
Abstract
South Africa has one of the highest prevalence rates globally for fetal alcohol spectrum disorders. Despite this, few interventions are routinely available for countering the adverse effects of perinatal drinking. The current study used the ADAPT-ITT framework to guide the development of a behavioral intervention with remote alcohol use monitoring and provision of financial incentives contingent on alcohol abstinence for people who are pregnant and postpartum. The study aims to maximize the intervention’s relevance, acceptance, and effectiveness in reducing alcohol use during pregnancy and lactation, ultimately improving maternal and infant health outcomes in South Africa. Thirty-two in-depth interviews with people who were pregnant and 16 key-informant interviews with clinic and community members were conducted to help inform the intervention. The adapted intervention was pretested with 20 people who were pregnant or breastfeeding, and additional feedback was obtained from the community collaborative board. While there was widespread support for the intervention elements, some concerns were raised, including perceived high street value of a monitoring device, access to mobile phones to use such a device, frequency of monitoring, cheating when using a remote monitoring device, devices being lost or stolen, and the sustainability of long-term monitoring. The adapted intervention combines alcohol monitoring-based contingency management with text-based health promotion and information on where to access services tailored to maternal populations ready for testing in feasibility and efficacy trials.
Background
South Africa has one of the highest rates of fetal alcohol spectrum disorders (FASDs) in the world (Adnams, 2017; Lange et al., 2017; Popova et al., 2017). Of 187 countries, South Africa’s reported rate of FASD was 111 per 1000 population, compared to the estimated global prevalence of 7.7 per 1000 population (Lange et al., 2017). In the Western Cape region, the observed FASD prevalence in some communities is even higher at 20%–28% (May et al., 2017), with high levels of drinking reported among people who are pregnant (Petersen Williams et al., 2013, 2020).
While the risk of FASD is directly associated with prenatal alcohol exposure, there is limited research on the direct impact of alcohol consumed by people who are breastfeeding on the baby’s growth and development. Recent evidence suggests that even among children unexposed to alcohol prenatally, those exposed to alcohol via breastfeeding had significantly poorer physical and neurocognitive development outcomes (Gibson & Porter, 2018; May et al., 2016). Therefore, support during pregnancy and lactation to reduce alcohol use is critical to ensure the healthy development of children. However, few interventions that are routinely implemented and go beyond general health promotion advice in South Africa address perinatal drinking to prevent adverse effects on maternal and infant outcomes.
Behavioral interventions with contingent incentives (i.e., contingency management [CM]) have been effective in reducing alcohol use in nonperinatal populations (Alessi & Petry, 2013; McDonell et al., 2017; Oluwoye et al., 2020). In addition, CM has successfully reduced prenatal cocaine, alcohol, and tobacco use (Higgins et al., 2012; Schottenfeld et al., 2011; Washio et al., 2017). However, use of contingent rewards requires frequent biochemical monitoring for abstinence verification. Mobile technology has been successfully incorporated to remotely monitor alcohol use with adults (Alessi et al., 2017; Alessi & Petry, 2013) and people who are pregnant (Washio et al., 2017), expanding the potential to deliver a CM intervention remotely. However, no adaptations have been made for maternal populations in the South African context.
The Women’s Health CoOp (WHC) is a woman-centered brief intervention focused on alcohol and other drug use, gender-based violence, and HIV/sexually transmitted infections based on empowerment theory. Its core components include health education and promotion messaging, skills building, and referral to services (Wechsberg et al., 2013, 2015, 2019). The WHC has been shown to be efficacious in reducing HIV risk among women who use alcohol and other drugs in South Africa (Wechsberg et al., 2013, 2019). Disseminating content on health promotion and referral to services by means of texting increases contact and has been shown to enhance self-efficacy for behavior change (Alessi & Petry, 2013; Rodgers et al., 2005).
