
Abstract
Attention-deficit hyperactivity disorder is one of the most common disorders that can occur in children. The symptoms are thought to result from a deficit in executive functions. This study investigated whether children with attention-deficit hyperactivity disorder subtypes differed in behavioural planning and response inhibition, two of the domains of executive functioning, from a control group without attention-deficit hyperactivity disorder symptoms. Furthermore, it examined whether the three attention-deficit hyperactivity disorder subtypes differed from each other in terms of performance. The sample (n = 320) consisted of primary school children, aged between 6 and 14 years, from the Moletjie circuit (Limpopo). It consisted of an attention-deficit hyperactivity disorder group (n = 160) and a control group (n = 160). The Disruptive Behavioural Disorder rating scale was used to establish the symptoms of attention-deficit hyperactivity disorder. The Tower of London was used to measure planning ability, and the inhibition subtest (arrows and shapes) from the NEPSY-II (Developmental Neuropsychological Assessment, second edition) to measure response inhibition. Analysis of variance was employed to establish differences in subtype, gender, and age group. The results showed that children with the combined attention-deficit hyperactivity disorder subtype demonstrated significantly more deficits than the control group, in both behavioural planning and inhibition control. No significant differences between the hyperactive/impulsive and inattentive attention-deficit hyperactivity disorder subtypes and the control group were found. Gender and age did not influence performance with regard to planning and inhibition tasks. Correlations between planning behaviour and response inhibition were low, which suggests that they are distinct processes.
Keywords
According to the American Psychiatric Association (2013), attention-deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder, with onset in childhood, that often persists into adulthood. ADHD is a highly heritable condition, caused by multiple genes and affected by environmental risk factors (Thapar & Cooper, 2016). The worldwide prevalence of ADHD in children is approximately 5.3% (Polanczyk de Lima, Horta, Biederman, & Rohde, 2007). A study conducted in South Africa (Limpopo province) by Meyer, Eilertsen, Sundet, Tshifularo, and Sagvolden (2004) found the prevalence to be 5.6%, similar to that found in Western countries. The male-to-female ratio was found to be 4:1 in clinical samples, and 2.4:1 in population studies (Faraone et al., 2015; Polanczyk et al., 2007). The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)recognises three presentations (previously called subtypes): predominantly inattentive (ADHD-PI, ±45%), predominantly hyperactive-impulsive (ADHD-HI, ±21%), and the combined presentation (ADHD-C, ±34%) (Woo & Rey, 2005).
ADHD is not only a behaviour disorder, characterised by hyperactivity, impulsiveness, and inattention, it is fundamentally a cognitive disorder, a developmental impairment of executive functions (EFs), which are the controlling system of the brain (Brown, 2009; Ciuluvica, Mitrofan, & Grilli, 2013). Symptoms of ADHD arise from a primary deficit in specific EF domains, such as response inhibition, working memory, set-shifting, and planning (Ciuluvica et al., 2013). Some of the executive difficulties that children with ADHD experience include difficulty with organisation, problem-solving, and planning behaviour. As a result, they experience problems with social skills, and they exhibit low self-esteem, low frustration tolerance, and impaired academic performance (Rhodes & Kelley, 2005).
Executive dysfunction is generally attributed to structural and functional frontal pathology (Faraone et al., 2015; Willcutt, Doyle, Nigg, Faraone, & Pennington, 2005). The dorsolateral prefrontal cortex (PFC) is linked to working memory, while the ventromedial PFC is linked to complex decision-making and strategic planning (Cortese et al., 2012; Faraone et al., 2015). Neurotransmitter circuits are involved in EFs, with the dopamine system, especially, playing an essential part in planning and cognitive flexibility (Arnsten & Li, 2005; Sagvolden, Johansen, Aase, & Russell, 2005). Optimal levels of dopamine are essential for prefrontal functioning. A hypofunctioning mesocortical dopamine branch will cause poor behaviour planning in EFs (Sagvolden et al., 2005).
