
Abstract
Objective
Hereditary angioedema is a serious disease with unpredictable attacks. It has an impact on patients’ health-related quality of life. This study aimed to assess the quality of life of the hereditary angioedema patients and to investigate the relationship between quality of life and demographic, clinical, laboratory, and psychiatric parameters.
Method
A semistructured face-to-face interview, Hamilton depression rating scale, and Hamilton anxiety rating scale were performed by a psychiatrist. Participants completed Medical Outcomes Study Short Form-36, Revised Form of the Multidimensional Scale of Perceived Social Support, Anxiety Sensitivity Index-3, and Adult Separation Anxiety Questionnaire. Patients’ complement results were recorded, and clinical data obtained by interview were cross-checked from patients’ files.
Results
In 33 hereditary angioedema patients, subscales of the Study Short Form-36, except for physical functioning, vitality, and mental health were significantly lower compared with population norms. Quality of life scores were found to be correlated with depression, anxiety, anxiety sensitivity, separation anxiety, perceived social support, perceived discrimination, perceived limitation, treatment naïve C1-Inhibitor function, and C1q level. Physical role functioning scores were better in the patients using attenuated androgens (p = 0.006, t = −3.027). Hereditary angioedema contributed to the marital problems and childbearing decisions of the patients.
Conclusion
Hereditary angioedema results in significant impairment in quality of life of the patients and has an impact on family life and life style of the patients. In case of depressive and/or anxiety symptoms, patients should be referred to psychiatrists for better quality of life. Higher levels of C1-inhibitor function and C1q seem to correlate with better quality of life; these needs to be further studied.
Keywords
Introduction
Hereditary angioedema (HAE) is a rare autosomal-dominant inherited disorder characterized by recurrent attacks of swelling that can commonly affect the extremities, gastrointestinal tract, face, and upper airways. Although the swelling is self-limited, without treatment, laryngeal involvement may cause fatal asphyxiation. A dysfunction of C1 inhibitor causes HAE. 1 Being a debilitating and potentially life-threatening disease, improper diagnosis, inappropriate treatment, and delay in diagnosis contribute to the burden of HAE. As HAE has attacks that are unpredictable and leads to a frequent need for medical intervention and time away from normal activities, it has an impact on patients’ health-related quality of life (QOL). 2
Several studies showed the impairment in QOL of HAE patients.2–10 The only opposite result is from Denmark; in Danish, patients’ mean scores of QOL corresponded to population norms. 11 Some studies attempted to quantify the QOL by using standardized instruments such as Medical Outcomes Study Short Form-36 (SF-36),3,5,7,10,11 SF-12, 2 European QOL 5 Dimensions,12,13 or RAND 36-Item Health Survey. 13 Some of them have been web- or telephone-based2,14 or retrospective. 9 A few studies aimed to assess the impact of treatment options on QOL.7,15
For prophylaxis, attenuated androgens and tranexamic acid are the only medications supported by Turkish health-care system; for acute treatment, C1 inhibitor concentrate (Cinryze®) and bradykinin B2 receptor antagonist, icatibant (Firazyr®), are available.
Although it is shown that depressive and anxiety symptoms are common in patients with HAE and these may trigger HAE attacks; there is a paucity of data about emotional reactions of HAE patients. 16 Due to unpredictable attacks, anxiety sensitivity may be high in HAE patients. We hypothesize that the level of anxiety sensitivity and separation anxiety will affect the QOL of HAE patients.
In this study, we aimed to assess the QOL of the HAE patients and to investigate the relationship between QOL and demographic, clinical, laboratory, and psychiatric parameters. Our secondary aim was to obtain data concerning the patients’ experiences of disease with a face to face interview made by a psychiatrist.
Method
This cross-sectional study was conducted by the Department of Internal Medicine, Division of Allergy and Clinical Immunology, and the Department of Psychiatry.
