
Abstract
Inadequate investment in mental health care by the governments of both high- and low-income countries contributes to recurrent challenges of uneven distribution of and access to mental health services between urban and non-urban communities. While recent research has acknowledged the role of mental health in well-being and the cost of failure to invest in the sector, prioritising mental health to the same degree as physical health remains a challenge. This article highlights the unequal distribution of mental health services, and psychological services in particular, in KwaZulu-Natal. This is achieved by considering the background of psychology in South Africa and KwaZulu-Natal and then examining the ratio of clinical psychologists to the KwaZulu-Natal population. Furthermore, the article explores the geographical distribution of psychological services in KwaZulu-Natal and concludes with a discussion of the impact of uneven mental health service distribution on service provision and utilisation in non-urban areas of KwaZulu-Natal.
Influential bodies such as the World Health Organization (WHO), Pan American Health Organization, European Union Council of Ministers, World Federation for Mental Health, and the United Kingdom Royal College of Psychiatrists have raised concerns about failure to pay adequate attention to mental health, which they assert is a fundamental part of health (Saxena, Thornicroft, Knapp, & Whiteford, 2007). Concerns highlighted by research findings indicate the serious impact of mental disorders on the global burden of disease (Burns, 2010; Prince et al., 2007; Saxena & Skeen, 2012; WHO, 2013). Steel et al. (2014) in their systematic review and meta-analytic study (1980–2013) estimated the global prevalence of common mental disorders to be one in five respondents who met the diagnostic criteria within a year of assessment. This high incidence of mental disorders demonstrates the magnitude of mental health needs and the significance of prioritising mental health.
The WHO and global research community advocate investing in mental health to redress its omission from the millennium development goals’ agenda. According to researchers, such omission not only undermines optimal health benefits, but is also costly and constitutes a human rights violation (Burns, 2010; Prince et al., 2007). The WHO’s (2015) call for attention to the promotion of the dignity of persons living with mental illness further contributes to ensuring that, globally, mental health issues receive due consideration. Continued global mental health discourse further emphasises the importance of attending to mental health and other health issues equally. Researchers also state that failure to attend to mental health is detrimental to the well-being of the world population (Prince et al., 2007). Furthermore, poor attention to mental health incited multiple calls to revive and accelerate principles of the Alma Ata Declaration which encourages an integrated and comprehensive health care system through the primary health care (PHC) approach (Kakuma et al., 2011; Lund et al., 2012; Petersen, Ssebunya, Bhana, Baillie & MhaPP Research Programme Consortium, 2011; WHO & World Organisation of Family Doctors [WONCA], 2008). Likewise, Lawn et al. (2008) emphasised upholding the declaration’s core values of universal access to care, equity, community participation, inter-sectoral collaboration, and appropriate use of resources.
The World Health Assembly adopted the Comprehensive Mental Health Action Plan 2013–2020 and urged United Nations member states to act on agreed objectives of strengthening leadership, governance, and provision of integrated mental health services to meet proposed mental health targets (WHO, 2013). The objectives mentioned above are relevant to this article as it also supports integration of psychology services into the PHC package of health care. While commendable consideration of mental health has been observed globally, the persistent high prevalence of mental disorders indicates that focused efforts, particularly in low- and middle-income countries (LMICs), remain essential. LMICs have unique contexts that require special attention. Like other LMICs, South Africa’s health budgets, infrastructure, and human resources should reflect robust investment in mental health, as recommended by the WHO (2013).
History of mental health services in South Africa
Although high-income countries have more mental health resources than LMICs, the imbalance between available resources and necessary services is noted globally (WHO, 2011). However, the impact of this imbalance is mostly prevalent in the African continent where the health care demand is much higher than available resources. While South Africa is economically and socio-politically better off than most African countries, it continues to reflect perceptible ramifications of economic disparities from the apartheid regime. The apartheid regime promoted segregation of South African citizens along geographic, racial, cultural, and class lines. In addition, during apartheid, better-resourced mental health services were accessible to the privileged minority. The rest of the population, particularly in non-urban communities, relied on poorly resourced and unevenly distributed mental health services that did not uphold human dignity (Burns, 2011; Cooper, 2014). Key societal resources in education, health, and the economy continue to reflect this inequality. Similar segregation along race and gender lines persists in the profession of clinical psychology (Cooper, 2014; Pillay & Siyothula, 2008).