In this study, the focus was on two EF domains frequently cited in the literature, namely, behaviour planning and response inhibition (Faraone et al., 2015; Miyake et al., 2000; Willcutt et al., 2005), which are often linked to the abnormal functioning of the PFC (Niendam et al., 2012; Stuss, 2011). According to Miyake et al. (2000), these EF domains are moderately linked to each other but are also separable. Children with planning deficits have insufficient problem-solving strategies, which in turn compromises their learning ability at school. On the other hand, children with ADHD, with deficits in inhibitory control, act without thinking. Both deficits contribute to their inability to complete tasks and to overall poor performance at school.
Behaviour planning
Behaviour planning is one of the active components of EF deficit in ADHD; it is defined as the categorising and organising of the steps and elements required to carry out an intention (Chiang & Gau, 2014). According to Allain et al. (2005), planning involves the ability to categorise behaviour in order to achieve a specific goal and to envisage the series of intermediate steps required to achieve it.
A study by Kofman, Gidley Larson, and Mostofsky (2008) stated that children with ADHD exhibited poor performance in any work where planning or a proper strategy was needed. Nigg, Blaskey, Huang-Pollock, and Rappley (2002) also found that children with ADHD-C typically had problems with planning ahead. However, Geurts, Verté, Oosterlaan, Roeyers, and Sergeant (2005) found that children with ADHD did not differ from normal controls with regard to planning. Problems with communication and socialisation skills, as well as reading ability, have been associated with planning deficiencies in children with ADHD (Clark, Prior, & Kinsella, 2002).
Structural and functional neuroimaging studies have shown that children who have ADHD are highly deficient in making use of the striatal–prefrontal and the cerebellar–prefrontal systems (Krain & Castellanos, 2006; Mostofsky, Lasker, Cutting, Denckla, & Zee, 2001). Adequate research support has been provided for the role of the PFC in planning capability (Alvarez & Emory, 2006; Unterrainer & Owen, 2006).
Response inhibition
The second EF domain examined in this study concerned the ability to suppress irrelevant stimuli or behavioural impulses to enable goal-directed behaviour (Barkley, 2001; Miyake et al., 2000). Studies conducted by Blair and Razza (2007) and Espy and Bull (2005) stated that inhibitory control predicts children’s academic achievement across domains in early childhood and during their transition to formal schooling. We can, therefore, conclude that inhibitory control is one of the key skills for the early fundamental achievements in the field of education (McClelland et al., 2007).
According to Geurts et al. (2005) and Chhabildas, Pennington, and Willcutt (2001), symptoms of inattention account for the lack of response inhibition in children with ADHD. In terms of the different ADHD presentations, Nigg et al. (2002) found that children with ADHD-C had more problems with response inhibition than children with predominantly inattentive subtype of ADHD (ADHD-PI). It remains unclear whether deficits in response inhibition are related to ADHD-C or whether they are also present in ADHD-PI. The inconsistency may be due to methodological differences in the various studies.
The PFC guides attention and oversees hidden responses to both externally and internally generated stimuli. The PFC dysfunction in ADHD is found to be located in the right hemisphere and can offer a behavioural disinhibition profile (Arnsten & Li, 2005). The role of the PFC in dopamine functioning is relevant to ADHD since attention response deficiencies are caused by hypofunctioning mesocortical dopamine branches, which results in a lack of inhibition control (Arnsten & Li, 2005; Sagvolden et al., 2005; Tripp & Wicken, 2009).
This study aimed to establish whether children with ADHD differed from a neurotypical control group in behavioural planning and response inhibition and whether the inattentive, hyperactive/impulsive, and combined presentations differed from each other in this respect. The study further tried to establish whether planning and inhibition responses were related.
Method
Participants
A quantitative, case-controlled, experimental design was used. The sample (n = 320) was divided equally in terms of gender (160 boys and 160 girls). Learners from grades 1 to 7, between the ages of 6 and 14 years, were recruited from six schools in the Moletjie area of Limpopo Province, South Africa. The participants were divided into three age groups: 6–8, 9–11, and 12–14 years. The sample was chosen because of its accessibility. To detect symptoms of ADHD, the learners were screened using the Disruptive Behavioural Disorder (DBD) rating scale, based on ratings from parents as well as teachers (Pelham, Gnagy, Greenslade, & Milich, 1992; Pillow, Pelham, Hoza, Molina, & Stultz, 1998).