Participants
Patients with HAE were recruited from the Department of Internal Medicine, Division of Allergy and Clinical Immunology. All the patients were diagnosed with HAE according to medical history and laboratory parameters. Type I HAE patients were characterized by low C1 inhibitor antigenic level and dysfunctional C1 inhibitor protein; type II HAE patients were characterized by normal or elevated C1 inhibitor levels and dysfunctional C1 inhibitor protein.17,18 All blood samples for complement proteins were taken at the time of diagnosis, in the treatment-free period, and these basal values were used in this study. C4 (reference range: 10–40 mg/dL) and C1 inhibitor antigen levels (reference range: 21–39 mg/dL) were analyzed by immunonephelometry (Siemens, Marburg, Germany), and functional C1 inhibitor (reference range: 70%–130%) was measured by chromogenic assay (Berichrom Siemens, Marburg, Germany). Semiquantitative C1q levels (reference range: 100–300 μg/mL) were tested by radial immunodiffusion, using the C1q Binarid Radial Immunodiffusion kit (Binding Site, Birmingham, UK). There is no validated symptom severity score for HAE patients; nevertheless, we used Freiberger score. 19 This detailed symptom score ranging from 0 to 11—where 0 represents the mildest, and 11 represents the most severe scores—includes the frequency of attacks and age of HAE onset. Besides, in this study, patients were asked to assess their attack severity (estimation of all attacks); subjectively as mild, moderate, or severe; without giving any criteria for classification.
The inclusion criteria for the study were defined as HAE diagnosis confirmed clinically and by laboratory tests, as mentioned above, age between 18 and 65 years, volunteering to participate in the study, and being able to provide written informed consent. The exclusion criteria were defined as having a diagnosis of bipolar disorder, psychosis, dementia, or mental retardation as well as pregnancy and medical comorbidity which can also affect QOL. Among 40 volunteer patients, 33 participants matching the criteria constituted the sample (Figure 1).
Flowchart of the sample selection.
Procedure
This study was approved by the local ethics committee (Approval Number: 16–5.1/3) Procedures were in accordance with the Helsinki Declaration, Fortaleza, Brazil, 2013. All subjects were recruited after obtaining a proper written informed consent.
Case report forms providing data about the burden of HAE, disease characteristics, complement levels, and sociodemographic data were filled, with a face to face interview made by a psychiatrist. Subjects underwent clinician-rated evaluations for depression level with Hamilton depression rating scale (HAM-D) 20 and for anxiety level with Hamilton anxiety rating scale (HAM-A). 21 Participants completed self-report questionnaires such as SF-36, 22 Revised Form of the Multidimensional Scale of Perceived Social Support (MSPSS), 23 Anxiety Sensitivity Index-3 (ADI-3), 24 and Adult Separation Anxiety Questionnaire (ASA). 25 The adaptation and reliability studies of all of the scales and interviews for the Turkish population had been performed previously.26–31 A study for obtaining population norms for the Turkish version of SF-36 has also been performed. 32
Statistics
Results were expressed as mean and standard deviations if there was a normal distribution, and as median with minimum to maximum values or 25th–75th percentiles if there was skewed distribution. IBM SPSS Statistics 21 program was used for statistical analysis. Shapiro–Wilk test was used to test normality. To compare the quantitative data, we used Student’s t test for the data with normal distribution and Mann–Whitney U test was used for the data with skewed distribution; for comparison of qualitative data, χ2 test or Fisher’s exact test was used. Pearson correlation analysis was used to assess correlations between continuous variables with normal distribution, and Spearman’s rank test was used for the variables with skewed distribution. Multiple regression models with a stepwise procedure were performed including the variables which were found to be correlated with the analyzed SF-36 subscale. A p value of <0.05 was considered to indicate statistical significance.
Results
The demographic data, disease characteristics, and SF-36 results of the sample are provided in Tables 1 and 2. None of the patients were within attack period while attending the research.
Demographic and clinical data of the patients with hereditary angioedema.