This study investigated the use of mobile breathalyzer technology to remotely monitor maternal alcohol use in South Africa with contingency management and taken concepts from WHC for text-based health promotion and referrals to treatment and other health and social services. Interventions that combine these three elements hold promise for supporting the reduction of alcohol use during pregnancy and lactation (Skipper et al., 2014). However, there are no technology-based CM interventions available that account for the specific needs of pregnant and lactating people who use alcohol in the South African context. To address this gap, the current study describes the adaptation of a technology-based behavioral intervention with remote alcohol use monitoring and provision of financial incentives contingent on alcohol abstinence during pregnancy and lactation to incorporate text-based content on health promotion and referral to services.
The study aimed to enhance the relevance, acceptance, and effectiveness of an intervention designed to reduce alcohol use during pregnancy and lactation, thereby improving maternal and infant health outcomes in South Africa. To achieve this, the researchers used the ADAPT-ITT framework (Wingood & DiClemente, 2008), which helps adapt evidence-based interventions to new settings, populations, or contexts. This model is particularly useful for making interventions culturally and contextually appropriate, thereby increasing their likelihood of success. By engaging local communities and stakeholders, the intervention can be tailored to address the specific cultural, social, economic, and healthcare challenges faced by pregnant and lactating individuals in South Africa. This approach ensures the intervention is both acceptable and feasible, ultimately enhancing its impact on reducing alcohol use and improving health outcomes.
Methods
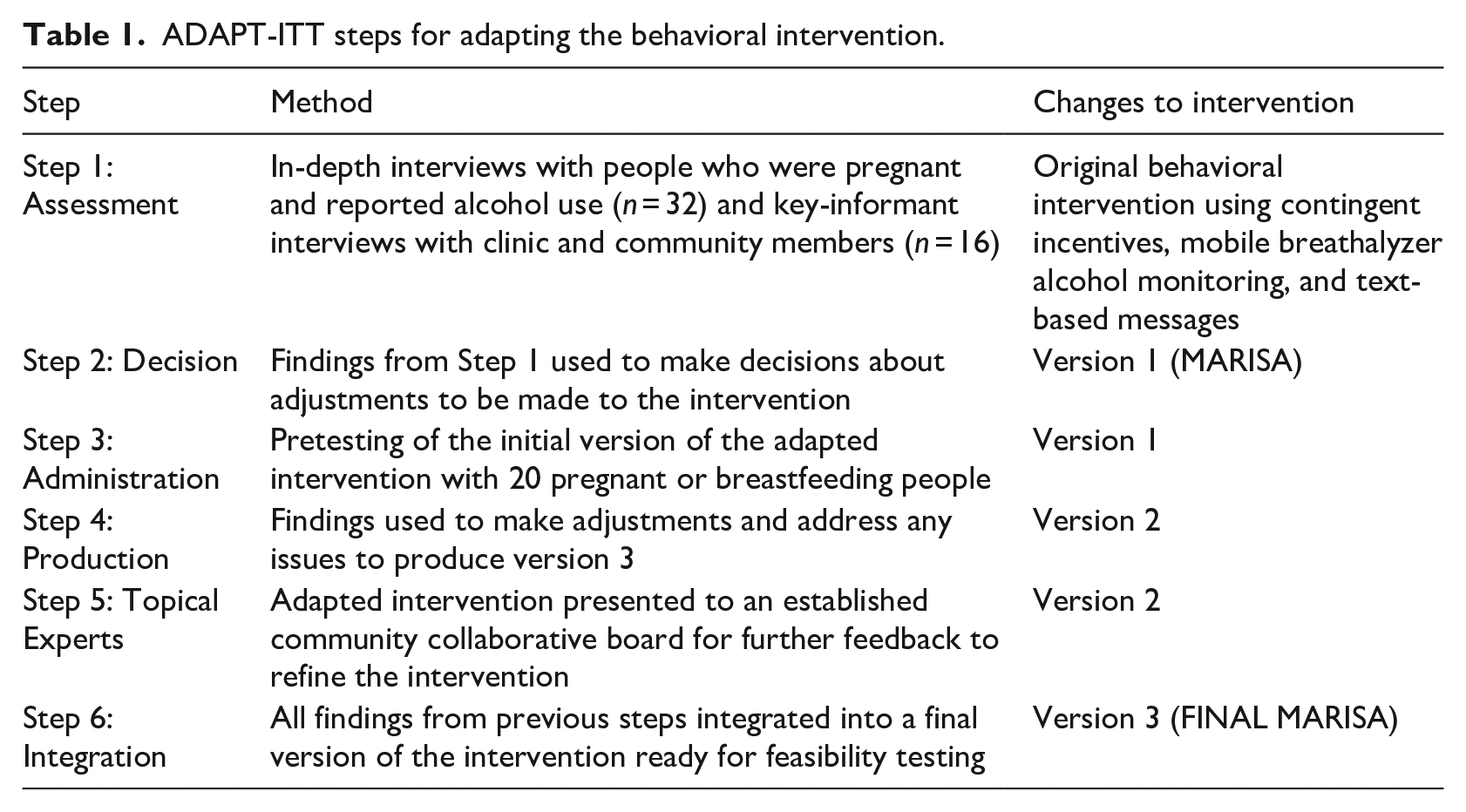
The ADAPT-ITT model consists of eight sequential phases that inform the adaptation of evidence-based HIV-prevention interventions and has been used successfully by our team with substance using populations in South Africa and elsewhere (Myers et al., 2018; Wechsberg et al., 2015). This study will focus on the first six steps of the framework: (a) assessment of pregnant and lactating people’s needs, (b) decisions about adjustments to be made to the intervention, (c) pretesting of the initial adaptation of the intervention with pregnant and breastfeeding people to make additional changes and increase