The advent of democracy and efforts of professional associations like the Psychological Society of South Africa have played a major role in unifying and changing the face of South African psychology (Cooper, 2014). The Mental Health Care Act (MHCA), No. 17 of 2002, has also been instrumental in driving access to mental health care and upholding the rights of persons with mental illness (Burns, 2009). The MHCA is considered to be one of the accolades of South Africa’s democracy as it promotes a shift from mainly hospital-based mental health services to decentralised mental health care. One of the key factors of the MHCA is the promotion of collaboration between stakeholders and active participation of communities in their own care. However, concerns about the implementation of the Act and its effectiveness through designated levels of care for optimal benefit have been raised. Constraints in infrastructure, financing, and human resources are among the hurdles that hinder optimal implementation and benefits of the Act (Ramlall, 2012; Ramlall, Chipps, & Mars, 2010).
The 2012 Ekurhuleni Declaration on Mental Health signalled a hallmark in persuading the South African government to consider the plight of persons living with mental illness and implementing measures that safeguard their dignity. The declaration encouraged the government to respond to the call by the WHO to invest in mental health by making South Africa a signatory of the United Nations Convention on the Rights of Persons with Disabilities (Burns, 2009; WHO, 2013). The National Mental Health Summit held in April 2012 contributed to the development of a detailed and aspirant South African National Mental Health Policy Framework and Strategic Plan, 2013–2020 (Department of Health [DOH], 2012; Stein, 2014). In this document, the government upholds the need for dignity of mental health care users by committing to the provision of accessible, quality, and adequate mental health services. The government further affirms that access to mental health care is not a privilege but a constitutional human right (Burns, 2009). Nevertheless, while the policy provides a comprehensive framework for the delivery of mental health services in South Africa, there are concerns that implementation has not followed with the same enthusiasm (Morgan, 2015). Hence, researchers caution against the ripple effects of apathy and negligible investment in mental health remain pertinent (Lund et al., 2012).
The integration of mental health and clinical psychology services into PHC in KwaZulu-Natal
Integration of mental health services into PHC is an international vision of bringing services closer to the people (Petersen et al., 2009; WHO, 2001). The KZN DOH responded to the MHCA and the WHO’s call to integrate mental health services into PHC by forming a task team in 2004 to facilitate this process. The task team was mandated with examining and integrating all available mental health documents into a new document called The Strategic and Implementation Plan for Delivery of Mental Health Services in KwaZulu-Natal (KZN) (Mkize, Green-Thompson, Ramdass, Mhlaluka, & Dlamini, 2004). The purpose of this document was to guide the implementation of mental health service delivery in KZN. This newly constructed document included operational plans, time frames, and specific recommendations for community mental health services and forensic psychiatry. It also emphasised the provision of adequate human resources for implementation of its recommendations (Mkize et al., 2004).
The envisaged benefit of integrating mental health into PHC was the promotion of inclusive health care service that caters for the intricate health needs of communities (Bhana, Petersen, Baillie, Flisher, & The MHaPP Research Programme, 2010). However, implementation of the much-anticipated integration of mental health services into PHC is imbued with challenges (Bhana et al., 2010). While the constructed document provided a comprehensive framework for the delivery of mental health services, scarcity of specialist mental health professionals, including clinical psychologists, hinders availability of the proposed members of the multi-disciplinary team at PHC level. The PHC level is considered to be the community’s first point of contact with the health care system. The task team’s framework proposed ‘staggering’ the availability of specialised mental health team members (clinical psychologist, social worker, and occupational therapist) on a part-time basis in community health centres and district hospitals, with the full team (including a psychiatrist) only available at regional and tertiary levels (Mkize et al., 2004). In reality, particularly in non-urban settings, most PHCs have none of these team members. While this document pioneered decentralisation of mental health services, delayed involvement of the full multi-disciplinary team indicates a missed opportunity of early investment in mental health and ensuring that it forms an integral part of PHC. Furthermore, failure of clinical psychology as an independent profession to assert and advance its position in the provision of mental health perpetuated the traditional medical hospicentric model. Hence, clinical psychology services remain in hospitals where leadership of the mental health team is often under psychiatry and the independence of clinical psychology is unclear.