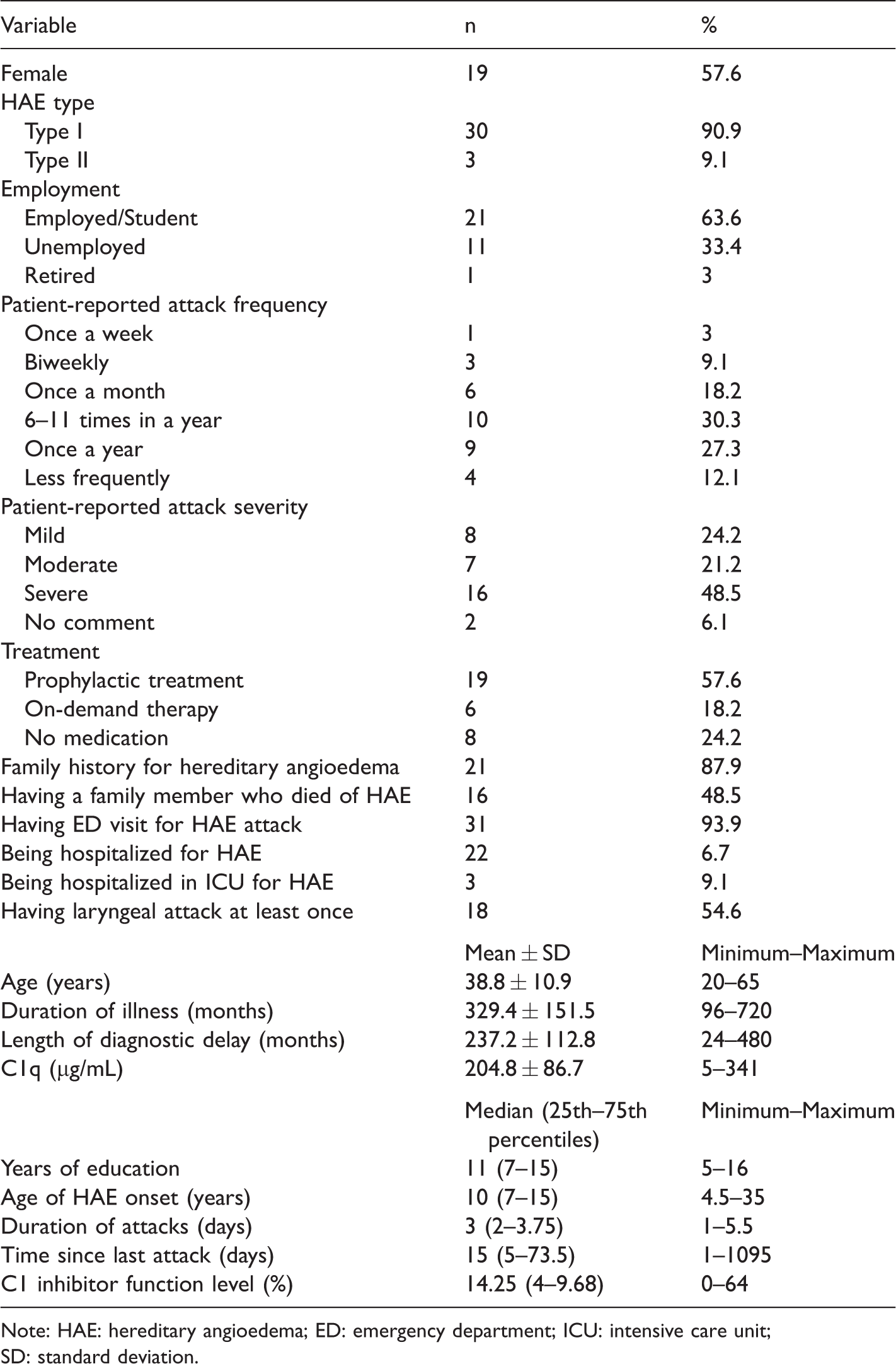
Note: HAE: hereditary angioedema; ED: emergency department; ICU: intensive care unit; SD: standard deviation.
SF-36 results of the patients with hereditary angioedema.