Children were divided into an ADHD group and a control group, without ADHD symptoms. Cut-off points were based on the results obtained from a previous study that had been conducted in Limpopo by Meyer et al. (2004). Patients with a score of ⩾17 on the Hyperactivity/Impulsivity (HI) subscale were considered as ADHD-HI, while those with scores of ⩾20 on the Inattention subscale were regarded as ADHD-PI. When the criteria for both were met, the participants were considered as the ADHD-C subtype. The cut-off point was the 95th percentile, which is regarded to be clinically significant (Barkley & Murphy, 1998). Scores of less than 15 on the HI and Inattentive subscales were criteria for inclusion in the control group. For the control group, the cut-off point was set as the 85th percentile or less, to reduce the likelihood of false positives being included in this group. The researchers confirmed the diagnosis.
Children who are suffering from cerebral palsy, epilepsy, any head injury, or severe psychiatric disorders, as reported on the demographic questionnaire by the parents, were excluded from this study. At the time of testing, the researcher ensured that none of the children were taking psychostimulant medication.
Instruments
The DBD rating scale, which was used for ADHD screening, was completed separately by parents and teachers (Pelham et al., 1992; Pillow et al., 1998). The scale was standardised for all language and population groups in the Limpopo Province, South Africa (Meyer et al., 2004). The DBD assessed the degree of ADHD-related symptoms and included hyperactivity/impulsiveness and inattention, oppositional defiant disorder, and conduct disorder symptoms (McClelland et al., 2007). The 42 items included on the DBD scale are based on the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) diagnostic criteria (American Psychiatric Association, 2000). Only the 18 items that measure ADHD were selected. The items were rated on a 4-point scale: 0 (not at all), 1 (just a little), 2 (pretty much), and 3 (very much). Cronbach α for the Limpopo province was calculated at .90 for the HI scale and .92 for the Inattention scale (Meyer et al., 2004). In this study, the sample’s Cronbach α for the HI scale was calculated at .74, and at .79 for the Inattention scale.
Assessment of executive functions
The Tower of London (ToL) was used to assess planning behaviour (Shallice, 1982). It is a well-known neuropsychological test, customarily used to assess EFs, and specifically to detect deficits in planning (Luciana, Collins, Olson, & Schissel, 2009; Riccio, Wolfe, Romine, Davis, & Sullivan, 2004). The apparatus consisted of three wooden pegs of various lengths, mounted on a strip of wood where three different coloured wooden beads (red, yellow, and blue) had been placed. The researcher presented an example of the problems, on cards, which were to be solved in two to five steps. In a practice problem, the same initial position was used, where two steps were needed to reach a solution. The task consisted of 12 problems, which had been graded in terms of their difficulty. From the start position, the participants were expected to move the beads to the finish position shown on the cards, making use of the least number of steps. Reliability coefficients were split-half reliability, r = .72, and internal consistency, Cronbach α = .69 (Kaller et al., 2015; Kaller, Unterrainer, & Stahl, 2012).
The NEPSY-II (Developmental Neuropsychological Assessment, second edition) Inhibition subtest is used to assess various aspects of EFs, including inhibitory control, cognitive flexibility, and self-monitoring (Korkman, Kirk, & Kemp, 2007). This timed subtest is designed to assess the ability to inhibit automatic responses in favour of original responses, as well as the ability to switch between response types. The subject looks at a series of black and white shapes or arrows and names the shape or direction, or provides an alternate response, depending on the colour of the shape or arrow. According to Korkman et al. (2007), the Inhibition subtest shows appropriate and adequate to high internal consistency. The test–retest reliability average for inhibition combined with switching was between .73 and .87 for ages 12–16 years.