Petersen et al. (2009) assessed the progress of decentralisation and comprehensive integration of mental health services into PHC in KZN and found that progress is hindered by ‘lack of resources within the primary care package’ (p. 140). In addition, Stein (2014) states that decentralisation of mental health services seemed to have been misunderstood to mean disassembling experienced mental health teams and views this kind of thinking as a crucial factor contributing to the slow and negligible progress in integration of mental health services into PHC. The adverse effect of decentralisation was removing stand-alone mental health clinics from the community back to hospitals. Furthermore, placing mental health services in the same premises with other health care services, without the accompanying resources, expertise, and commitment, has stalled successful integration of mental health into PHC. The majority of PHCs in KZN do not have support services of multi-disciplinary teams, training, and supervision for non-specialist mental health care workers. More than a decade later, the task team’s proposal of integrating clinical psychology services into PHC has not been implemented. Despite initiatives from clinical psychologists of the Midlands Hospital Complex in the mid-1980s (Pillay & Kramers-Olen, 2014), little progress has been made. While these efforts contributed to community psychology services, integrated and comprehensive health services at PHC level have not gathered the desired momentum in KZN.
It is disheartening to observe that involvement of the multi-disciplinary team at PHC level has not been effected and non-urban communities in KZN continue to struggle to access optimal mental health services. To date, there are still non-urban health districts in KZN with only one clinical psychologist expected to meet the psychological needs of approximately half a million people. As a result, these districts rely on monthly services of ‘fly in’ clinical psychologists transported by the Air Mercy Services from metropolitan areas (Pillay, Kometsi, & Siyothula, 2009; Pillay & Kramers-Olen, 2014). While this effort is better than the absence of clinical psychology services, it is limited by irregular visits as flights depend on suitable weather conditions. In KZN, only two community health centres have resident psychologists (KwaZulu-Natal Department of Health, 2015).
The introduction of community service for newly qualified clinical psychologists by the National Department of Health has brought limited relief to the lack of mental health care in rural areas. Distribution of placements between urban and rural areas is inequitable, and newly qualified clinical psychologists prefer urban areas to rural areas where services are needed most. While the intention of mandatory community clinical psychology service was admirable, there is often lack of service continuity due to delays in completion of a dissertation which qualifies new clinical psychologists to start community service (Pillay & Harvey, 2006). This defeats the purpose of this government initiative to address human resource disparities in disadvantaged rural areas and improve local access to all health services (DOH, 2006). These recurrent human resource disparities and limited progress in the integration of mental health services into PHC reflect inadequate investment in mental health and the prioritisation of mental health care in South Africa (Bhana et al., 2010; Mkhize & Kometsi, 2008).
The distribution and ratio of psychologist to population in KZN
Fragmented and skewed distribution of health resources and personnel between rural and urban areas, public and private sectors, high-income countries and LMICs, and primary and tertiary health care contexts is well documented (Ashmore, 2013; Burns, 2009; Cooper, 2014; De Jager, Hofman, Khan, Volmink, & Jina, 2012; Saxena et al., 2007). Prior to 1994, South Africa had 14 disjointed health departments. Ten years into democracy, in 2004, the DOH acknowledged that efforts to redress past disparities had not fully materialised but had instead evolved into a two-tiered health care system (the public and private sectors) which perpetuated inequality. According to Ashmore (2013), the imbalance in these contexts continues to contribute to the ongoing struggle to effectively manage diseases and maintains their high impact on the global burden of disease. Ashmore’s claim is supported by the documented research on the pervasive impact of South Africa’s quadruple disease burden (HIV and tuberculosis; chronic illness and mental health; injury and violence; and maternal, neonatal, and child health) (Burns, 2011; Coovadia, Jewkes, Barron, Sanders, & McIntyre, 2009) and increased susceptibility of non-urban areas to these diseases (Burns, 2011).
