
Abstract
The burgeoning increase in Internet access and use in South Africa and globally has opened a new doorway for provision of mental health services online. This descriptive study focuses specifically on psychotherapeutic services provided by South African psychologists. Draft guidelines for online therapy were developed and a sample of South African registered psychologists was asked to review, rate, and comment on the draft guidelines via an online survey. The sample also identified key ethical dilemmas arising from the novel use of this modality in South Africa. The draft guidelines were positively appraised by the majority of participants supporting the value of such guidelines in South Africa. Key ethical dilemmas identified included confidentiality, competence, boundaries, technological limitations, emergency situations, nature of therapeutic process, security of records, payment, and verification of identity.
As the world evolves and technological innovation increasingly drives development, Internet use has proliferated over the past two decades (Luxton, Nelson, & Maheu, 2016). Mental health services, including psychological interventions, have been greatly impacted by the increased access to and use of the Internet (Barnett & Scheetz, 2003; Clay, 2017; Evans, 2018; Fisher & Fried, 2003; Young, 2005). Provision of online mental health services, also called telepsychology, is increasing. Future clients may choose online counselling for all or part of their health care (Oravec, 2000), as is reflected in increasing applications of telemedicine (Mars, 2013). The provision of online therapy has many advantages, accommodating individuals who cannot or will not access direct face-to-face psychological services (Clay, 2017; Luxton et al., 2016) due to constraints such as geographic location, medical conditions, financial restraints, or other barriers (American Psychological Association [APA], 2013). A growing body of research suggests that in some cases online therapy is as effective as traditional forms of therapy (APA, 2013; Barak, Hen, Boniel-Nissim, & Shapira, 2008).
There has, however, been insufficient research done on the phenomenon of online therapy (Suler, 2005, in Hanley, 2009). Ethics authorities in developing countries lag behind in developing guidelines for online therapy (Hilgart, Thorndike, Pardo, & Ritterband, 2012). Consequently, there is considerable potential risk for both psychologists and their clients due to a lack of clearly defined best practices in existing ethics guidelines (Ohio Psychological Association [OPA], 2009; Palomares, Bufka, & Baker, 2016).
Some of the reported ethics-related issues common in telepsychology include confidentiality, competence, privacy, informed consent, crisis intervention, identity verification, online assessment, and appropriateness of online therapy (Clay, 2017; Hilgart et al., 2012; Luxton et al., 2016; Palomares et al., 2016). Availability of ethics guidelines for online therapy, supplementing existing ethics guidelines, may help to alleviate some of these ethical issues (London, 2010) and assist South African psychologists to practice online therapy ethically.
The existing South African ethical code for psychologists (Health Professions Council of South Africa [HPCSA], 2011) does not explicitly address online therapy (Evans, 2018), which is consistent with comments that ethics guidelines in general lag behind developments in practice (Hilgart et al., 2012; Wassenaar & Mamotte, 2012). In this research, the investigators aimed to develop draft ethics guidelines for online therapy in South Africa and surveyed a sample of registered South African psychologists regarding their perception of the draft guidelines, and explored their concerns about online service provision. Key ethical dilemmas in online therapy and suggestions to improve the draft guidelines were descriptively analysed and discussed.
It is hoped that this study may prompt more research on online therapy in South Africa and be of interest to the Professional Board for Psychology of the HPCSA.
The first part of this study involved the review of existing ethics guidelines to develop a new set of draft ethics guidelines specifically for online therapy in South Africa. A widely used biomedical ethics frame of reference (Beauchamp & Childress, 2013) was used to categorise the ethics dimensions.
The following ethics codes and guidelines were reviewed:
American Psychological Association, Ethical Principles of Psychologists and Code of Conduct (APA, 2016)
Australian Psychological Society, Code of Ethics (APS, 2007)
British Psychological Society, Code of Ethics and Conduct (BPS, 2009)
Canadian Psychological Society, Canadian Code of Ethics for Psychologists, 3rd ed. (CPA, 2000)
New Zealand Psychological Society, Code of Ethics for Psychologists Working in Aotearoa/New Zealand (NZPS, 2012)
Health Professions Council of South Africa, Act 56 of 1974, Annexure 12 (HPCSA, 2011)
Ohio Psychological Association, Telepsychology Guidelines (OPA, 2009)
These codes and guidelines (hereafter simply referred to as guidelines) were chosen as they were influential in the development of the current South African psychologists’ ethics code (Cooper, 2012; Wassenaar, 1998). These international guidelines were coded using a ‘top-down’ approach, with the initial theme codes adapted from Hilgart et al. (2012).