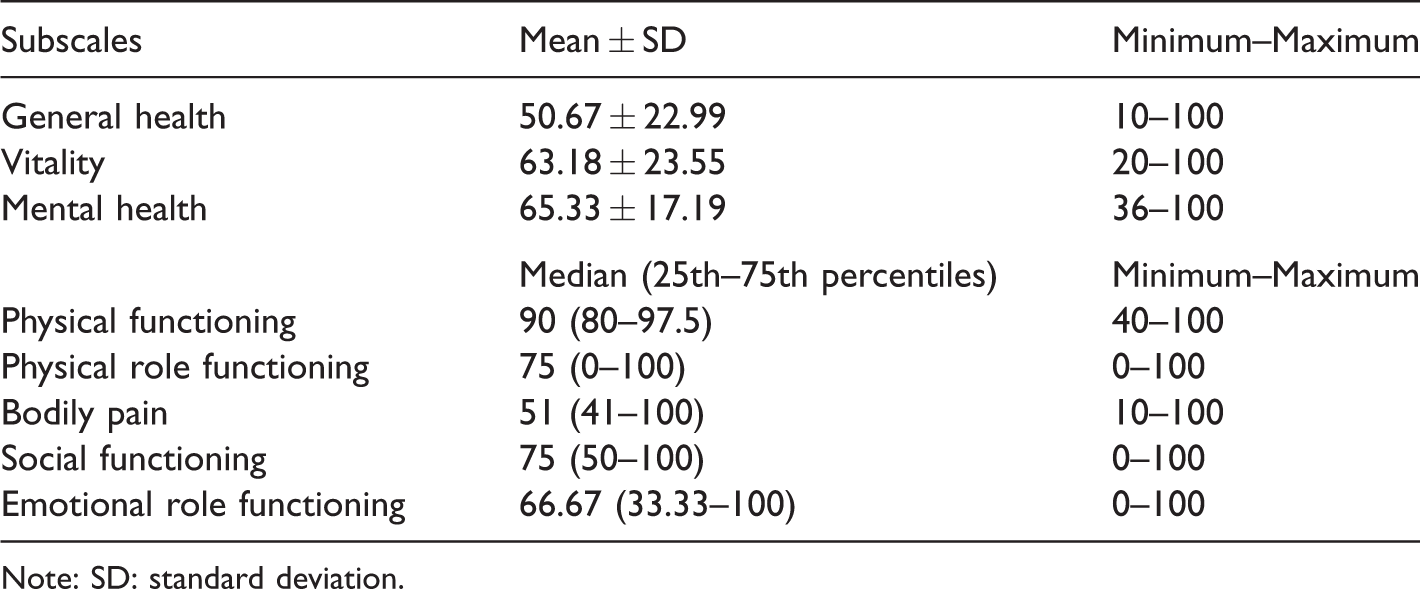
Note: SD: standard deviation.
Results related to SF-36 Scores
Mean scores for emotional role functioning (ERF), social functioning (SF), general health (GH) perception, bodily pain (BP), and physical role functioning (PRF) subscales of SF-36 were significantly lower for HAE patients, compared with population norms (Figure 2). The population studied for getting normative data was similar to our study group regarding age and gender. 32

Comparison of quality of life results of the hereditary angioedema patients with normative data. SF-36 results are shown as error bars. The numbers in the boxes are the normative values for the Turkish population. SF-36 scores of the sample are compared with the normative values. Calculated p values based on t test are shown in the boxes. CI: confidence interval.
Twenty-five patients (75.8%) had received misdiagnosis before they were diagnosed with HAE, and they had undergone unnecessary treatments. Misdiagnosed patients had significantly lower scores for BP (medians: 87 vs. 51; p = 0.040, Z = −1.440). Nineteen out of the 33 patients were taking attenuated androgens (danazol at doses ranging from 50 mg every other day to 200 mg daily) as the prophylactic treatment. Six out of the 33 patients were on-demand treatment with C1 inhibitor concentrate (Cinryze®) and/or bradykinin B2 receptor antagonist, icatibant (Firazyr®). The remaining eight patients were treatment free. Patients with prophylactic treatment (attenuated androgens) had significantly better scores for PRF than the rest of the sample (Table 3). The only gender-related difference was in physical functioning (PF) (p = 0.006, t = −3.027); males had better scores (93.21 ± 6.68) than females (81.05 ± 15.69). There was no association between patient-reported attack severity and SF-36 scores. Two patients did not comment on their attack severity, as they did not have an attack for a long time (Table 1).
Comparison of quality of life results of the hereditary angioedema patients with and without prophylactic treatment.

Note: n: number; SD: standard deviation; Values marked in bold indicate a statistically significant difference (p<0.05)
aFor prophylaxis, attenuated androgen treatment is the only medication supported by Turkish health-care system.
Significant correlations between QOL scores and patients’ demographic characteristics and disease variables are shown in Table 4. There was no correlation between the SF-36 subscales scores and current age, the age of HAE onset, duration of illness, delay in diagnosis, time since the last attack, duration of attacks, having a laryngeal attack, C1-inhibitor level, C4 level, and disease severity score. 19 Laryngeal death in the family did not affect SF-36 subscale scores.