Procedure
The procedure was explained to the children. The assessment was conducted during school hours at the participants’ respective schools. First, the ToL was administered, followed by the NEPSY-II Inhibition subtest. The testing procedure for each child lasted 30 min and was conducted by a clinical psychologist, assisted by five research assistants, all of whom had achieved a bachelor’s degree in psychology and were fluent in the home language of the child.
Ethical considerations
The study obtained ethical approval from the Biomedical Research Ethics Committee of the University of KwaZulu-Natal (reference number HSS/0702/015D). The Department of Education provided permission for the study to be conducted at the participating schools, and consent was obtained from the relevant school principals. Written consent was obtained from the parents of the children, and the children signed assent forms; they were also told that their participation was voluntary and that they could withdraw at any stage.
Data analysis
STATISTICA-10 (StatSoft, Inc., 2011) was used to analyse the data. The analysis of variance (ANOVA) method was utilised to investigate the possible group differences on the ToL and NEPSY-II Inhibition subtest performances. The two-way ANOVA compares the mean difference between groups that have been split on two or more independent variables. The primary purpose is to understand if there is an interaction between the two independent variables on the dependent variables. The study used a 4 × 2 × 3 (ADHD-presentation × gender × age group) ANOVA to analyse the results of independent samples. The Bonferroni test was used to conduct post hoc comparisons. To examine whether the two domains of EFs were distinctive or reflected a common process, Pearson’s correlation coefficients were calculated. All the participants were treated as a single group.
Results
The study hypothesised that the three ADHD subtypes (ADHD-HI, ADHD-PI, and ADHD-C) would perform more poorly on behavioural planning and response inhibition than the control group and that the performance with regard to the tasks would differ for the three subtypes. In addition, we sought to determine whether behaviour planning and response inhibition were distinct or related processes. The demographics and DBD scores for the sample are presented in Table 1.
Demographic and ADHD characteristics of the sample.
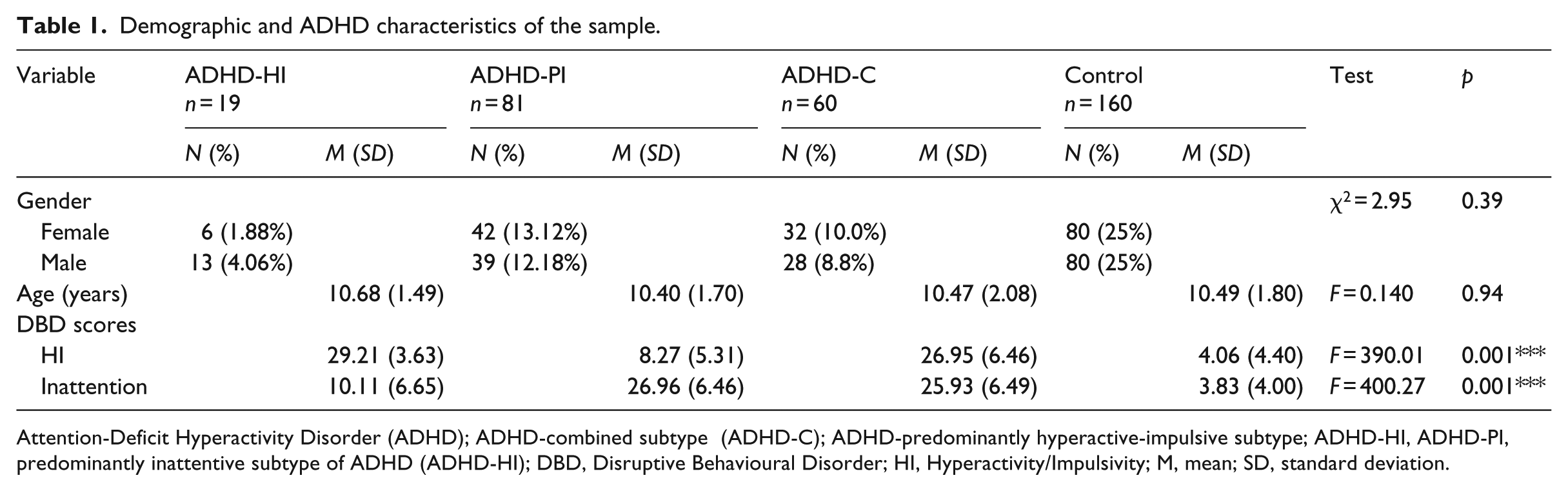
Attention-Deficit Hyperactivity Disorder (ADHD); ADHD-combined subtype (ADHD-C); ADHD-predominantly hyperactive-impulsive subtype; ADHD-HI, ADHD-PI, predominantly inattentive subtype of ADHD (ADHD-HI); DBD, Disruptive Behavioural Disorder; HI, Hyperactivity/Impulsivity; M, mean; SD, standard deviation.