According to Ashmore (2013), South Africa has adequate supply of health workers above the expected benchmark per 1000 people as stipulated by the WHO’s Global Atlas, and the minimum benchmark of 2.5 health workers per 1000 people, as defined by the Joint Learning Initiative in 2004. Ashmore (2013) states that this health worker/population ratio sets South Africa above most African countries and affirms its status as a middle-income country. However, he also points out that inequitable distribution of health workers between and within South African provinces, and between public and private sectors, only caters for health needs of the advantaged minority while the majority continue to have limited access to health care even during the democratic era. This undermines South Africa’s success in addressing public health problems and developmental challenges (Ashmore, 2013; De Jager et al., 2012).
Contrary to the health care situation in LMICs, high-income countries are reported to have a ratio of psychiatric health workers to population that is about 200 times higher than in LMICs (Ashmore, 2013). These figures reflect inequalities in distribution of mental health services across the world (WHO, 2014). Likewise, inequity in distribution of clinical psychology services between health districts in KZN remains prevalent as illustrated in Table 1. Figure 1 also displays the distribution of psychologists in KZN per health district. The map below depicts the concentration of clinical psychologists in two metropolitan districts of uMgungundlovu and eThekwini, followed by the semi-urban Ugu district.
Ratio of clinical psychologists to population in KZN health districts.

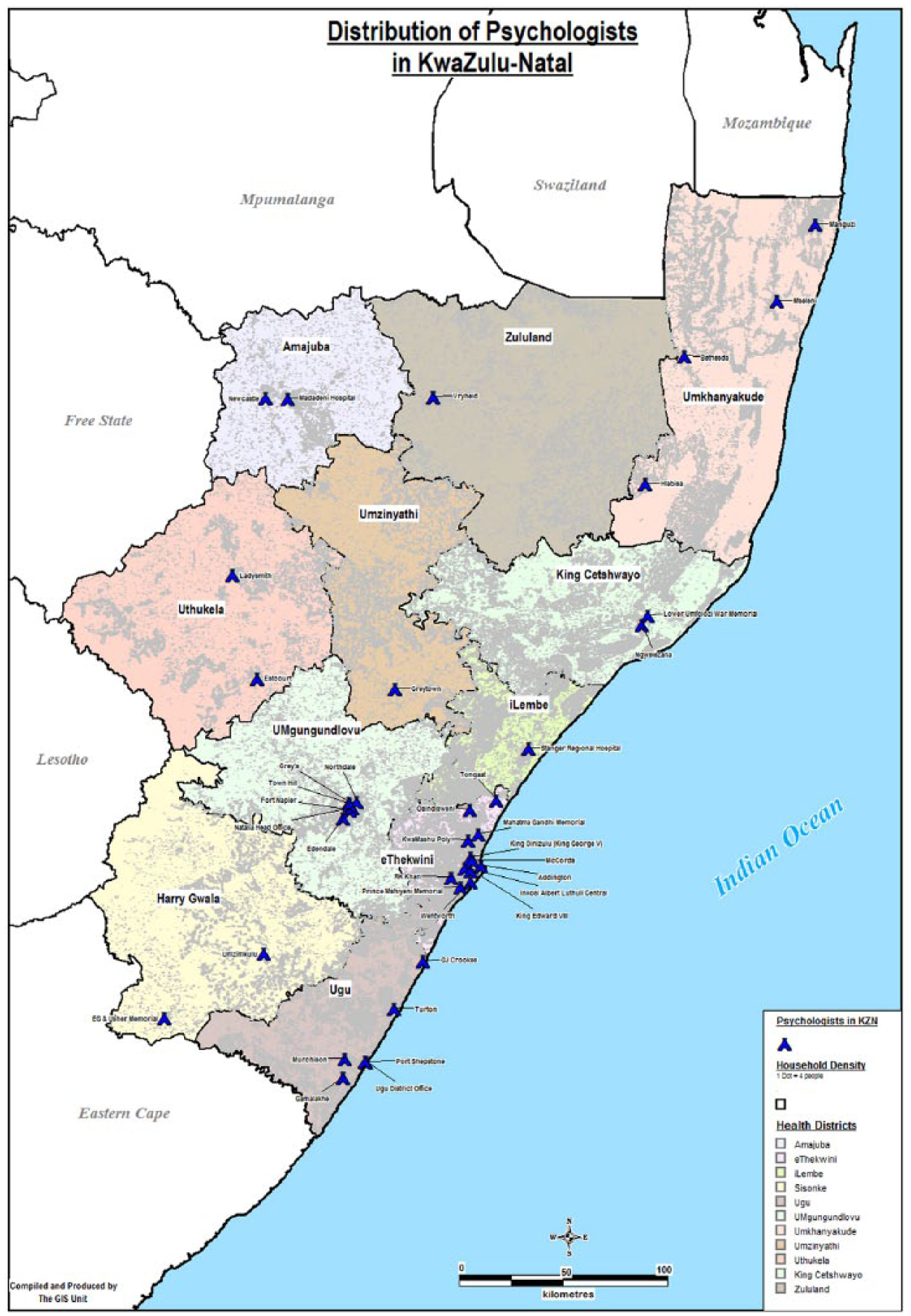
Distribution of clinical psychologists in KwaZulu-Natal.
While the study by Lund et al. (2012) found that in South Africa the ratio of clinical psychologists (0.32/100,000 population) is higher than that of psychiatrists (0.28/100,000 population), it is important to consider the duration and frequency of clinical psychologists’ sessions. Ideally, clinical psychologists allocate at least an hour for each consultation and often have follow-up sessions. This means that the clinical psychologist can only see five to six patients per day if depth and quality of service is to be maintained. Furthermore, as part of quality mental health, efficiency of psychological interventions should translate into enduring and generalisable self-regulation skills that can promote autonomy and productivity (Barry, Clarke, Jenkins, & Patel, 2013). Viewing clinical psychologists’ work against this backdrop, it is evident that there are inadequate numbers of clinical psychologists to meet the needs of the South African population particularly in non-urban areas.
Challenges that impact service provision and utilisation
