
Abstract
Universities in South Africa face ongoing challenges with low rates of academic attainment and high rates of attrition. Our aims were to (1) investigate the extent to which common mental disorders evaluated early in the first year predict academic failure at the end of the year, controlling for sociodemographic factors and (2) establish the potential reduction in prevalence of failure that could be achieved by effectively treating associated mental disorders. Self-report data were collected from first-year students (n = 1402) via an online survey at the end of the first semester. Participants were assessed for six common mental disorders. Academic performance data were subsequently obtained from institutional records at the end of the year. Bivariate and multivariate logistic regression models were used to identify the best sociodemographic and mental health predictors of academic failure. Population attributable risk analysis was used to assess the potential impact of treating associated mental disorders. In multivariate logistic regression models controlling for significant sociodemographic factors, the odds of failure were elevated among students with major depressive disorder (aOR = 3.69) and attention deficit hyperactivity disorder (aOR = 2.05). Population attributable risk analysis suggests that providing effective treatment to students with major depressive disorder and/or attention deficit hyperactivity disorder could yield a 6.5% absolute reduction in prevalence of academic failure (equivalent to a 23.0% proportional reduction in prevalence of academic failure). Providing effective and accessible campus-based mental healthcare services is integral to supporting students’ academic attainment and promoting transformation at South African universities.
Universities in South Africa (SA) face a number of challenges, not least of which is the need to improve access for historically marginalised groups and increase the rate of educational attainment for all students (Badat & Sayed, 2014; Moodley & Singh, 2015). Post-secondary educational attainment rates have traditionally been very low on the African continent, even though tertiary education is understood to be a key force for modernisation, development, and social justice (Bloom et al., 2006; Darling-Hammond, 2015; Teferra & Altbachl, 2004). In SA, 25%–30% of students drop out in their first year of study and a further 20%–30% drop out in the second or third years, with an overall graduation rate of 15% across all universities (Letseka et al., 2010; Letseka & Maile, 2008; Murray, 2014). It is estimated that only 24% of SA graduates complete their degrees within the minimum prescribed number of years (Council for Higher Education, 2016). These high dropout rates have focused attention on the need for effective early identification and intervention programmes, particularly among first-year students (Moodley & Singh, 2015). Promoting academic retention and attainment is integral to achieving socio-political justice, transformation, and economic development in SA. Yet, much of the literature on predictors of university academic performance comes from high-income, Western countries, and most of the studies in this area have focused on sociodemographic determinants of performance rather than mental health (De Clercq et al., 2013; Richardson et al., 2012). The aim of this study was to investigate the extent to which common mental disorders (CMDs) evaluated early in the first year predict academic failure at the end of the year, when controlling for sociodemographic factors. We also wanted to establish the potential reduction in prevalence of academic failure that could be achieved by effectively treating the associated CMDs among students in SA. This research was undertaken as part of the ongoing work of the World Health Organization (WHO) World Mental Health Surveys International College Student Initiative (Cuijpers et al., 2019).
The majority of studies on academic performance among university students come from North America, Canada, and Europe (Richardson et al., 2012). Furthermore, many of the studies in this field use subjective (self-report) assessments of academic performance and focus on single determinants (such as ethnicity or gender) or a very limited number of factors, thus ignoring complexity and the potential influence of multiple-factors and possible interactions (Richardson et al., 2012). Two exceptions are the work of De Clercq et al. (2013) and Jia and Maloney (2015), which showed how socioeconomic variables interact with demographic factors to shape academic success (De Clercq et al., 2013; Jia & Maloney, 2015).
Academic performance is consistently associated with sociodemographic factors, including socioeconomic status (SES), parents’ level of education, ethnicity, and gender. Students from families of low SES and those with parents who have lower levels of education are more likely than their peers to fail and dropout of university (Stratton et al., 2007). While ethnicity appears to be an important determinant of academic success, evidence suggests that ethnicity interacts with other variables, such as gender and SES, to increase risk of failure (De Clercq et al., 2013; Murray, 2014). For example, ethnic minority students in the United States are more likely than other groups of students to have lower academic attainment rates, take longer to graduate, and have higher rates of attrition compared with students who are part of the ethnic majority, although these disparities are even more marked for male students (Strayhorn, 2014).