The descriptive statistics, the results of the ANOVA, and the post hoc test scores for both the ToL and the NEPSY-II Inhibition subtest are shown in Table 2.
Means, standard deviations, and ANOVA for the ADHD subtypes and control groups.
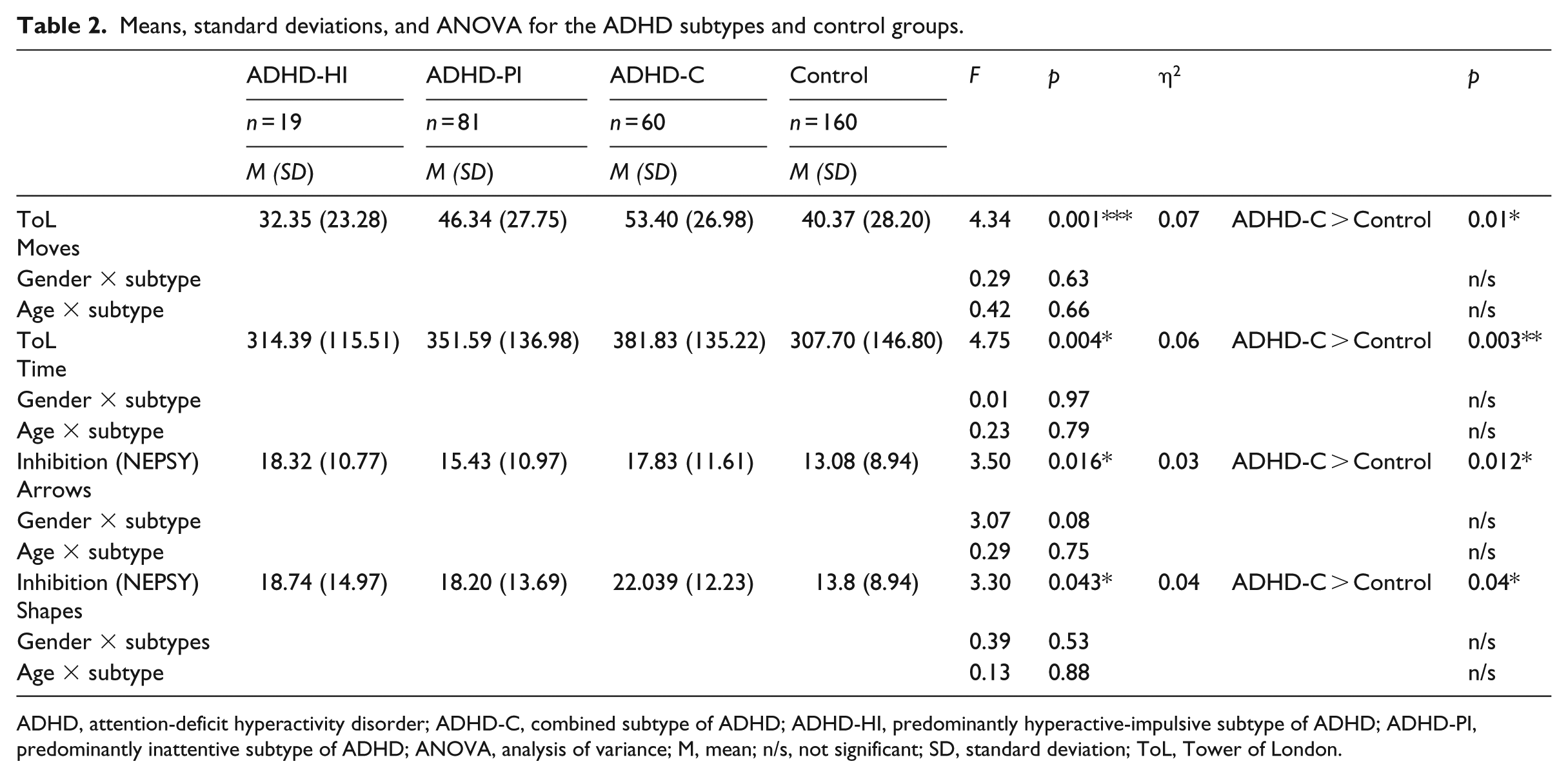
ADHD, attention-deficit hyperactivity disorder; ADHD-C, combined subtype of ADHD; ADHD-HI, predominantly hyperactive-impulsive subtype of ADHD; ADHD-PI, predominantly inattentive subtype of ADHD; ANOVA, analysis of variance; M, mean; n/s, not significant; SD, standard deviation; ToL, Tower of London.
For the ToL (moves), the ANOVA showed a main effect of subtype: F (3, 312) = 4.34, p < .001, η2 = 0.07, and for time taken: F (3, 312) = 4.75, p = .004, η2 = 0.06. The effect sizes for the moves (η2 = 0.07) and the time taken (η2 = 0.04) were small. The ANOVA revealed no main or interacting effects of age and gender. Hence, the gender and age groups were not analysed separately.
The interaction effect for gender × subtype for moves was F (1, 312) = 0.29, p = .63, for age and subtype: F (1, 312) = 0.42, p = .66, and for time taken, gender and subtype: F (1, 312) = 0.01, p = .97 and age and subtype: F (2, 308) = 0.23, p = .79. The Bonferroni test revealed a statistically significant difference between the ADHD-C subtype group and controls, both for moves (p = .001) and for the time taken (p = .003). The ADHD-C group used significantly more moves and took significantly more time to complete the task than the neurotypical control group. There were no significant differences in the performance between ADHD-HI and ADHD-PI subtypes and the control group for either moves or time taken.