acceptability, (d) production of the intervention after making adjustments, (e) presentation of the next version of the adapted intervention to topical experts for further input, and (f) integration of findings from previous steps into a final version of the intervention ready for feasibility testing. A description of the methods that we followed in each step of the adaptation is provided in Table 1.
ADAPT-ITT steps for adapting the behavioral intervention.
Participants and procedures
To explore treatment needs and feedback regarding the proposed intervention to adapt it to their context, we conducted in-depth interviews with people who reported alcohol use during the current pregnancy. Participants were recruited from several communities in the Cape Flats region of the Western Cape Province of South Africa. In addition, we conducted key-informant interviews (KIIs) with clinic and community members providing services to women, to explore their perceptions, experiences, and knowledge about perinatal alcohol use; breastfeeding while drinking; relevant health and psychosocial issues; necessary treatment and services to address these issues; and barriers to linking people to the required services. The findings from this formative research have been published elsewhere (Petersen Williams et al., 2024). For people who were pregnant and postpartum, community-based outreach techniques and snowball sampling were used to market the study and recruit participants. To be eligible, participants had to: (1) be 18 years of age or older, (2) be currently pregnant or delivered within the last 3 months, (3) report drinking during the current pregnancy or while breastfeeding, (4) have their own mobile phone, (5) intend to breastfeed for at least 6 months, (6) be able to participate in the interview in English, and (7) voluntarily consent to participate in the study. Clinic and community members were recruited through two Midwife Obstetric Units in Cape Town (providing antenatal services) and a community collaborative board our team has worked with in past studies. Prior to the interviews, participants were asked to provide informed consent. Interviews lasted up to 60 min and took place between July and November 2021. All interviews were audiorecorded and transcribed verbatim. Participants were reimbursed ZAR150 (~US $8.31 [ZAR18.04/$1]) for their time. We used findings from this phase to guide decisions about adjustments to increase the relevance of the intervention to the target population (Step 2).