Evidence regarding the influence of gender on academic failure and attrition is mixed. Stratton et al. (2007) found that being female increased the probability of attrition, whereas Jia and Maloney (2015) found that females have a higher probability of completing university compared with males. Murray (2014) found that male SA university students were more likely to succumb to involuntary attrition, and dropped out sooner than their female peers (Murray, 2014).
There is a small body of literature on associations between mental health and academic performance (Bruffaerts et al., 2019; Gormley et al., 2016; Richardson et al., 2012; Stratton et al., 2007; Wintre et al., 2011). Poor academic performance is consistently associated with attention deficit hyperactivity disorder (ADHD; Gormley et al., 2016), symptoms of depression (Wintre et al., 2011), substance use and alcohol dependency (Aertgeerts & Buntinx, 2002), and frequency of binge drinking (Piazza-Gardner et al., 2016). Most studies investigating the influence of psychopathology on academic performance have focused narrowly on one form of psychopathology (e.g., depressive illnesses) and have assessed symptoms of psychopathology rather than screening for students who are likely to meet the diagnostic criteria for a mental disorder (De Clercq et al., 2013; Gormley et al., 2016; Richardson et al., 2012). The existing literature has largely failed to explore issues such as the cumulative effect of having more than one mental disorder, potential interactions between different psychological disorders, and how sociodemographic factors may increase vulnerability to academic failure among students with psychopathology (Richardson et al., 2012). A notable exception to this is a study of first-year students in Belgium (n = 4921), which reported that students with mental health problems have significantly lower academic functioning than other students, leading the authors to advocate for campus-based mental health interventions as an integral component of promoting educational attainment (Bruffaerts et al., 2019).
Data suggest that rates of psychopathology among SA university students are higher than those observed in the general population (Bantjes, Breet, et al., 2019; Bantjes, Lochner, et al., 2019). Yet, the impact of CMDs on the academic performance of SA university students remains largely un-investigated. Furthermore, it is not clear how the prevalence of academic failure might be reduced if effective campus-based treatments were offered for CMDs which compromise academic performance.
Method
The aims of this study were to (1) investigate the extent to which CMDs evaluated early in the first year predict academic failure at the end of the year, when controlling for sociodemographic factors and (2) establish the potential reduction in prevalence of academic failure that could be achieved by effectively treating the CMDs associated with academic failure.
Participants
All first-year students (i.e., students registering for the first time at university) at Stellenbosch University in 2015 and 2017, and the University of Cape Town in 2017 were invited via email to participate in an anonymous online survey. A total of 1402 students completed the survey (participation rate = 9.7%).
Instruments
The following data were collected via an online survey in English.
Sociodemographic characteristics: Participants provided information about their parents’ level of education, whether they had a serious physical impairment (e.g., vision, hearing, or movement impairment), and whether they suffered from any chronic illnesses (e.g., asthma, diabetes, migraine, or chronic pain disorder). They were asked how they identified in terms of gender and sexual orientation. In addition, participants were also asked how they self-identify in terms of Black-African, Coloured, Asian, White, and Other. We used these terms given that they continue to be broadly used to report census data in the country as well as in contemporary legislation and discourse about transformation of universities. Participants were identified as ‘first-generation students’ (if neither of their parents had completed tertiary education) or ‘second-generation students’ (if either of their parents had a tertiary education). Participants were identified as having a disability if they reported any serious physical impairment or chronic health problem. Gender was coded as ‘male’ or ‘female’; students who identified as gender non-conforming were omitted from the analysis because this subgroup was too small to allow meaningful analysis. Following the APA style guidelines, sexual orientation was coded as ‘heterosexual’ (i.e., no same sex attraction) or ‘sexual minority groups’ (i.e., lesbian, gay, bisexual, asexual, or questioning). Students who self-identified as Black-African, Coloured, or Asian were coded as Black. This broad definition of Black was used to identify all students in groups which have been historically excluded from universities in SA. In using this classification, our intention was to explore the possibility of ongoing social and political inequality in access to education and economic opportunities as a result of apartheid; our use of these terms was not intended to reify sociocultural constructs about ancestry or to imply that such categories have a biological or scientific basis.