The ANOVA results for the NEPSY-II Inhibition subtest (arrows) also indicated a main effect of ADHD subtype: F (3, 312) = 3.50, p = .016, η2 = 0.03, but there were no main effects for gender and age, and also no interaction between gender and subtype: F (1, 312) = 3.07, p = .08, and age and subtype: F (2, 308) = 0.29, p = .75. On the NEPSY (shapes) there was also a main effect for subtype: F (3, 312) = 3.30, p = .043, η2 = 0.04, but no interaction between gender and subtype: F (1, 312) = 0.39, p = .53 or age and subtype: F (2, 308) = 0.13, p = .88. Therefore, the age and gender groups were not analysed separately. The effect sizes were small both for arrows (η2 = 0.03) and shapes (η2 = 0.04). Post hoc analysis (Bonferroni correction) revealed significant differences between the ADHD-C group and the control group, for both arrows and shapes. No statistically significant differences were found for the performance of the Inhibition subtest (arrows and shapes) between the ADHD-HI and ADHD-PI subtypes and the control group.
The results of the correlation scores for the ToL and the NEPSY-II Inhibition subtest are shown in Table 3. Results show that the correlations were significant but weak (r = .13–.25).
Correlations between the EF tests: ToL and NEPSY-II Inhibition subtest.