While the role of mental health care in effective management of all health concerns is well documented (Mayosi et al., 2012; Petersen et al., 2015; WHO & WONCA, 2008), there is a dearth of research focusing on the role of clinical psychology. Like mental health care services in general, the effectiveness of clinical psychology services relies on availability, mutual collaboration, and support for both service providers and service users. Some of the factors that influence effectiveness of clinical psychology interventions are discussed below.
Human resource constraints
The enduring human resource shortage in the health sector is a global concern that impedes universal health coverage (Campbell et al., 2013). Considering that mental health care relies on human resources instead of advanced technology or equipment (Stein, 2014), continued concerns about scarcity of mental health personnel and its impact on effective service delivery, particularly in LMICs, is justified. This scarcity is well documented in the WHO Mental Health Atlas Series (WHO, 2011, 2014; WHO, Department of Mental Health, & Substance Abuse, 2005). In LMICs, concerns over the scarcity of human resources for mental health is accentuated by concentration of available mental health professionals in urban areas, while susceptible rural areas remain poorly attended (Burns, 2011). While unpacking reasons for health professionals’ preference to work in urban areas is beyond the scope of this article, frustration from professional isolation, poor infrastructure, and lack of resources like formal interpreters (Elkington & Talbot, 2015) for providers who do not speak the local language could be among the contributing factors. South Africa, like most LMICs, still faces repercussions of underdeveloped and under-resourced non-urban areas (Burns, 2011) despite commendable efforts of the democratic government to redress these injustices of the apartheid system. The government also introduced monetary incentives for staff working in non-urban settings; however, this effort has not improved the situation as much as it was anticipated. While Campbell et al. (2013) propose striving for a match between distribution of human resources for health and population needs, the majority of non-urban communities continue to operate with inadequate health personnel, particularly in mental health. Pillay and Kramers-Olen (2014) point out that an insufficient number of trained clinical psychologists perpetuate the imbalance between mental health needs and service provision in underprivileged communities. Furthermore, sparsely distributed clinical psychology services contribute to the poor awareness of the role of clinical psychologists. This frustrates both psychologists and service users, as their expectations from consultations are often incongruent.