Correlation between SF-36 subscales and some variables.
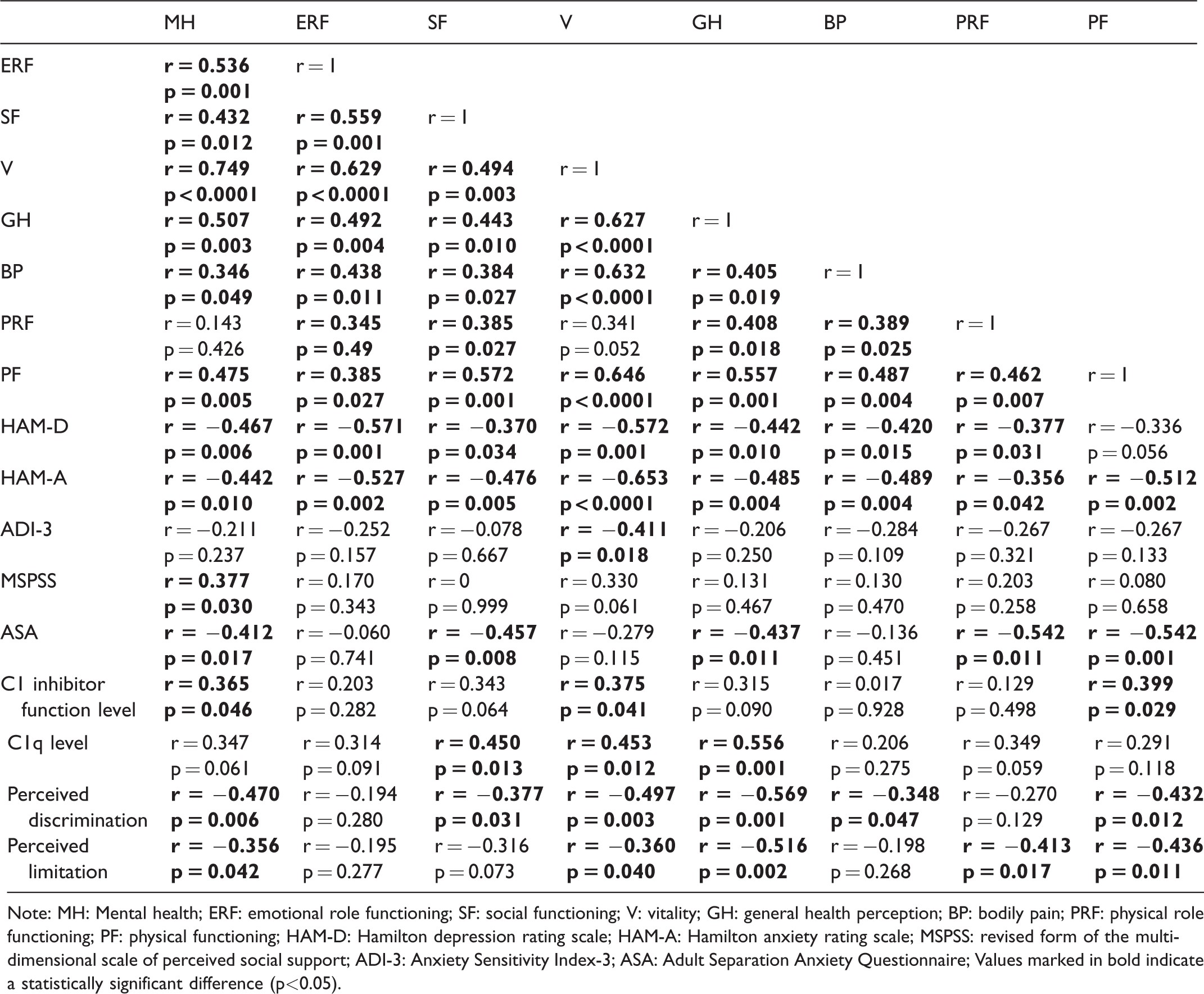
Note: MH: Mental health; ERF: emotional role functioning; SF: social functioning; V: vitality; GH: general health perception; BP: bodily pain; PRF: physical role functioning; PF: physical functioning; HAM-D: Hamilton depression rating scale; HAM-A: Hamilton anxiety rating scale; MSPSS: revised form of the multidimensional scale of perceived social support; ADI-3: Anxiety Sensitivity Index-3; ASA: Adult Separation Anxiety Questionnaire; Values marked in bold indicate a statistically significant difference (p<0.05).