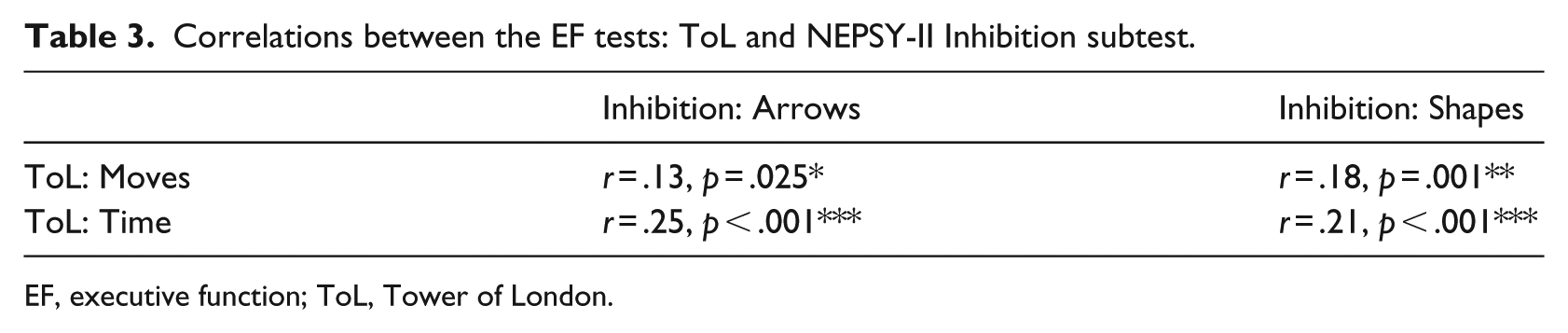
EF, executive function; ToL, Tower of London.
Discussion
The study examined two domains of EFs in Sepedi-speaking primary school children with ADHD, to determine whether there were deficits in behaviour planning and response inhibition. The results of the study support the view that children with ADHD-C show more impairment in both behaviour planning and response inhibition when compared to children without ADHD.
The ADHD-C subtype’s poor performance on the ToL indicated that children with symptoms of both HI and inattention experience planning deficits, and they struggle to perform tasks and select strategies that entail reasoning. The findings were consistent with the study conducted by Sarkis, Sarkis, Marshall, and Archer (2005), who found that the ADHD-C subtype performed significantly worse than the non-ADHD groups on the ToL. Children with symptoms of both inattention and HI were more severely impaired than those with ADHD-HI and ADHD-PI only because they have difficulty sustaining attention and respond impulsively, whereas the other subtypes are only affected in one domain. Similarly, Pila-Nemutandani and Meyer (2016) and Schmitz et al. (2002) noticed that children with the ADHD-C subtype were highly deficient in behavioural planning and faced more difficulties when compared to both the ADHD-HI and ADHD-PI subtype and the control group of non-ADHD children.
Children with ADHD-C struggle to remember instructions and to plan new strategies in a different situation (Saydam, Ayvasik, & Alyanak, 2015). A study by Geurts et al. (2005), however, showed no deficiencies in children with ADHD-C on the ToL. The incongruencies between the Geurts et al. (2005) study and the findings of this study may be because of a smaller sample that they used. Nonetheless, Geurts et al.’s (2005) observation do not shift the common view that children with ADHD-C are more impaired in planning behaviour than control groups, or the ADHD-PI and ADHD-HI presentations (Nigg et al., 2002; Pila-Nemutandani & Meyer, 2016; Solanto et al., 2007). Saydam et al. (2015) further support the notion that ADHD-C children are more impaired in their planning ability than those with ADHD-PI.
These suggest that the poor performance on the ToL by children with ADHD-C was a result of their rapid implementation of solutions that had not been well thought out. Children with ADHD-C had problems carrying out tasks to their conclusion and paying attention to instructions, and they were quick and disorderly when they planned their tasks. It follows, then, that children of the ADHD-C subtype have a compromised learning ability at school, which makes it difficult for them to apply new skills. The mechanism underlying planning deficits in children with similarly poor skills or abilities are associated with frontal lobe dysfunction, which arises from the hypofunctioning of the mesocortical dopaminergic branch, which also causes symptoms of ADHD (Kofman et al., 2008).