Access to mental health services
Provision of quality mental health care is threatened by inaccessibility of services. Mental health services stem from an era where services were located in the tertiary level of health care in specialised psychiatric hospitals. These health care facilities were not easily accessible to communities as they required a complex referral process and out-patient follow-up services were provided at stand-alone mental health clinics. Access to mental health services in non-urban areas should not only be narrowly viewed from the angle of availability of services and human resources. For example, Ruane (2010) states that language and class differences are barriers to accessing psychological services. Therefore, access to services should consider the geographic layout of the catchment area and affordability of transportation to health facilities which is often costly for non-urban service users (Mkhize & Kometsi, 2008; Pillay et al., 2009; Swarts, 2013). With the rising cost of living, unemployment, and poverty in LMICs particularly affecting previously disadvantaged non-urban communities, funding mental health needs is frequently overtaken by basic needs like access to food and shelter. Mental health needs which are often inaccurately perceived as not life threatening tend to be pushed down the priority list until it is too late to manage them with simple interventions. The WHO (2013) in the mental health action plan 2013–2020 states that ‘People with mental disorders experience disproportionately higher rates of disability and mortality’ (p. 7). The assertion that approximately 75% of people with a mental illness have no access to services and that this constitutes the mental health treatment gap prevalent in LMICs, including South Africa, should be understood against this background (Williams et al., 2008; WHO, 2016).
The WHO’s Mental Health Gap Action Programme (mhGAP) intends to enhance services for mental, neurological, and substance use disorders particularly in LMICs (WHO, 2016). However, access to services should not be limited to only taking services to the communities and assuming that physical presence of the mental health component within the PHC setting is sufficient. Contact with the service point without the necessary resources cannot meet complex mental health needs. Access to services should translate to service users’ ability to utilise and benefit from the service demonstrated by the effective management of identified mental disorders and optimal quality of life. While deinstitutionalisation and dissolution of stand-alone psychiatric clinics initiated integration of mental health services into PHC, there has been a failure to provide access to expert mental health professionals, which compromises the quality and benefit from mental health care (Stein, 2014). Therefore, access to services should consider that mental health care, including psychological interventions, are rarely a once-off occasion but constitute commitment to regular follow-up sessions for lasting impact. Failure to appreciate the long-term nature and value of the mental health consultation process impedes effectiveness of care, despite its accessibility. Hence, viewing access to services in a continuum of physical contact with the service point, quality and relevance of the service rendered, how the service is perceived and received and service impact in improving the quality of life could contribute to the service user’s satisfaction and adherence to treatment. Therefore, access to services should consider availability, utilisation, and benefit from the rendered mental health services.