Ethics guidelines from New Zealand, Ohio, and Australia were further coded for text relating to recommended online therapy practices (APA, 2013). A table identifying the practices covered in the different guidelines was adapted and modified from the Ohio Telepsychology guidelines of 2008. Following the analysis of these ethics codes and guidelines, the Draft Ethics guidelines for psychologists with special reference to Online Therapy were developed (Appendix 1).
The second part of this study surveyed a sample of registered psychologists in South Africa who were also members of the Psychological Society of South Africa (PsySSA), soliciting their opinions on the proposed ethics guidelines developed in the first part of this study.
Method
Participants
A purposive sampling method was used in this study. Only registered psychologists in South Africa who were members of PsySSA were selected due to the availability of a PsySSA mailing list. All 1310 registered psychologists from this list were invited to participate via e-mail and were sent later reminders. The response rate was 3% (N = 38).
Instruments
The survey questionnaire comprised 10 forced-choice and open-ended questions. The open-ended items allowed for a more in-depth expression of participants’ opinions on the proposed guidelines. Some examples of open-ended questions include the following: ‘Question 6: What are the key ethical issues in online therapy?’ and ‘Question 8: If yes to Q7 (Do you think any points need to be added, developed more in the draft guideline?), describe and give reasons’.
Procedure
The online survey questionnaire was accessible to participants as an embedded link in the e-mail. The survey was created using the online form builder ‘Jotform Builder’. Respondents were requested to review the content and structure of the draft guidelines (Appendix 1), provide their feedback, and rate the code as useful or not useful. Respondents were also asked to identify key ethical dilemmas in online therapy.
Ethical considerations
Strict adherence to confidentiality and anonymity were maintained. Ethics clearance was obtained from the University of KwaZulu-Natal Humanities and Social Sciences Research Ethics Committee (Refs. HSS/0471/013M).
Data analysis
Descriptive statistics for the forced-choice question data were analysed using Statistical Package for Social Sciences (SPSS). Qualitative content analysis was done to aid in deductively analysing data obtained from the open-ended questions using codes adapted from Hilgart et al. (2012). The responses were coded into different themes and key ethical issues (Hilgart et al., 2012). Actual word counts and phrases were picked out and themes formed based on frequencies (Silverman, 2011). Furthermore, the qualitative data were compared with the quantitative data. This was done by using the frequencies determined in the quantitative analysis to aid in determining the level of importance given to the codes and labels identified and discussed in the qualitative analysis.
Results and discussion
Because this study is largely qualitative, the results and discussion are presented together below. The topics discussed are presented in descending order of frequency as raised by respondents.
Sample characteristics
Thirty-eight usable responses were received. Of these, 25 were female, 11 were male, and two did not specify gender. The spread of respondents by HPCSA registration category is shown in Table 1. The majority of respondents were Clinical Psychologists, followed by Counselling and Educational Psychologists in descending order. No Industrial or Research Psychologists responded, and are likely underrepresented on the PsySSA mailing list. Most respondents had between 1 and 15 years of professional experience, with a minority having more than 15 years of professional experience (Table 1).
Sample characteristics by professional category and years of experience.