Independent variables which have significant correlation and association with the scores of SF-36 subscales were included in the multiple linear regression models. Independent variables are given in Table 5, in the order of entry into the model.
Results of stepwise multiple regression analyses.
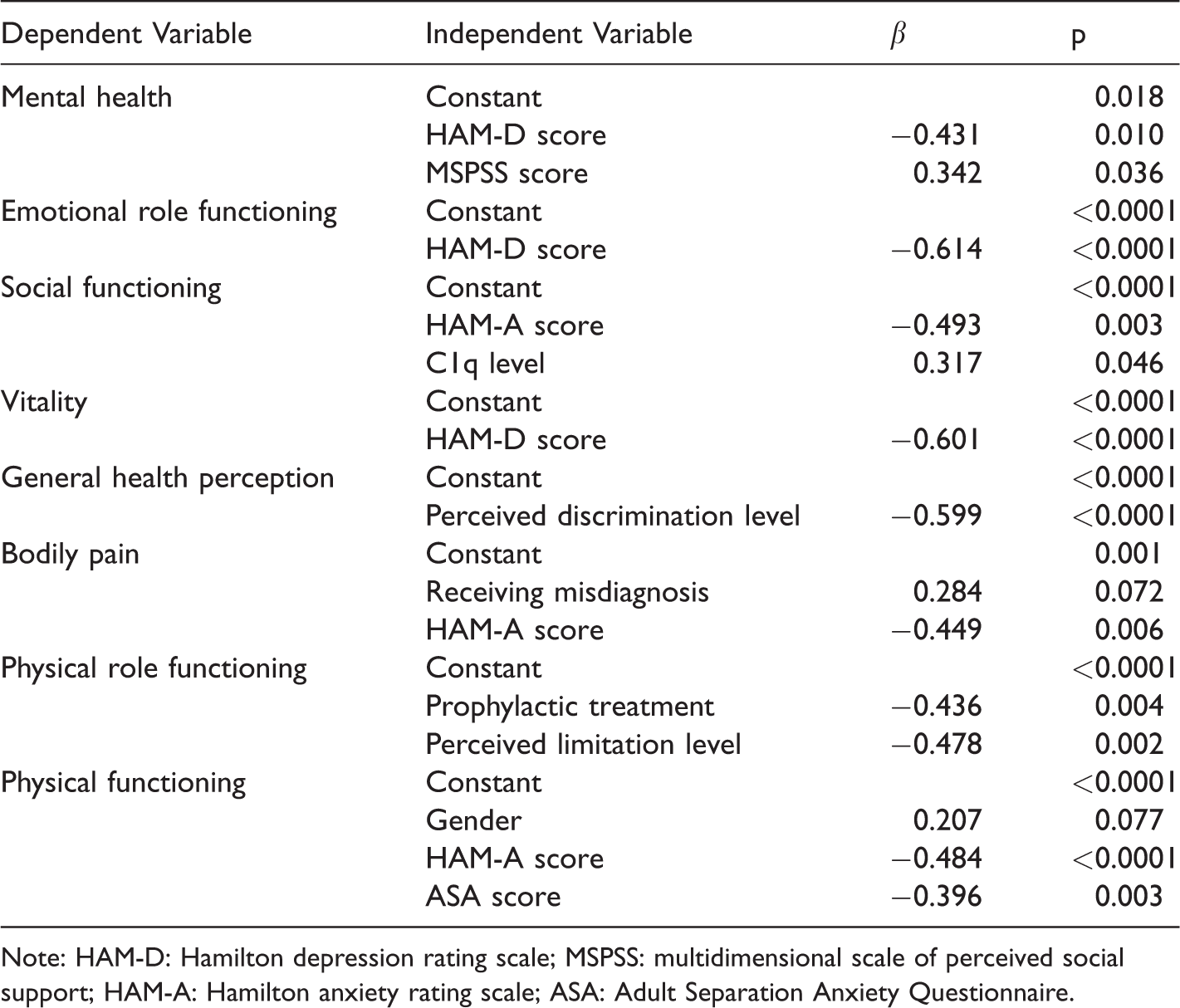
Note: HAM-D: Hamilton depression rating scale; MSPSS: multidimensional scale of perceived social support; HAM-A: Hamilton anxiety rating scale; ASA: Adult Separation Anxiety Questionnaire.