Next, we conducted pretesting of the initial version of the adapted intervention with 20 people, some of whom participated in the in-depth interviews and agreed to future contact, and some newly recruited, using the same inclusion criteria and from the same communities described above, to gather participant feedback on the appropriateness and relevance of the content and any technological issues of the intervention (Step 3). Pretesting continued for a month. At the end of the 1-month period, participants were asked to provide feedback by completing acceptability and process measures on monitoring, contingent incentives, and weekly texts. Questions were designed to assess participants’ reactions to the intervention, what they learned, and suggestions for improvements. We used this feedback to refine the intervention (Step 4).
We presented the adapted intervention to our community collaborative board (CCB) as topical experts, to comment on necessary refinements. The CCB has been active since 2005 and includes representatives from nongovernmental organizations, community-based organizations, government, academic institutions, and communities where the intervention was to be tested (Myers et al., 2018). The feedback from these topical experts was used to make final adjustments (Step 5). Finally, we integrated all findings from previous steps into a final version of the intervention (Step 6) ready to be tested for acceptability and feasibility in a pilot trial.
Analysis
NVivo 12 software was used to manage the qualitative data. Data were analyzed, thematically using the Braun and Clarke approach (Braun & Clarke, 2006). We combined a deductive approach to coding based on the research questions concerning people’s needs and feedback regarding the proposed intervention, with an inductive approach to allow for the identification of emergent themes. PPW conducted the initial process of familiarization through a review of transcripts and coding. PPW and L-AE-C discussed the initial framework and individually coded the first two transcripts. Following this, they discussed refining of codes and themes. Intercoder reliability checks were conducted, with a Cohen’s Kappa score of 0.80 being obtained. Coding then continued independently for all transcripts. Any coding disagreements were resolved through discussion and consultation with YW. Excel 365 and SAS version 9.4 were used to manage quantitative data. Descriptive statistics were used to describe the data and summarized using the mean (standard deviations) for continuous variables and frequency (percentages) for categorical variables. In addition, we made use of visual presentations of urinalysis results.
Ethical considerations
Ethical approval was obtained for this study from the South African Medical Research Council’s Human Research Ethics Committee (EC002-2/2021). The Western Cape Department of Health (WC_202103_050) provided approval to conduct research activities in healthcare facilities. Participants provided informed consent to participate.
Results
Step 1: assessment
We conducted 32 interviews with women who were pregnant (P) with a mean age of 26 years. A total of 16 clinic and community members (CCMs) were interviewed. These consisted of researchers, government officials, substance use treatment specialists, clinic-based healthcare workers, and community health workers. In addition to the previously published findings, which highlighted the need for an alcohol intervention program that is innovative and tailored to the needs of women who are pregnant or postpartum, and the importance of including community-based support and possibly partner involvement in these interventions (Petersen Williams et al., 2024), participants described issues around program acceptability, feasibility, and provided various suggestions for future implementation.