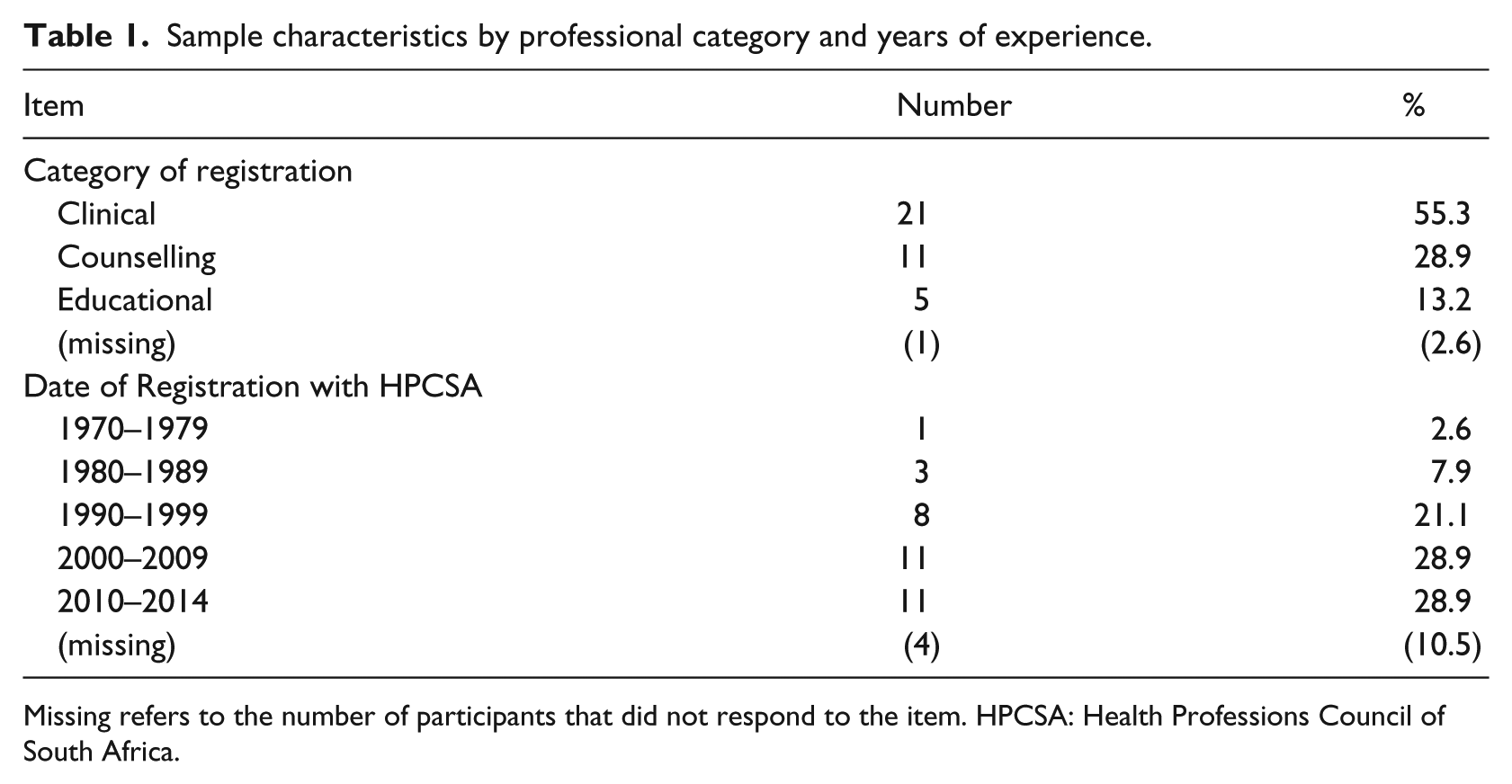
Missing refers to the number of participants that did not respond to the item. HPCSA: Health Professions Council of South Africa.