CMDs: We assessed the 12-month prevalence of major depressive disorder (MDD), generalised anxiety disorder (GAD), bipolar spectrum disorder, alcohol use disorder (AUD), drug use disorder (DUD), and ADHD using items adapted from the Composite International Diagnostic Interview (CIDI) used in the World Mental Health Surveys (Ronald C. Kessler & Üstün, 2004), EPI-Q Screening Survey (R. C. Kessler et al., 2013), Alcohol Use Disorders Identification Test (Saunders et al., 1993), and The World Health Organization Adult ADHD Self-Report Scale (ASRS; R. C. Kessler et al., 2005). Caseness was determined using the procedure validated in the Army Study to Assess Risk and Resilience in Service Members (Heeringa et al., 2013), and replicated in the WHO World Mental Health Surveys (Ronald C. Kessler & Üstün, 2004),. These instruments and procedures were used to ensure that our data collection methods were aligned with the procedures used in the World Mental Health Surveys (Ronald C. Kessler & Üstün, 2004), thus enabling meaningful comparisons with existing international psychiatric epidemiological data for university students (Auerbach, Mortier, Bruffaerts, Alonso, Benjet, Cuijpers, Demyttenaere, Ebert, Green, Hasking, Murray, et al., 2018). These instruments have been widely used in diverse cultural settings and have been shown to be reliable and valid for assessing CMDs (Ronald C. Kessler & Üstün, 2004).
Academic failure: We used official university records to identify all participants who did not proceed to the second year of academic study (which we defined as academic failure), either because they did not earn sufficient credit to progress to the second year or because of attrition. Students who only failed one or two modules, but who proceeded to second year were not identified as having failed, since this subgroup of students were still on track to complete their degrees in the allotted time.
Procedure
Participants were invited to complete an online survey in the first half of the academic year to assess their mental health. At the end of the academic year we obtained data directly from the university about the academic performance of participants.
Ethical considerations
Ethical approval was obtained from the Health Sciences Research Ethics Committees at Stellenbosch University and the University of Cape Town. Institutional permission was also obtained from the relevant university authorities. Participation in the study was voluntary and informed consent was obtained from all respondent’s prior to data collection. All data were securely stored on password-protected computers. Information about counselling and crises services was provided to all participants. Once we had obtained information about academic failure, all data were de-identified to protect participants’ privacy.
Data analysis
Data were cleaned, checked, and imported into SPSS 25 for analysis. A post-stratification weighting technique was used to weight all the data by gender and self-identified ‘race’ (Holt & Smith, 1979) (i.e., the data analysed were statistically adjusted to reflect the demographic composition of the two universities and to compensate for the bias that resulted from oversampling students who identified as female or White). Bivariate and multivariate logistic regression models were used to identify the sociodemographic and mental health predictors of academic failure. We examined both main effects and all possible two-way interactions between predictors. The results of all logistic regression analysis are reported as adjusted odds ratios (aOR) with associated 95% confidence intervals (95% CI). The significance level was set at alpha = .05. Finally, we conducted a population attributable risk (PAR) analysis, to establish the potential reduction in prevalence of academic failure that could be achieved by effectively treating CMDs associated with academic failure, assuming that CMDs cause academic failure.
Results
The majority of the sample were second-generation students (80.3%), and identified as female (55.2%), White (58.6%), heterosexual (77.8%), and able-bodied (81.6%). A total of 42.7% of participants reported a CMD in the past 12 months, namely MDD (13.6%), GAD (20.8%), bipolar spectrum disorder (1.0%), AUD (5.6%), DUD (3.1%), and ADHD (25.9%). The prevalence of academic failure in the sample was 26.2%.
Sociodemographic predictors of academic failure
In the first step of the analysis we explored associations between sociodemographic variables and academic failure, to identify sociodemographic factors which best predicted academic failure. We used bivariate and multivariate regression analysis to investigate all main effects and all 2×2 interaction effects (detailed results of this analysis are available from the authors as supplementary materials). A significant interaction was observed between identifying as Black and first-generation status. Academic failure among second-generation students who responded to the survey was associated with male gender (aOR = 1.43) and identifying as Black (aOR = 1.64), but not with sexual orientation or disability status. By comparison, academic failure among first-generation students was not associated with any other sociodemographic variables. On the basis of this analysis, we estimated a multivariate regression model of the effects on academic failure of all possible 2×2 combinations of identifying as Black and first-generation status, controlling for gender (Table 1). Academic failure among students who responded to the survey was significantly associated with being a first-generation White student (aOR = 4.68), being a first-generation Black student (aOR = 2.63), and being a second-generation Black student (aOR = 1.63).
Multivariate analysis of gender and all possible 2×2 combinations of population group and first-generation status as predictors of academic failure among first-year university students in SA (n = 1402).
