η2 = .07 for depressive symptoms.
Univariable regression analyses of CSA on risky behaviours adjusted for gender.
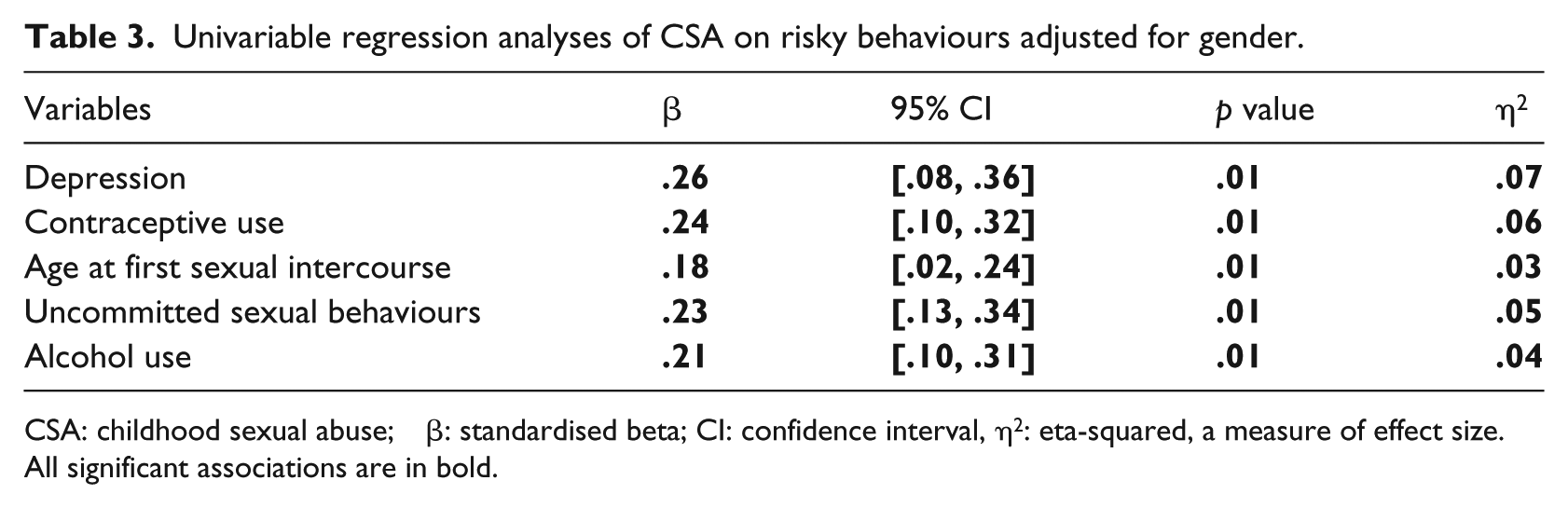
CSA: childhood sexual abuse; β: standardised beta; CI: confidence interval, η2: eta-squared, a measure of effect size.
All significant associations are in bold.
Discussion
The current study assessed the influence of self-reported CSA on depression and risky behaviours in young adults at a university in Botswana. Almost 25% reported CSA, which, in turn, was associated with more symptoms of depression and risky behaviours. The findings of this study are consistent with previous findings suggesting that CSA predicted depression and risky behaviours (Berg et al., 2017; Daigneault et al., 2017; Seloilwe & Thupayagale-Tshweneagae, 2009). Past studies have indicated that a history of CSA was linked to PTSD, which, in turn, was associated with alcohol abuse to control emotional experiences (Hannan et al., 2017). Although the effect sizes of the associations in this study ranged from low to moderate, the differences between participants who experienced CSA and those who did not were all significant. The small effect sizes can be explained in the context of two important environmental factors: family environment and traditional beliefs and practices.
Although neglected in research, a confluence of family environmental factors such as conflicts, poverty, domestic violence, and alcohol and drug abuse are known to be related to child maltreatment in general (Seehuus, Clifton, & Rellini, 2015). In Botswana, family dysfunction is common with 7 out of 10 children coming from homes with only one parent, mostly single mothers, and only 18% of couples are married (Government of Botswana and United Nations, 2010). Besides the family situation in Botswana, domestic violence and alcohol and drug abuse are rampant and often expose children to risky behaviours early in life (Phorano, Nthomang, & Ntseane, 2005). Besides, the traditional belief that young girls are free from sexually transmitted diseases (e.g., HIV/AIDS) may be associated with CSA (Santow et al., 2017, p. 17). Moreover, intergeneration sex for monetary gain and material support, all common in Botswana, provide an enabling context for CSA to thrive (Schaefer et al., 2017). Consequently, it could be that CSA often thrives in a context of both low-income family environment and deep-rooted negative traditional beliefs. Therefore, a dysfunctional family environment such as domestic violence, drug and substance abuse (Kgatitswe & Amone-P’Olak, 2017; Ludick & Amone-P’Olak, 2016; Moitlakgola & Amone-P’Olak, 2015), and traditional beliefs and practices could be mediators of CSA (Seehuus et al., 2015).
The present study has several limitations. First, the cross-sectional design makes it impossible to conclude that the symptoms of depression or risky behaviours are a result of CSA. Second, the sample size was small and uncharacteristic of young adults in Botswana. Third, the role of other factors such as adverse family environment (conflicts, poverty, instability, drug and substance abuse, etc.) and personality on depression and the risky behaviours were not considered in this study. Consequently, the symptoms of depression and risky behaviours might be a result of other factors. Fourth, the strengths of the associations were weak as indicated by the low to moderate effect sizes. Subsequently, interventions to reduce the harmful effects of CSA on depression and behavioural risks may be minimal. Fifth, the results of the current study are restricted to the indicators of CSA used in this study. The CSA measure used in the study does not assess other forms of sexual abuse such as rape, exposure to pornography, and exposure to or engaging in other sexual activities. Finally, the subject of sexual abuse is sensitive and traumatic. The majority of victims often shy away from talking about it. This might have limited reporting the incidents of CSA and some outcomes. Therefore, to disentangle the influence of CSA on long-term mental health and behavioural risks, a longitudinal study that takes cognisance of family and community environmental factors is recommended.
Nevertheless, the findings of the current study contributed to the literature in mainly two ways. First, few studies have been conducted on CSA in Botswana in general and among university students in particular. Although the students were from diverse backgrounds, the findings of the study are indicative of the extent to which CSA is rampant and an essential public health issue. Second, our study is the first to assess the associations between CSA in a population of young adults in Botswana, especially among students in a university. Consequently, the findings may help to put the issue of CSA on the agenda not only in institutions of higher learning but nationally as well.
Conclusion
CSA is very prevalent and often associated with vulnerability to depression and risky behaviours later in life. Early interventions should invariably include education of children to report sexual violence and to seek care after sexual abuse. For example, interventions may include promoting self-efficacy and competence to help children become less vulnerable to CSA and to disclose abuse when it occurs. At the university level, identifying participants with a history of CSA and mental health and behavioural risk reduction should be prioritised by policymakers and university administrators. For example, students can be informed of available services and encouraged to seek treatment for sexual abuse. As victims of CSA are vulnerable to re-victimisation, better education to facilitate disclosure, teaching victims appropriate CSA protective behaviours, and treatment are recommended.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and publication of this article.