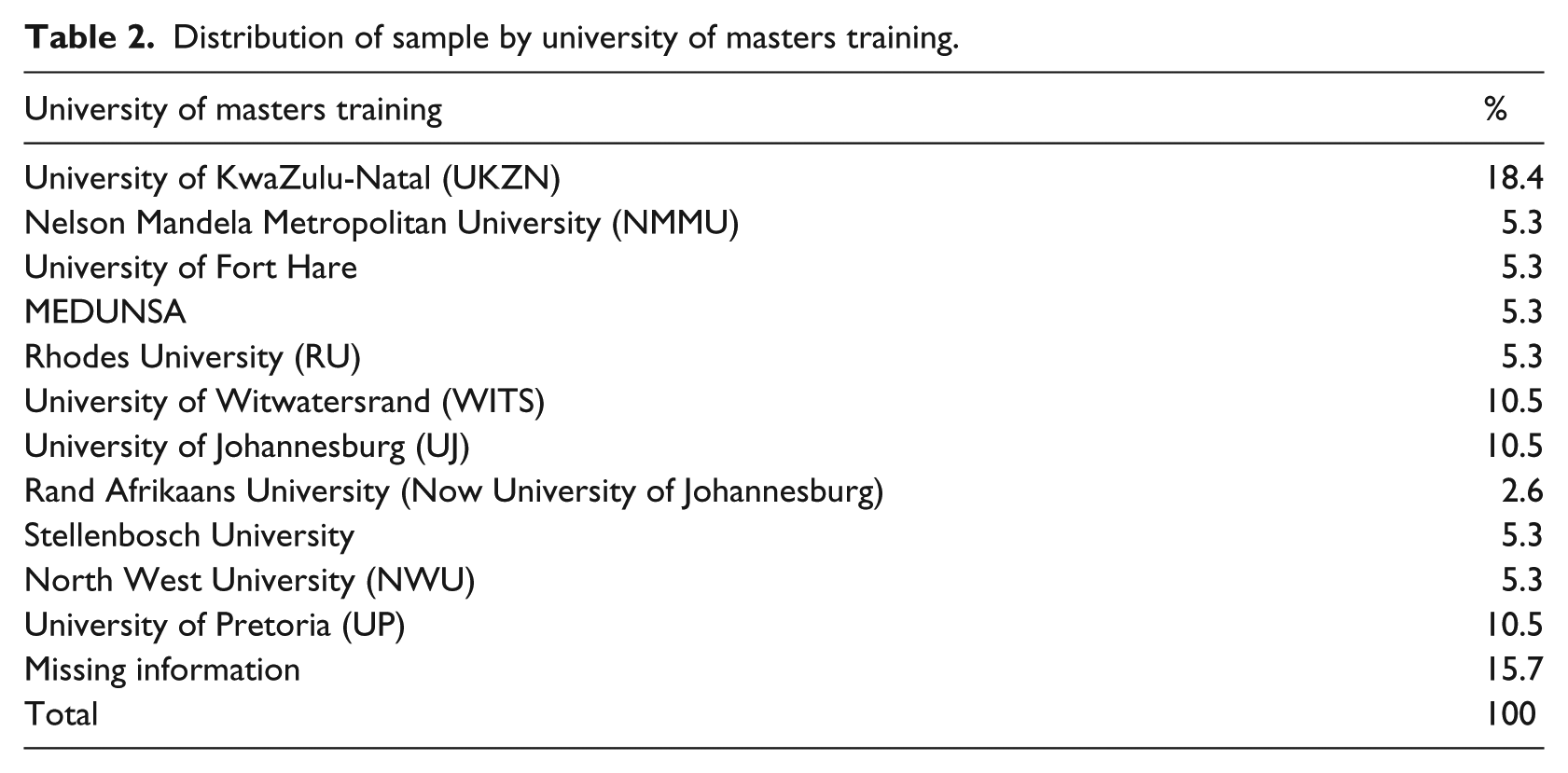
Table 2 shows that the majority of respondents were from the University of KwaZulu-Natal, with most other South African professional psychology training universities represented. Information on university of training was missing for 15.7% of respondents.
Distribution of sample by university of masters training.
Responses to the draft Ethical guidelines: ranking of the most important ethical issues
The most important ethical issue identified was confidentiality, accounting for 28.6% of concerns raised. The second most frequent ethical issue, at 23.8% was competence and the third was emergency situations, accounting for 19.1%. The fourth most important issue accounting for 14.3% was duty to warn. Boundary issues accounted for 9.5%. Finally, the sixth issue was on payment concerns accounting for 4.76%.
Qualitative findings
Participants were asked if any points needed to be developed or added to the draft guidelines. Some additional points were suggested and were grouped in descending order of perceived importance using the headings below.