In terms of the inhibition task, the results of this study were similar to those of other researchers, who had also found that children of the ADHD-C subtype displayed more impairment in inhibition tests, not only when compared with a neurotypical control group, but also when compared with the ADHD-PI subtype (Semrud-Clikeman, Walkowiak, Wilkinson, & Butcher, 2010; Skogli, Egeland, Andersen, Hovik, & Øie, 2014). According to Sergeant, Geurts, and Oosterlaan (2002), children with ADHD-C have deficits in the inhibition of a prepotent response (a reaction that is greater to other potential responses). However, Song and Hakoda found that both ADHD-PI and ADHD-C children showed deficits in response inhibition (Song & Hakoda, 2011).
The HI symptoms worsen the deficits in inhibition control. Impairment in inhibition involves both inattention symptoms, and impulsiveness and hyperactivity. The PFC dysfunction observed in children with ADHD means that they are both easily distracted and fail to focus. There is impairment in their filtering of sensory stimuli, and they are more vulnerable to interference or disruptions (Arnsten & Li, 2005).
Contrary to our findings, Chhabildas et al. (2001) demonstrated that the inattention symptoms accounted for deficits in response inhibition in ADHD. However, the small effect sizes of the Chhabildas et al. (2001) study suggest that some clear and prominent distinctions are present, but, simultaneously, there are some indirect differences between the two subtypes for ADHD. There is a need for future research to focus on these differences.
It was also demonstrated in the findings that children with ADHD-C were observed to respond much more slowly to the tasks allocated to them. These indicate a processing deficit, which involves the alternative responses rearrangement, following the ongoing actions for inhibition. This deficit for inhibition control in children with the ADHD-C subtype often acts as a contributing factor to their apparent inattentiveness in circumstances, which require a quicker and faster shift of attention from one response to another, as demanded by the situation (Nikolas & Nigg, 2013).
Finally, the low correlations shown between planning and inhibition tasks in this study, as well as in other studies (Olson, Schilling, & Bates, 1999; Scheres et al., 2004), suggest that planning and inhibition are distinct processes. The ToL and NEPSY-II Inhibition subtest is useful in identifying planning or inhibition deficits, also in non-Western populations.
It is essential that teachers recognise children with ADHD early so that they can provide appropriate and effective intervention. Early referrals ensure that children with ADHD can receive the appropriate assessments and necessary follow-up treatments at an early age (Subcommittee on Attention-Deficit/Hyperactivity Disorder et al., 2011). An early intervention means that clinicians can implement an appropriate strategy to eliminate misdiagnosis, reduce the impact of the disorder, prevent unnecessary suffering, and promote healthy development. In this regard, early pharmacological and/or behavioural treatment should be provided when applicable.
The sample used in this study was homogeneous: All the children were Sepedi speaking and from the same geographical area. Consequently, the results cannot be generalised to the rest of the country. The study has yet another limitation since tests were used for the assessment of only two of the domains of EFs – the inhibition and planning aspects. For future studies, there is a need for assessment of other EF areas, including working memory, cognitive flexibility, and attention control.
Conclusion
We found that children with ADHD-C exhibit deficits in planning and inhibition control. Our results for the ToL suggest that children with the ADHD-C subtype demonstrate severe deficits in planning and have difficulty with problem-solving. Poor response inhibition was also evident in the ADHD-C subtype, which indicates that the children experienced difficulty suppressing interfering stimuli and focusing on the stimulus of choice. Their inability to exercise inhibitory control compromises their learning (Diamond, 2013). Both the ToL test and the NEPSY-II Inhibition subtest can be used to detect behavioural planning and response inhibition in children with ADHD in a clinical setting, although they measure different domains and therefore can be used independently.
Footnotes
Declaration of conflicting interests
It is hereby declared by the authors that there has been no involvement of any other person in this research, neither has there been the incentive of any financial or other advantages which may have influenced the outcomes of the study, both while the data were being collected or when the research document was being written.
Funding
The College of Health Sciences Research Office at the University of KwaZulu-Natal provided the funds required to enable this study to be conducted.