Program acceptability, feasibility, and suggestions for implementation
While some clinic and community members thought using a device for mobile monitoring of alcohol use among perinatal people was a good idea, many raised concerns. One of the main concerns was that the perceived high street values of mobile devices, such as breathalyzers, would lead to devices being sold or stolen. Second, participants were concerned about limited access to mobile phones which may be necessary for the use of such devices. This was raised as a concern particularly for those living in more rural areas. Third, the concern was raised that people will not want to be monitored frequently and have healthcare providers informed every time they consume alcohol. Other concerns raised related to the possibility of people cheating when using a remote monitoring device and not being honest about who is providing the sample, devices being lost, and finally, the sustainability of the Department of Health funding the technology and infrastructure required for this long-term monitoring: There’s perhaps funding for this type of thing. And it shows you promise, but when it gets into policy implementation, then at sometimes given a grant, and then it’s not really sustainable over the long term. (CCM11)
Some perinatal participants also thought a mobile device could be easily stolen or not kept safe. In addition, many felt that people would be fearful in some instances to be monitored daily via breathalyzer: They won’t [blow] because, they will maybe be scared the children will be taken from them. (P14) If the person thinks he drank too much then he wouldn’t want to blow in there. (P13)
Some perinatal participants also thought the frequency of monitoring would be a problem, as it would be too burdensome to be monitored regularly. However, others felt it was a positive idea and would reduce drinking behavior: That—personally—is a very good thing that you’re giving the people to see when they’re using alcohol. Because there will be less—it will happen less. Fewer of them will use it [alcohol]. Because that is the thing that will—they will be seen through this. (P22)
Participants made recommendations for when and how often monitoring should take place. The suggested frequency of testing varied from 1 to 3 times a day. Given the local weekend binge-drinking culture, many participants thought it most practical to limit monitoring to weekends and/or specific days of the week known to be associated with heavy drinking: Your big problem is not necessarily people who are habitual drinkers, i.e. I need to drink every day like proper alcoholics, your problem here is someone that’s exposed to the environment that then drinks and then that does finish drinking over period. And that’s usually your Wednesday, Thursday, Friday, Sunday, or even Thursday, Friday, Sunday. (CCM11)
All the perinatal participants responded positively to the suggestion of being provided financial rewards contingent on abstinence from alcohol and thought it would be a great motivator for reducing drinking: Just want to say it will really encourage participants to get money every time their sample is negative. Because every time they think about lapsing, they will think, ahh how much money I’ve built up already. I can’t lose that money and they will continue to stay away from alcohol. (P1)
Similarly, there was overall support for contingency management from clinic or community members. However, concerns were raised about the feasibility of implementation from a policy point of view: So contingent measurement, this, I think, is a good thing. But unless it’s tied to a commitment by the [health] department [to fund this program], I don’t think there’s going to be benefit to it. So it does require quite a big policy shift. And I think it will probably be up to [you] to be able to sell this thing in such a way to be able to say this is a really good, cost benefit for you. Because we know that social support does uhm make a very positive impact in people’s lives . . . I am in support of the contingency being added to it, I’m just thinking to myself, only advice or comment that I would say is that it needs to be implementable on a larger scale. (CCM11)
Concerns were raised by clinic or community members about the use of cash incentives or too high incentives contributing to continued substance use rather than motivating change. A few therefore suggested replacing the cash incentive with grocery store vouchers or hampers or not inflating the cash value of the incentives: Cash, you know, they can spend on drugs and alcohol whereas a food voucher at a specific supermarket at least they can buy food. Because by giving cash you’re almost helping them to be able to buy their choice of product. (CCM2)
When asked about recruitment and retention of people in a program, participants mainly felt that the best place to recruit would be via healthcare facilities, as there was a general willingness of healthcare providers to assist in their facilities with recruitment. Some perinatal participants also recommended community-based recruitment through community health workers as well as making people aware through pamphlets and posters: Recruitment is tough. To keep them is also but often the incentives help. And it’s really important that you keep with the same messages, health messages that the promotions departments at health and metro work with, and use. (CCM2)
Although a few perinatal participants who already had older children were less interested in health promotion messages, as they felt they knew most things, generally, perinatal participants felt positive about receiving messages. They reported that sending positive messages (rather than telling them not to drink), such as information on the development of the baby at various stages of gestation and what to do or not do during pregnancy or what may be dangerous for the baby would be helpful: I will want to know what is—I don’t know if it’s like that—but what is dangerous? Like for the baby or for the mother during her pregnancy. Or what must you drink when you give birth, what must you really eat. Things like that. Like health. (P23) Definitely the do’s and the don’ts, because you’re not really sure like what is allowed during your pregnancy. And growth wise, baby growth wise and appointments. (P25)
Perinatal participants were asked about their views on alternative methods of testing for alcohol use. While some preferred urine tests, as it would mean only testing twice a week, as opposed to every day by breathalyzer, those perinatal participants who were employed preferred the breathalyzer to avoid clinic visits twice a week.