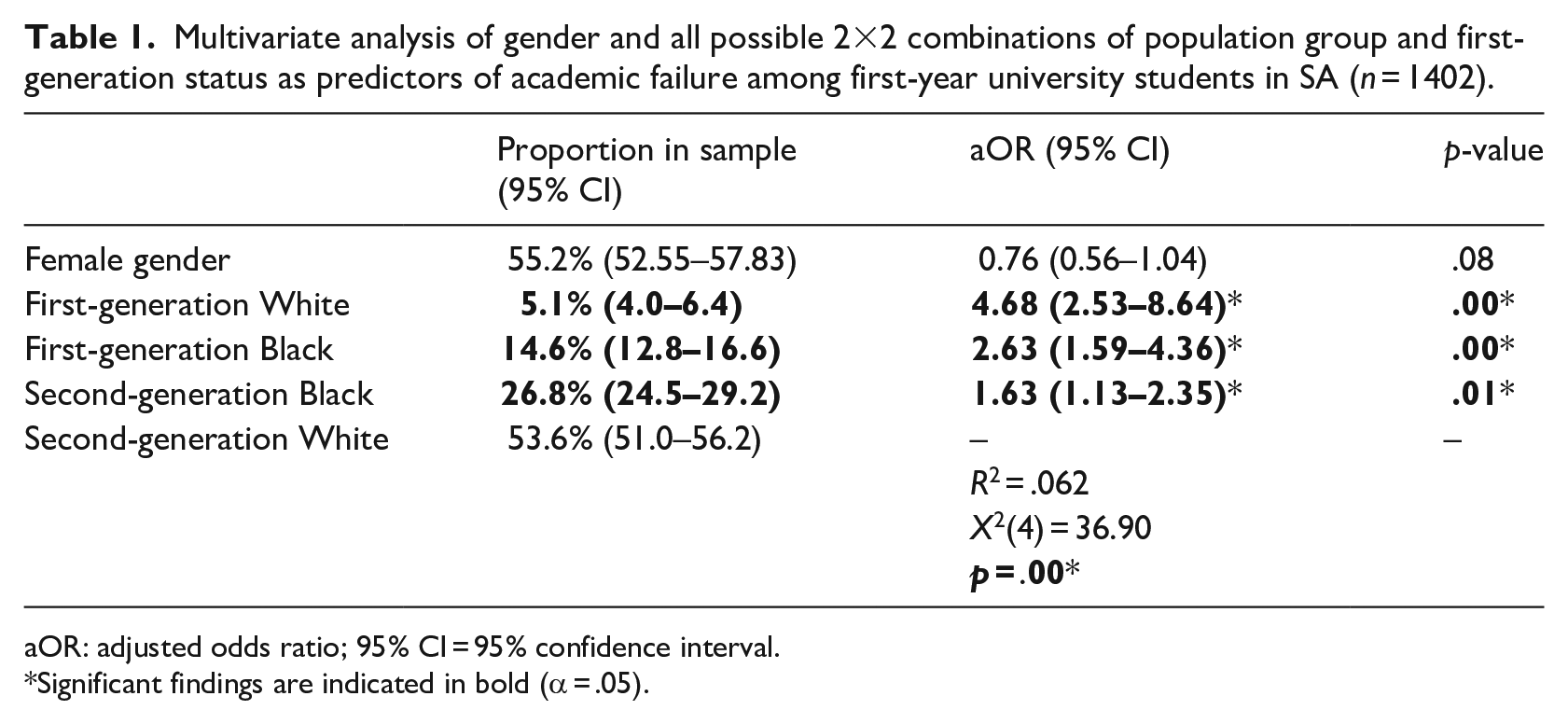
aOR: adjusted odds ratio; 95% CI = 95% confidence interval.
Significant findings are indicated in bold (α = .05).
CMDs as predictors of academic failure
In bivariate analysis, academic failure was independently associated with MDD (OR = 2.90) and with ADHD (OR = 1.95), but not with GAD, bipolar spectrum disorder, AUD, or DUD (detailed results of this analysis are available from the authors as supplementary materials). Table 2 shows the results of the multivariate regression analysis of CMDs as predictors of academic failure, controlling for comorbidity. In this model, academic failure was associated with MDD (aOR = 3.69) and ADHD (aOR = 2.05). The odds of academic failure among students who completed the survey increased with the number of CMDs.