Results related to family planning decisions
Four single and five married patients had negative thoughts about marriage, due to their disease. Those married patients declared that HAE contributed to their marital problems. Among 33 patients, 22 (66.7%) patients had negative thoughts about having children, due to the anxiety of passing the disease to the children. Hence, some of them chose not to have children or to have fewer children than they had wished. A single young man in the sample said “No need to pass this disease to new generations …” while he associated his parents’ divorce with his father’s HAE disease.
Perceived discrimination and limitation
The patients were asked “to what degree do you feel different from others who have not HAE?” to analyze their level of discrimination perception. It was scored between 1 and 10. Sixteen (48.5%) patients scored above 5. Perceived discrimination level was significantly correlated with HAM-D scores (p = 0.023, r = 0.395), HAM-A scores (p = 0.005, r = 0.481), ASA scores (p = 0.002, r = 0.514), and the level of C1q (p = 0.003, r = −0.516). Patients were asked about their level of limitation due to HAE, and it was also scored between 1 and 10. Ten (30.3%) patients scored above 5. Perceived limitation level was significantly correlated with the perception of discrimination level (p < 0.0001, r = 0.620) and ASA scores (p = 0.005, r = 0.479).
Fears
The greatest fears of the patients about having HAE were sudden airway closure in 15 (45.5%) patients, death in 4 (12.1%) patients, and transmission of HAE to their children in 2 (6.1%) patients. Eight patients among the ones whose greatest fear was sudden airway closure had never had a laryngeal attack. Having an attack in a special day, such as a wedding, having an abdominal attack when the patient was alone, being disabled in the future, having an attack in the face, and having difficulty in accessing the drugs were other five greatest fears, in each patient (n = 5, 15.1%). Seven (21.2%) patients declared that they have no fear about HAE.
Discussion
Consistent with the literature, we found that QOL impairment continues even between attacks, despite full physical recovery between attacks.2,10,12,14,33,34 ERF, SF, GH, BP, and PRF subscales of SF-36 were significantly lower for HAE patients, compared with population norms. As far as we know, only Aabom et al. did not find impairment in QOL of HAE patients. They suggested that this finding is related to good health-care system and availability of new treatment options in Denmark. 11 In our study, the patients using on-demand treatment of attacks are few. As it is not easily accessible, they mostly keep it only for very severe attacks, which eventually might have a negative impact on QOL. Banerji et al. suggested that availability of new treatment options will improve the QOL of the HAE patients. 8 Despite the fact that most of the patients in our sample use attenuated androgens for prophylaxis, they report attacks. In the study of Lumry et al., it has been found that patients taking attenuated androgens had reduced level of productivity and QOL compared with patients not taking androgens. 2 Androgens are often prescribed to patients with more severe disease, 35 and this might be the cause of lower QOL of the patients taking androgens, reported in previous studies. However, in our study, there was no treatment-related significant difference for seven subscales of SF-36, and for PF patients taking attenuated androgens had better scores than the patients without prophylactic treatment. This result may be related to anabolic properties of androgens, as androgens increase muscle strength and aerobic capacity. 36
Finding no impairment in vitality and PF subscales was an unexpected finding. In a Brazilian 5 and a Canadian study, 10 impairment in vitality was more pronounced. There is no significant difference regarding these dimensions between the Turkish population and other country populations.32,37,38 Further QOL studies involving Turkish HAE patients are needed to clarify this finding.
In our study, some demographic, clinical, biological, and psychiatric parameters which can affect QOL of the HAE patients were investigated. With multiple regression analysis, gender, depression, anxiety, perceived social support, separation anxiety, perceived discrimination, perceived limitation level, receiving a misdiagnosis, C1q levels, and prophylactic treatment were found to be predictors for QOL of HAE patients. Each predictor parameter will be discussed in order. Effect of treatment was addressed earlier.