Despite some concerns raised by both community members and perinatal participants, there was consensus that some program or intervention for people who are pregnant and breastfeeding who drink is needed, particularly the additional support it would provide, compared to current health services: Because woman need empowering, especially these women, they don’t get empowered, you know, they are used to drinking, the partners are drinking. So you need to empower them in order for them to say no, but I’m not going to drink because it’s a benefit for my baby, even though my situation is like that, or whatever. (CCM13)
Step 2: decision
Based on these findings, we developed the Maternal Alcohol Reduction Intervention in South Africa (MARISA). As significant concerns were raised about the feasibility and barriers to using breathalyzers, we changed the alcohol monitoring from daily remote breathalyzer monitoring to twice weekly in-person urine testing to measure an alcohol metabolite (EtG). Incentives would then be provided on a weekly basis via a mobile “cash-send” mechanism. Since the frequency of monitoring with urinalysis would be twice a week instead of twice a day, the incentive magnitude for the first biochemically verified abstinence was set at R10, increasing by R10 up to R100. The same reset rule would apply, namely if a participant missed a clinic visit, is unable to provide a urine sample, or tests positive for alcohol use, the incentive magnitude would go back to R10 until the participant provided two consecutive alcohol-negative urine samples. With two consecutive alcohol-negative urine samples, the magnitude would be back to where it was before missing a clinic appointment or providing a urine-positive sample. A total potential earning will be R1590 (~US $88.14 [ZAR18.04/$1]).
Step 3: administration
Thirteen pregnant and seven postpartum people, with a mean age of 27 years (SD = 4.7), participated in pretesting the adapted intervention. In total, 15% were married, 40% were living with a partner, and 40% were not living with a partner. All participants had 12 years or less education, only 10% were employed and 5% (1/20) had an intended pregnancy. At baseline, the reported mean number of days participants had four or more drinks in the past month was 2 days, with 95% reporting three or more drinks on a typical day (Table 2). In total, 50% reported breastfeeding while drinking. Participants had a mean depression score of 14 (SD = 5.3) and 44% reported being emotionally abused by a main sexual partner in the past 3 months, while 6% reported physical and sexual abuse.
Participant characteristics (N = 20).

At the 1-month follow-up, the reported average number of days participants had four or more drinks in the past month reduced to 0.6 (SD = 1.3) days (Table 3). The mean percentage of alcohol-negative urinalysis was 88% (SD = 26%). The proportion of participants who reported alcohol use while breastfeeding decreased from 50% at baseline to 0%. Participants reported a mean depression score of 13 (SD = 5.8), 9% reported being emotionally abused by a main sexual partner since enrollment, and 11% reported physical and 6% reported sexual abuse (Table 3). The average amount earned by pregnant participants was ZAR621.55 (SD = 97.9) and by postpartum participants ZAR617.50 (SD = 107.8).
One-month follow-up.

When asked at the 1-month follow-up how they felt about providing urine samples for alcohol monitoring, on a scale of 1 (not at all comfortable) to 5 (very comfortable), 82% responded with a “5.” Similarly, participants were asked, “How helpful has this incentive program been in helping you abstain from alcohol use?,” “How helpful has this program been in helping your infant stay healthy?,” and “How do you feel about accessing support remotely via mobile technology such as texting?” In total, 96%, 86%, and 82% responded with “5” (very comfortable) to these questions, respectively.
Step 4: production
Following the pretesting, adjustments were made to address various issues before the pilot testing. Based on the findings from Step 3, we confirmed that our procedure works. We decided to continue with urinalysis to monitor alcohol use. Furthermore, it was decided to have more stringent inclusion criteria for the pilot trial, which meant biologically verified alcohol use would be a requirement for inclusion in the trial. Since we did not receive any responses to our text messages, we decided to only include text messages providing information and would not ask any questions requiring an answer, such as “How are you feeling today?” Furthermore, pretesting the use of cash transfers as incentives showed promising results, so we decided to continue using cash incentives and not to switch to vouchers.