Multivariate analysis of current common mental disorders as predictors of academic failure among first-year university students in SA, controlling for comorbidity (n = 1402).
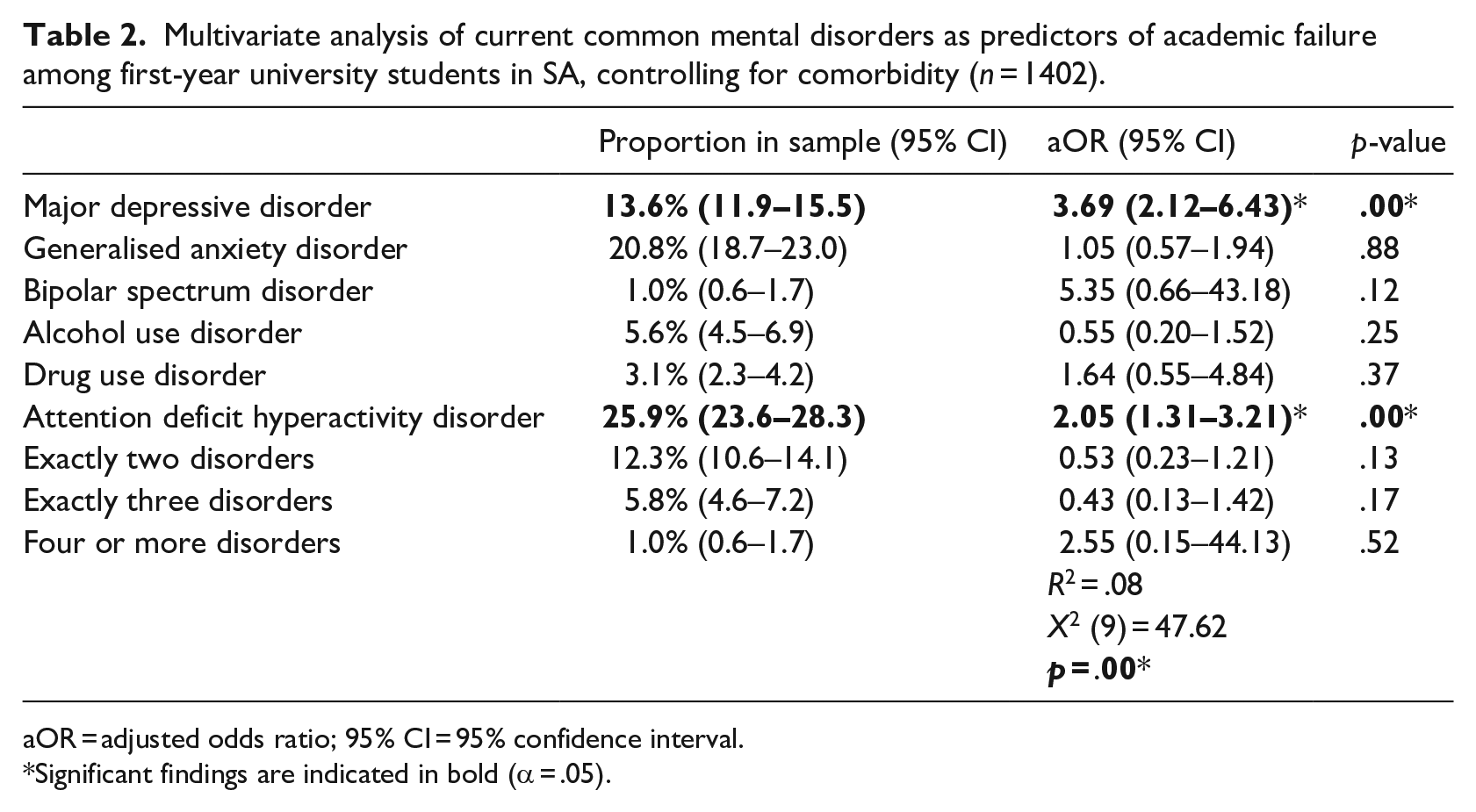
aOR = adjusted odds ratio; 95% CI = 95% confidence interval.
Significant findings are indicated in bold (α = .05).