Confidentiality, privacy, and records
Most participants were concerned about threats to confidentiality in online therapy. This correlates with findings by Wassenaar (2002) showing confidentiality as the most frequently self-reported ethical dilemma by South African psychologists practising conventional face-to-face therapy. Similarly, in a study of the concerns of professionals currently conducting online therapy, confidentiality was the most frequently reported concern (Wells, Mitchell, Finkelhor, & Becker-Blease, 2007).
The issue of ‘unintentional violations of confidential information’ (Participant 35) was identified in the survey. This risk is increased online when the interface used for interaction between psychologist and client is not secure (Palomares et al., 2016). Kanani and Regehr (2003) refer to this in text-based therapy whereby the psychologist may unintentionally e-mail conversations to the wrong person. Another participant, in response to the same question, stated, . . . confidentiality as there is a possibility that there might be a hacker, the client’s family may access some confidential information if the computer is being shared at home. (Participant 32)
Several participants were concerned about the security of records in online therapy. Phrases such as ‘privacy of records’, ‘risk of being hacked’, and ‘security of information exchange online’ were common. It is the psychologist’s duty to ensure confidentiality through methods such as encryption of e-mails and educating clients about passwords and software related to secure interactions as this helps to ensure that only the concerned parties have access to online conversations or the conversation data (APA, 2013; Kanani & Regehr, 2003). This heightened concern about confidentiality may also reflect psychologists’ own lack of competence in managing such dilemmas when practising online therapy.
Competence
Most concerns regarding competence focussed on ‘mastery of the medium’ (Participant 25), in relation to technological difficulties and the nature of the therapeutic relationship. ‘Technological limitation’ was thus proposed as a subtheme as one participant stated, For me it is a problem when there is distortion in the sound and you cannot assess the tone etc. in the voice of the client. Also, if there is a break in the communication and you cannot re-establish it. (Participant 19)
Clay (2017) and McCrickard and Butler (2005) mentioned that psychologists need to be competent in the use of computers, if they are to be competent in online therapy. In the same light, one participant added a suggestion that ‘it should be mandatory that they take formal courses on how to protect the information exchanged between themselves and their clients’ (Participant 32).
Nature of the therapeutic process
The same excerpt from Participant 19 above highlights difficulty in the therapeutic process because of limited access to nonverbal cues from the client. Similarly, due to the nature of current training, it may also be difficult for the psychologist to ‘express empathy’ (Participant 11) and to correctly interpret text (Participant 33). This may be an even greater problem considering the South African context with many diverse cultures and languages in a single nation. Moreover, concern was raised about the fact that the client and psychologist are in different environments and the psychologist has no control of the therapeutic frame. The client’s environment could easily be disturbed by a third party at any point without the psychologist’s awareness, which could influence the therapeutic process. These concerns reflect some anxiety about psychologists’ perceived readiness to work in this modality.
Training
The HPCSA (2006) Annexure 12 for psychology (section 5.1) states, When a psychologist is developing competency in a psychological service or technique that is either new to him or her or new to the profession, he or she shall engage in ongoing consultation with other psychologists or relevant professions and shall seek and obtain appropriate education and training in the new area.
One participant sharing this view of the need for training stated that Before such a service is formalised as a mode to offer a therapeutic service psychologists will have to undergo training not only on how to conduct such a service but it should be mandatory that they take formal courses . . . There will need to be an effective monitoring system in place that will ensure that psychologists do attend courses on a yearly . . . (Participant 32)
This suggests a need for specific training in the practice of online psychotherapy. In relation to the therapeutic process, emphasis should also be placed on training in working with people from diverse cultures as part of competence (Barnett & Scheetz, 2003; Hilgart et al., 2012; McCrickard & Butler, 2005). Some participants, however, pointed out limitations of formal training. For example, Participant 16 stated that Training in technological competence and online counselling is a tall order. Online networks change all the time e.g. Facebook, Mixit, WhatsApp, Instagram, Twitter, etc. How long will the entire training program for psychologists be?