Conceptualisation of mental illness and utilisation of services
Different communities explain mental health issues in ways relevant to their specific contexts and their worldviews. Cultural explanations of mental illness dominate mental health issues. Inherent to these explanations is the stigma attached to mental illness which influences help-seeking behaviours (Jorm et al., 1997; Mkhize & Kometsi, 2008; Patel et al., 2007; Shai & Sodi, 2015). To address stigma, Lund, Kleintjes, Kakuma, Flisher, and The MHaPP Research Programme Consortium (2009) recommend investing in community involvement through establishment of a multi-sectoral community collaborative management forum. According to Lund et al. (2009), this collaboration can reduce stigma and encourage community control over their mental health. While this approach can alter how mental health is viewed and received, awareness that non-urban communities continue to rely on traditional healing interventions for chronic and manageable mental health needs is important. Shai and Sodi (2015) identified multiple pathways to health care which include both Western and traditional health care, depending on whether symptoms are acute or chronic. An earlier national study on traditional healers’ treatment of common mental disorders in South Africa by Sorsdahl et al. (2009) found that alternative practitioners including traditional healers and religious advisors appear to play a notable role in the delivery of mental health care services. Labys, Susser, and Burns (2016) confirmed the complexity of pathways to mental health care in rural South Africa and found that more than half of service users reported no contact with formal health care services. Moreover, those authors proposed consideration of services beyond formal health services and community-based interventions. It must be borne in mind that perceptions and understandings of mental health issues influence the types of services that are utilised and these should be considered in service planning and development. The influence of the cultural context in conceptualising mental illness, mental health needs, and importance of cultural sensitivity in mental health service delivery is well documented.
Understanding of clinical psychology in non-urban settings
The previous tiered structure of the South African health system meant that mental health and clinical psychology services were only available at tertiary level which limited access to these services (Cooper, 2014). Clinical psychologists’ roles and scope remain misunderstood not only by service users but also by providers and caregivers (Rhohleder, Miller, & Smith, 2006; Swarts, 2013). While each professional has a unique health care role, focus area, and scope of practice, this misunderstanding affects the expectations and outcomes of consultation. In the PHC settings, inappropriate referrals are commonplace and such referrals are rarely explained to the health care users. Valuable consultation time is taken up as the service provider required to explain his or her role. Lack of understanding of each mental health service providers’ role affects the treatment outcomes and formation of a strong therapeutic alliance (Ssebunya, Kigozi, Ndyabanangi, & MhaPP Research Programme Consortium, 2010) and contributes to a high rate of once-off sessions (Swarts, 2013). Therefore, beneficial interventions are disrupted by dissonance of expectations and goals between service providers and service users (Jorm et al., 1997).
In addition, psychological services in non-urban settings compete with traditional and medical models of care, where service users often leave sessions with concrete evidence of consultation that can be used between sessions and requests for medication at the end of the consultation are common. Mental insights or reflections from a psychological consultation may not be viewed as equally effective. The unintended effects of unclear understanding of the clinical psychologists’ role may lead to underutilisation of the few available services and dissatisfaction for both psychologists and service users.
Conclusion
Research has shown that people living in non-urban settings are equally susceptible to mental illness and have complex mental health/ psychological needs. Considering that integration of mental health services into PHC is an international drive, concerted efforts to include clinical psychology services in all levels of care in non-urban settings is necessary to achieve global mental health coverage.
Collaboration between the department of health and training institutions to find robust means to mitigate the current integration challenges are necessary. Therefore, introducing middle-level workers such as registered counsellors could provide relief. They are not only an already available resource with psychological training, but they also have a clearly defined scope of practice (Health Professions Council of SA, 2004) to perform basic psychological and primary mental health screening, basic assessment, and psychological interventions. Furthermore, community health workers are effectively used to meet non-specialised health needs. Adopting a similar approach in mental health care could facilitate early identification, support, and timely referral of people in need of mental health services. While this is not a suggestion to replace clinical psychologists by registered counsellors and community health workers, utilising existing resources could avail the limited number of clinical psychologists, particularly in non-urban areas to provide training, support, supervision, and specialised psychology services. Considering financial and human resource constraints in the public health sector and the reality of the prevalence of mental illness, the department of health should find innovative, flexible, and cost-effective ways of prioritising mental health services. Adopting such task sharing strategies as recommended by the WHO and other researchers could contribute to integrating psychology services into PHC. Furthermore, given the growing advancements of technology in health care, public mental health care should also explore strategies to utilise this medium of communication to optimise access, support, and service delivery in under-resourced settings.
Footnotes
Funding
The author(s) declared receipt of the following financial support for the research, authorship, and/or publication of this article: The Research was funded by Phd funding from the University of KwaZulu-Natal, and not by a specific grant from any funding agency in the public, commercial, or not-for-profit sectors.