Sociodemographic and CMDs as predictors of academic failure
We used multivariate regression analysis to investigate all main effects and 2×2 interaction effects between CMDs and sociodemographic variables as predictors of academic failure (detailed results of this analysis are available from the authors as supplementary materials). An interaction was observed between first-generation status and having MDD and/or ADHD. Among first-generation students the odds of academic failure were not increased by having MDD and/or ADHD (X2 = 1.66, OR = 1.61, 95% CI = 0.78–3.32, p = .098), while the odds of academic failure among second-generation students increased significantly if a student had MDD and/or ADHD (X2 = 32.64, OR = 2.75, 95% CI = 1.93–3.93, p = .00).
Given the results of the preceding analysis, we estimated multivariate regression models with gender, all 2×2 combinations of identifying as Black and first-generation status, and all 2×2 combinations of CMDs, to identify the best predictors of academic failure (detailed results available from the authors as supplementary materials). The best fitting model is presented in Table 3. In this model, academic failure among students who completed the survey was associated with identifying as male (aOR = 1.51), first-generation White (aOR = 4.22), first-generation Black (aOR = 2.54), second-generation Black (aOR = 1.55), and having MDD and/or ADHD (aOR = 2.61).
Multivariate regression model with gender, all 2×2 combinations of population group and first-generation status, and MDD and/or ADHD, as predictors of academic failure among first-year university students in SA (n = 1402).
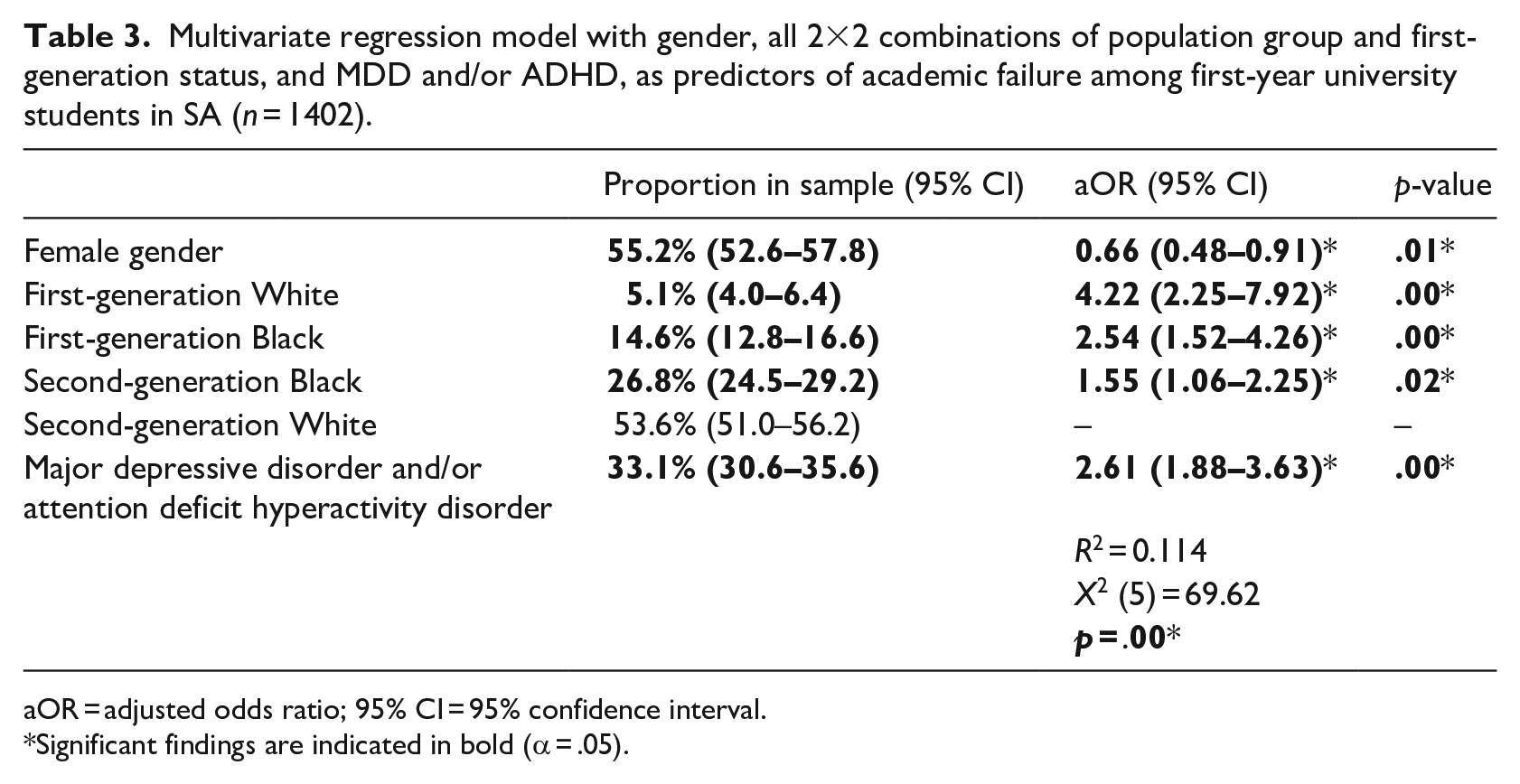
aOR = adjusted odds ratio; 95% CI = 95% confidence interval.