The changing nature of technology, however, cannot negate the need for training specific to online therapy. Regular review of online therapy guidelines will help to address the technological changes, even though guidelines, as a rule, lag behind innovations in practice and research, as mentioned earlier. According to Hilgart et al. (2012), expanded online therapy training should be mainstreamed into professional training programmes to produce competent practitioners. Participant 25 commented by saying, I also think that it would be a good idea to include it in the curriculum of the masters training at universities that are training therapists which would take away the need for this over regulation after training . . . I do agree that all therapists should be educated re the guidelines for practicing responsibly when they do therapy in any form that is not face-to-face.
This proposal for formal initial and ongoing training for online service delivery was linked to the need for specialised training supervision in online therapy. Hilgart et al. (2012) suggest that psychologists practising online therapy should pursue relevant supervision to provide competent online service. The draft ethics guidelines developed in this study (Appendix 1), propose that if a psychologist is to practice solely in online therapy they should undergo a year’s postqualification supervision. One participant responded by saying, I think it is unrealistic to make it a rule that the therapists have to have a year’s supervision in doing on-line counselling as a requirement for them to engage in this modality of therapy. There are not enough therapists who do this kind of work that would be able to do supervision to start with. I would recommend that more, reasonably priced, accessible workshops be held to enable therapists to add the skill to their skill base. (Participant 25)
Emergency situations
Many participants were concerned about how to address emergency situations in online therapy. Participant 21 mentioned that there are ‘no boundaries and no sense of acting on duty to warn or prevent or act immediately on a suicide risk individual’. Another participant’s concerns are expressed below: Emergency situations – you don’t necessarily know the person’s full mental state if you are not able to observe them and interact directly as well as assess non-verbal behaviour. If the client is a danger to themselves or others, who do you report this to? (Participant 10)
The draft ethics guidelines developed in this study propose that the psychologist should only accept a client from a different geographical area if he or she has adequate information and contacts in the same area as the client in case of emergency situations. Having information on emergency resources in the client’s area prior to offering the service (APA, 2013) would help in accessing appropriate immediate intervention where there is need for follow-up or referral to services in the same area as the client (Hilgart et al., 2012).
Duty to warn
A psychologist’s duty to warn refers to their obligation to inform an appropriate third party of any possible harm or intention to harm that the client reveals during their interaction with the therapist (Kanani & Regehr, 2003). Participant 21 mentioned difficulty in acting on this duty by saying there is ‘. . . no sense of acting on duty to warn’, in online interactions. Similarly, Participant 10 asked: ‘. . . If the client is a danger to themselves or others, who do you report this to?’ The psychologist in online therapy is also less able to assess the nature and intensity of the client’s affect, especially anger and potential for violence, which can arguably still be better assessed using nonverbal cues in face-to-face therapy (Kanani & Regehr, 2003).
Verification of identity
This reported concern referred to verification of the identity both of the psychologist and the client. Phrases used by participants to highlight this concern included the following: ‘verifiability of the clinician’s details’ (Participant 27), ‘Guarantee of same person on other end of connection?’ (Participant 33), and ‘no confirmation of the ID of the patient accessing the services’ (Participant 35). Barak (1999) highlights how the Internet ‘makes it is easier for charlatans or professionals without sufficient credentials to offer psychological services’ (p. 240). The draft ethics guidelines proposed in this study suggest that psychologists must encourage clients to verify the psychologist’s registration bona fides on independent formal websites such as the HPCSA web register (see http://www.hpcsa.co.za/Public/FindPractitioner). Such concerns, of course, are not unique to verification of online service providers. Maheu and Gordon (2000) found that very limited information was available to independently verify the qualifications of those providing online mental health services, raising questions about the professional standing and competence of many online service providers.
Although recommendations for verification of the therapist’s identity were included in the draft guidelines (Appendix 1), issues regarding verification of the client’s identity were not addressed. Young (2005) found that clients that accessed online therapy did so because online anonymity made personal disclosures easier. However, this raises concerns about minors accessing online therapy without the consent of a legal guardian (Barnett & Scheetz, 2003; Pope & Vasquez, 2016), even though South African law is fairly permissive regarding child access to care and treatment without parental consent (Strode, Slack, & Essack, 2011).