Step 5: topical experts feedback and community collaborators
The adapted intervention was presented to an established community collaborative board (CCB) for further feedback to refine the intervention. Following the recommendations of the CCB, it was decided that all health messaging would be sent to women via SMS text message rather than WhatsApp messages to avoid issues related to nondelivery due to them not having airtime/data/Wi-Fi to receive such messages. In addition, the CCB recommended the inclusion of referrals for domestic violence services, given the high levels of domestic violence experiences among the pretesting sample.
Step 6: integration
Feedback from previous steps was integrated into version 2 of the MARISA program. The adapted intervention includes twice weekly urinalysis for alcohol use; provision of contingent incentives via a cash send mechanism, and weekly health promotion text messages.
Discussion
The current study describes the process of adapting an evidence-based contingency management and health text messaging intervention to encourage alcohol use reduction during pregnancy and lactation. The first six steps of the ADAPT-ITT framework guided our adaptation process. To the best of our knowledge, this is the first behavioral intervention to monitor alcohol use with contingent financial incentives and text-based health promotion and referrals for alcohol use reduction during pregnancy and lactation in the South African context. The proposed intervention is innovative in that it combines alcohol monitoring-based CM with text-based health promotion messages tailored to maternal populations. The text messages will include health promotion messages addressing alcohol and other substance use, breastfeeding, gender-based violence, maternal/infant health, physical and mental health, and other psychosocial matters.
We had originally planned to monitor alcohol use by means of remote breathalyzers, but the adaptation process highlighted feasibility and acceptability concerns. Concerns included the perceived high street value of a monitoring device, access to mobile phones to use such a device, frequency of monitoring, cheating when using the remote monitoring device, devices being lost or stolen, and the sustainability of long-term monitoring. Findings from previous research suggest that smartphone-based remote alcohol monitoring by means of breathalyzers shows some promise for tracking alcohol consumption, but that adherence to monitoring tasks could be improved (Lauckner et al., 2019). Studies have shown, however, that despite mixed views on the usability of breathalyzer monitoring, the use of CM to reward negative samples increased the likelihood of submitting negative samples, and the combination of a smartphone device and mobile breathalyzer shows promise for integration with CM and may increase the utility and reach of CM (Oluwoye et al., 2020). It is therefore plausible that, despite the concerns raised relating to use of breathalyzer monitoring devices, remote monitoring using this mechanism rather than twice weekly urine monitoring may be possible in this population. However, given the excellent follow-up rates and adherence to twice-weekly monitoring protocol, the current intervention utilizing urine testing, which has been shown to be feasible with this population (Petersen Williams et al., 2014), combined with CM shows promise, particularly since the majority of perinatal participants expressed a preference for urine testing. Despite concerns raised about the use of cash incentives or too high incentives, pretesting showed promising results with the continued use of cash incentives. This finding is in line with prior research with substance abuse treatment clients showing that neither the magnitude nor mode of payment had a significant effect on new drug use or perceived coercion (Festinger et al., 2008). Furthermore, there is a growing body of evidence for the cost-effectiveness and sustainability of the CM approach, which is encouraging for the allocation of funding for this approach to behavior change (Kirby et al., 2016; López-Núñez et al., 2016; Petry, 2011; Petry et al., 2017; Secades-Villa et al., 2014).
The current study demonstrated widespread acceptance for receiving text-based health promotion messaging and support despite the lack of responses to these messages during pretesting. The adapted intervention therefore will continue to send text-based health messages. However, these will not ask any questions requiring a response. The content was developed using concepts of the educational component of an evidence-based brief intervention for women’s alcohol and other substance use (Wechsberg, 1998). Current evidence suggests that text messaging in healthcare interventions shows substantial benefits, with text messaging improving attendance at appointments and behavior change outcomes (Mbuagbaw et al., 2015; Militello et al., 2012; Yeager & Menachemi, 2011). The text-based health promotion and referral content will also be incorporated according to the evidence of how lifestyle, mental health, and sexual health affect maternal alcohol use (Jones et al., 2014; Pitpitan et al., 2012).