Significant findings are indicated in bold (α = .05).
PAR analysis
The beta coefficients of the model represented in Table 3 were used to calculate the predicted probability (PP) of failure for each participant given two different scenarios. In Scenario 1, PP was calculated as a function of all significant sociodemographic risk factors and ADHD and/or MDD. In Scenario 2, PP was calculated as a function of only sociodemographic risk factors. The mean PP for Scenarios 1 and 2 were 28.3% (95% CI = 27.4–29.3) and 21.8% (95% CI = 21.2–22.4), respectively. The results of this PAR analysis suggest that effectively treating MDD and ADHD could yield a 6.5% absolute reduction in prevalence of academic failure (equivalent to a 23.0% proportional reduction in prevalence of academic failure), assuming that CMDs are a causal factor in academic failure and that effective treatments would remove the elevated odds of failure observed among students with CMDs.
Discussion
The finding that 26.2% of our sample of first-year students failed to proceed to the second year of academic study, is congruent with previous reports of high rates of failure and attrition in SA universities (Letseka & Maile, 2008; Murray, 2014; Scott et al., 2007). This finding highlights the need to establish early identification and intervention programmes to support at-risk students. Furthermore, our data provide additional evidence that students from historically excluded groups continue to be at increased risk of academic failure in these two historically White universities despite improved access to higher education (Murray, 2014). Our data suggest that of the students who responded to our survey, first-generation students are at an elevated risk of academic failure, even when controlling for the effects of gender and mental health. The observed interaction between parents’ level of education and identifying as Black or White is significant and highlights the importance of considering intersectionality when identifying at-risk students. Our data suggest that being a first-generation student may be the best sociodemographic predictor of academic failure among first-year students in SA. As such, this subgroup of first-year students may require particular assistance when entering tertiary education.
It is noteworthy that the proportion of students who reported symptoms of ADHD was markedly higher than the proportion with MDD or GAD. Typically in epidemiological studies of student mental health, depressive and anxiety disorders are the most common (Auerbach, Mortier, Bruffaerts, Alonso, Benjet, Cuijpers, Demyttenaere, Ebert, Green, Hasking, Lee, et al., 2018). There is, however, literature documenting the growing number of university students with attention difficulties and the associated academic and social problems (DuPau et al., 2018; Wolf et al., 2009). While our data do not allow us to account for the high prevalence of ADHD, our findings do highlight the need for subsequent research in this area to understand why attention difficulties may be so prevalent among first-year students in SA.
Our finding of a significant association between mental health and academic performance is consistent with the international research in this area (Bruffaerts et al., 2019; Gormley et al., 2016; Richardson et al., 2012; Stratton et al., 2007; Wintre et al., 2011). This is an important finding in the light of the emerging international research showing that approximately one-third of first-year students report a CMD in the preceding 12 months (Auerbach, Mortier, Bruffaerts, Alonso, Benjet, Cuijpers, Demyttenaere, Ebert, Green, Hasking, Lee, et al., 2018), yet only 25.3%–36.3% of these students receive treatment (Bantjes et al., 2020; Bruffaerts et al., 2019). Students in our sample with MDD and ADHD are approximately 3.7 and 2.1 times more likely than other students to fail or dropout, when controlling for the effects of other CMDs. Crucially, our data show that MDD and ADHD predict academic failure, even when controlling for sociodemographic variables. One possible explanation for the observed association is that the symptoms of MDD and ADHD cause first-year university students to fail. This interpretation is supported by research showing that depressive illnesses and attention difficulties are consistently associated with impairments in cognitive performance and executive function (Becker et al., 2018; Cheung et al., 2016; Cotrena et al., 2016; Peters et al., 2017). Our PAR analysis suggests that effectively treating MDD and ADHD could yield a 6.5% absolute reduction in prevalence of academic failure, assuming a causal link between these disorders and academic failure and assuming that these disorders can be effectively treated. This has potential policy implications, particularly given the evidence that effective treatments are available for both MDD and ADHD (Australian Psychological Society, 2018; Cuijpers et al., 2016; Newby et al., 2015).