Informed consent
The ethical and legal requirements of informed consent need to be tailored for online work (London, 2010; Luxton et al., 2016). The draft ethics guidelines produced in this study therefore propose that the psychologist should inform clients about the benefits and limitations of online therapy (APA, 2013), clarify working hours and provide education on how the technology related to this mode of therapy works. The current HPCSA codes (Annexure 12 for psychologists) require written consent for any form of therapy including any electronic communications. Our draft guidelines (Appendix 1) propose that In the case where written consent cannot be obtained . . . consent is valid by virtue of checking a box at the end of the web page . . . Failure to do so would consequently prohibit access to the next page . . . (for) . . . setting up an appointment. Consent may also be obtained by completion of a mini multiple choice questionnaire by the client to show understanding of informed consent. (p. 1)
However, respondents identified limitations of seeking informed consent in this manner: With the online consenting there is no guarantee that the clients do read the information contained on the page. There is a possibility that they just click on ‘agree’ in order to move to the next page that will allow them to receive the service that they are in need of. (Participant 32)
This illustrates the complexity of dealing with issues of identity and informed consent in online therapy.
Online therapy adjunctive to face-to-face therapy
A prominent topic raised was that of online therapy as a standalone modality versus being an adjunct to face-to-face therapy: Have doubts about ‘pure’ online therapy with not at least some face-to-face sessions. Therapy is an embodied process, and I do not think the in-depth, long term work that I do will be possible with at least some face-to-face sessions. (Participant 14)
McCrickard and Butler (2005) suggest that online therapy is most useful in conjunction with face-to-face therapy. Some participants had questions about the difference between being a full-time online therapist and using online therapy when a regular face-to-face client was away for a limited period of time: Perhaps . . . if you do say 10% of your work digitally you would have to go for a year-long supervision and then register with the HPCSA as an online therapist? This would enable those of us who do the odd session digitally when our clients are out of town to continue working, but will protect the public if the therapists work almost exclusively in this way and may have many clients who live outside of their geographical areas. (Participant 25)
This suggests that the proposed guidelines should distinguish between ‘pure’ online therapy and online therapy as an adjunct to face-to-face therapy, possibly incurring different registration requirements.
Age trends
Interestingly, the age of clients was considered to be a factor in determining the acceptability and usefulness of online therapy as anonymity and accessibility of the Internet makes the nature of help-seeking via the Internet appealing to adolescents (Grey, Klein, Noyce, Sesselberg, & Cantrill, 2005; King et al., 2006). One participant said, This counselling will exclude older clients who cannot keep up with these trends; and it will also exclude a number of younger clients who either cannot afford this service or are not techno-savvy. (Participant 16)
Therefore, both client and therapist preferences should be considered.
Impersonal therapy
Even though the draft guideline was noted as useful, respondents were concerned about the client and the therapist being in different environments, making online therapy impersonal. Another participant said that online therapy ‘may be seen as a crutch more than rehabilitation . . . Loss of the immediate interpersonal “people” element may make concepts more clinical and may lead to less interpretation and overall picture of the person’ (Participant 33). On one hand, the impersonal nature of online therapy is problematic. On the other hand, increasing research evidence on the effectiveness of online therapy (APA, 2013; Barak et al., 2008) reveals psychologists’ lack of confidence and skill in assisting clients in a modality that they have largely not been trained in. Translation of skills from face-to-face therapy to online therapy seems to be one of the main concerns expressed by therapists practising online therapy (Goss & Anthony, 2003).
Response to the guidelines
Although there were some useful suggestions for amending the draft guidelines, and some reservations about the guidelines, most (68%) participants rated the guidelines as good or useful, supporting the need and appropriateness of such guidelines for South Africa. One participant said, ‘I think these guidelines are very necessary and timely and should be made available as soon as possible’ (Participant 8). Fewer participants (7.9%) viewed the guidelines as not useful, but this was based on their principled objections to online psychotherapy of any kind.