Domestic violence among pregnant and postpartum people is an important public health concern. Studies in South Africa have demonstrated high prevalence of domestic violence, including intimate partner violence against pregnant and postpartum people (Bernstein et al., 2016; Field et al., 2018; Matseke et al., 2021). The correlation between experiences of intimate partner violence (IPV) and substance use among women is also well established (Ogden et al., 2022). In the current study, high levels of abuse by a main sexual partner were reported in the pretesting sample. While levels of emotional abuse decreased from baseline to the 1-month follow-up following the intervention, experiences of physical abuse increased among participants who were pregnant at enrollment. Based on this and feedback from topical experts, we added additional referrals for domestic violence.
The application of the ADAPT-ITT framework offered several uses and lessons, particularly when adapting interventions to new contexts. Applying the framework ensures that the intervention is tailored to the specific cultural and contextual needs of the target population, which is crucial for its acceptance and effectiveness. It involves local communities and stakeholders in the adaptation process, fostering buy-in and support for the intervention. It helps identify and address the unique barriers and needs of the target population, ensuring the intervention is appropriately tailored. It enhances the likelihood that the intervention will be feasible and acceptable to the target population, improving the chances of successful implementation. Finally, by making the intervention more relevant and suitable for the target population, it maximizes the potential impact on the desired outcomes, such as reducing alcohol use and improving health. In the South African context, the implications for program adaptation and content when using the ADAPT-ITT framework are significant. These implications revolve around ensuring that interventions are culturally appropriate, contextually relevant, and effectively address the unique challenges faced by the population. Programs must integrate local cultural beliefs, practices, and norms around pregnancy, lactation, and alcohol use to ensure acceptance. Interventions need to consider the socioeconomic context, including poverty, unemployment, and limited access to healthcare, which can influence health behaviors and outcomes. Programs need to be adapted to fit within the existing healthcare infrastructure, which may be resource-constrained, and ensure that they complement rather than overburden the system. Interventions should be tailored to address specific patterns of alcohol use prevalent in South Africa, including binge drinking and its social acceptability. Program goals should align with national and local health priorities, such as reducing maternal mortality and improving infant health outcomes. Local communities and stakeholders should be involved in the adaptation process to foster ownership and ensure the intervention meets their needs. Empowerment-based approaches that build capacity and resilience among pregnant and lactating women, enabling them to make informed health decisions should be used. By considering these implications, program adaptations in the South African context can be more effective in reducing alcohol use during pregnancy and lactation, ultimately improving maternal and infant health outcomes.
There are some limitations to this formative work. We were unable to recruit postpartum participants for the formative interviews as part of Step 1 assessment, and therefore, all participants interviewed were currently pregnant. However, we were able to include breastfeeding people in the pretesting administration step. The second limitation is that the experiences of participants may not be generalizable beyond the specific communities they were recruited from. It is likely though that findings are relevant to women in similar settings, such as are prevalent throughout South Africa. Our topical experts also work across various communities, organizations, and settings.
Conclusion
Despite these limitations, the current study describes a rigorous process for adapting an evidence-based intervention for alcohol use reduction during pregnancy and lactation. The adapted intervention combines alcohol monitoring-based contingency management (CM) with text-based health promotion and information on where to access services tailored to maternal populations ready to be tested in a feasibility pilot study before conducting a fully powered randomized controlled trial.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institute on Alcohol Abuse and Alcoholism (NIAAA) (R21AA029048). The research was also supported by the South African Medical Research Council (SAMRC).
Trial registration
Trial registration number: NCT05319977.