The discussion in the preceding paragraph is premised on the assumption that MDD and ADHD cause academic failure, which may not be true. For example, it is possible that the observed associations between MDD and academic failure reflect the depressive symptoms that result during the first semester from students’ realisation of their academic inadequacy and impending academic failure, in which case treating MDD is likely to have little effect on academic outcome. It seems much more likely that there is a causal link between ADHD and academic outcome, which may not be easy to break. Students with ADHD typically have ineffective study habits which have become habitual over a number of years (Simon-Dack et al., 2016). Any intervention to treat ADHD would need to be augmented with behavioural interventions to improve study habits in order to mitigate the risk of academic failure (Gormley et al., 2018). Nonetheless, our data suggest that counsellors treating students with MDD and/or ADHD need to take account of the increased odds of failure in this population and incorporate academic support as an explicit goal of treatment. Targeted interventions for students with ADHD are also important to promote academic attainment, especially since this condition is likely to be largely undiagnosed and/or poorly managed among university students given the significant mental health treatment gap in the country as a whole (Herman et al., 2009) and at SA universities (Bantjes et al., 2020).
It is noteworthy that male first-year students were 1.5 times more likely to fail compared with females, even when controlling for the effects of other socioeconomic variables and CMDs. This finding is consistent with the literature describing a so-called ‘gender crisis’ in education and the concern that has been expressed about both the enrolment and attainment of males in higher education across the globe (Buchmann, 2016; Fortin et al., 2015). As universities in SA seek to achieve greater equality by supporting the educational attainment of female students and those who identify as Black, it will be important to remember that male students may also be at elevated risk of academic failure. Policies to promote academic attainment, which fail to consider the vulnerability of male students, are at risk of creating a new gender order in SA in which one kind of inequality is simply replaced by another.
There are several limitations to this study, including the fact that we relied on self-report measures of CMDs from a self-selected sample of students from two large, well-resourced, historically White institutions. It is also a limitation that data were only collected in English. This limits the generalisability of findings and highlights the need to replicate this work with larger and more representative samples at other institutions in SA. A further limitation of the study is the fact that for the purposes of our analysis, we grouped self-identified ‘Black-African’, ‘Coloured’ and ‘Asian’ students together and considered them as a single group of historically marginalised students. Grouping students in this way may obscure the ongoing disparities between these three subgroups as a result of unequal treatment during apartheid (Cheteni, 2019; Sherer, 2000). Nonetheless, this study is the first of its kind to provide insight into a wide range of sociodemographic and mental health factors associated with academic failure among first-year students in SA. As such, this is an important first step in highlighting associations between academic failure and interactions between sociodemographic factors and mental health among first-year university students.
Conclusion
Scholars have called attention to the crises in rates of educational attainment within SA universities (Moodley & Singh, 2015). Badat and Sayed (2014) have affirmed that ‘A failure to act now and with urgency to reform South Africa’s educational approach betrays constitutional ideals and leaves intact the systemic crisis of education that especially affects South Africa’s historically disadvantaged and marginalized peoples’ (p. 127). Our data draw attention to the importance of considering factors such as mental health, gender, and being a first-generation student, when seeking to understand the dynamics of academic attainment in SA. Crucially, our data suggest that integral to addressing this educational crisis is the need to consider students’ mental health and prioritise campus-based student health services.
Supplemental Material
Supplementary_Tables__20_Aug_2020_(1) – Supplemental material for Mental health and academic failure among first-year university students in South Africa
Supplemental material, Supplementary_Tables__20_Aug_2020_(1) for Mental health and academic failure among first-year university students in South Africa by Jason Bantjes, Wylene Saal, Franco Gericke, Christine Lochner, Janine Roos, Randy P Auerbach, Philippe Mortier, Ronny Bruffaerts, Ronald C Kessler and Dan Stein in South African Journal of Psychology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: This research was funded by the South African Medical Research Council (SAMRC) through its Division of Research Capacity Development under the MCSP (awarded to Jason Bantjes). The content hereof is the sole responsibility of the authors and does not necessarily represent the official views of the SAMRC.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.