Points to be added to the draft ethics guidelines
The draft guidelines (Appendix 1) clearly require several modifications based on our study. The guidelines were designed for any form of therapeutic work using online modalities. Suggestions were made to distinguish between pure online therapy and online therapy as an adjunct to face-to-face therapy. A section should be added to the draft guidelines that addresses this mixed modality, and consequently addresses whether ethical requirements should differ according to the nature of online therapy. One participant suggested additional formal registration as an online therapist if more than 10% of therapeutic work is done online. The threshold criteria that warrant registration as an online service provider need to be debated and articulated.
One respondent suggested that section 3.2 of the draft guidelines (Appendix 1), whereby responsibility is placed solely on the psychologist to ensure privacy, should be amended to encourage clients also to take responsibility for ensuring privacy. Management of technological failures and breakdown in communication, due to power failures, for example, were suggested as worth mentioning in the draft guidelines. Similarly, Manhal-Baugus (2001) highlighted the need for procedures to follow in the event of technological failure. Another suggestion was for a screening questionnaire to help the psychologist to determine whether or not a client is suited for online therapy. A distinct suggestion was made to include a ‘Frequently Asked Questions’ section in the draft guidelines. Furthermore, a suggestion was made to have an expert in online therapy that is available via the HPCSA or other organisation (e.g., PsySSA) to advise on questions and ethical dilemmas related to online services. This would be necessary until online service delivery, like online banking, is well established in South Africa.
Another emphasis was on determining the efficacy of client evaluation and assessment without collateral information afforded by conventional physical observation of the client. Such efficacy could possibly be increased by using assessments standardised specifically for online use, acquiring a licence to do so and remaining aware of ‘blind’ test interpretation as suggested in the ‘additional notes’ section of the draft guidelines (Buchanan, 2002, 2003; Hilgart et al., 2012). This might be assisted by online video modalities as opposed to text-based therapy. Case management of emergency situations was also emphasised, revealing reservations about how the draft guidelines (Appendix 1) addressed this dilemma. This highlighted the importance of identifying appropriate referral services in the same geographical area as the client wherever possible (Hilgart et al., 2012), raising the possibility of a network of proximal professionals as a prerequisite for conducting online therapy. These suggestions highlight the need for further research and clear guidelines on the nature and ethics of online therapy.
The research has several limitations. Administration of the survey via e-mail meant delivery and response rates could not be verified. Only a subset of HPCSA registered psychologists were represented in the study. Regardless, the sample roughly reflected the proportions of HPCSA registered Clinical, Counselling, and Educational Psychologists, suggesting some generalisability. This study did not address the additional legal and ethical implications of cross-border service delivery. A question on respondents’ actual experience with practice of online service delivery and a distinction between text-based and video streaming would have been useful in refining analyses of response patterns. Perceptions of a particular type of online therapy seem to be based on the particular therapist’s exposure and preference (Chipise, 2012, 2015). Response bias and response misinterpretation would have been reduced with an option to probe responses. The study and proposed guidelines are nonetheless the first in South Africa for further consideration by practitioners and regulatory authorities.
Conclusion
This study developed and sought psychologists’ comments on draft South African online therapy guidelines. Similar methods have been used to develop and refine ethics codes for psychologists internationally (Wassenaar, 1998). Despite a minority of participants believing that online therapy should not be a professional service delivery modality, the majority of participants rated the draft guidelines as useful. Even though the draft guidelines were positively endorsed, some concerns about the ethical dilemmas and practical ways to practice in this modality were highlighted and suggestions were made to improve the guidelines. Most participants identified confidentiality as the dominant concern in online therapy. Another dominant concern was that of adequately and ethically managing emergency situations. A suggestion was that online therapy only be used as an adjunct to traditional therapy rather than a standalone mode of therapy. Suggested additional points for the draft guidelines emphasised concerns about competence and the need to protect both the therapist and the client. With the current surge of provision and accessibility of mental health care online, a set of guidelines could supplement Evans’ (2018) work and assist South African psychology in providing guidance on a par with some developed countries. Furthermore, developing special guidelines may ‘help improve service delivery in practice areas in which in which there is no recognized consensus about expectations’ (OPA, 2009, p. 1).