For gender, males had better scores for PF. This result may not be related to HAE, as QOL in men is generally better in Turkey. 32 Multiple regression analyses showed that depression score is the single best predictor for MH, ERF, and vitality; and anxiety score is the single best predictor for SF, BP, and PF in HAE patients. These results are not surprising as depression and anxiety lead to impairments in QOL. 39 Perceived social support score was found to be the next best predictor for MH, after depression scores. HAE is a debilitating disease that needs a caregiver in acute attacks. 14 Thus, for HAE patients, low level of social support seems to affect mental QOL negatively, when especially there is depression. Concordantly, separation anxiety scores were found to be correlated with MH, SF, GH, PRF, and PF. Separation anxiety is a disabling distress when faced with actual or perceived separation from major attachment figures. 40 Fear of having an attack when there is no caregiver seems to interfere with many domains of QOL, for HAE patients. In our sample, nearly half of the patients had perceived discrimination. HAE patients who have discrimination, in other words, who feel themselves much more different from other people are more depressive and/or anxious; discrimination is also associated with reduced QOL. Besides, discrimination was found to be the best predictor of GH. Thus, we can say that HAE patients with a high level of perceived discrimination feel themselves sicker. Discrimination is a neglected area in HAE. It may interfere with help-seeking and treatment-seeking behavior of the patients. Patients with high perceived limitation level also had high perceived discrimination. The correlation between separation anxiety and perceived limitation level may be because of the fear of having an attack when there is no caregiver. Feeling being limited appears to make patients feel more nervous, tired, and unhealthy. Besides, it was found to be the second-best predictor of PRF. An interpretation for this is HAE patients who have problems with work or other daily activities because of physical health, feel more limited. Although there is no correlation between length of diagnostic delay and QOL scores, misdiagnosed patients had significantly lower scores for BP. Misdiagnosis might prevent relief of pain and alter pain perception, leading to impairment in QOL in the future. This suggestion needs to be confirmed by prospective studies. C1q level was found to be the second-best predictor for SF, after anxiety scores. Besides, although in multiple regression analysis treatment naïve C1 inhibitor function level did not show association with QOL, it was found to be correlated with MH, vitality, and PF. The analysis of C1 inhibitor function level is the main diagnostic parameter for HAE C1 inhibitor deficiency. As far as we know, no study investigated and showed a correlation between complement proteins and QOL. According to our results, a higher level of the C1q is a predictor of higher social functioning.
Anxiety sensitivity has been defined as an excessive fear from senses and symptoms of anxiety. 30 For the first time, we investigated the relationship between anxiety sensitivity and QOL in HAE in this study. Anxiety sensitivity was found to be negatively correlated with vitality scores. However, this significance disappeared after regression analysis. People with high anxiety sensitivity may feel tired and worn out all the time and so have low vitality scores. Anxiety sensitivity needs to be further studied, as we know that distressing life events may precede attacks. 16
In a French study, QOL was found to be negatively correlated with the annual number of attacks, 4 but we did not get such a correlation. SF-36 is an important tool for the evaluation of QOL. However, it does not address the unique characteristics and symptoms of HAE. Maybe, because of using a generic instrument, we could not find a correlation between QOL and some disease characteristics, such as disease severity, duration, and age at onset.5,11 Recently, an HAE-specific QOL questionnaire is developed. 41 As adaptation and reliability study of this scale for the Turkish population has not been performed, we could not use this questionnaire. New studies using this questionnaire are needed. On the other hand, using SF-36 enabled us to compare the results of HAE patients with normative Turkish population data.
In the study of Huang, the three greatest fears were sudden airway closure (85%), intolerable pain (65%), and transmission of HAE to their children (55%) in 63 patients with HAE. 42 Consistently, in our study, the most common greatest fear was sudden airway closure. It is noteworthy that more than half (53.3%) of the patients whose greatest fear was sudden airway closure had never had a laryngeal attack. In addition, four patients’ greatest fear was death. As the laryngeal attack is the only life-threatening feature of HAE, we can assume that totally 57.6% of the patients’ greatest fear is having a laryngeal attack and therefore death. Although only two patients’ greatest fear was the transmission of HAE to their children, most of the participants were concerned about having children because of the heredity factor of this disease. Some patients also had negative thoughts about marriage. Consistent with the study of Bygum et al., all these fears interfere with the patients’ family life and their lifestyles. 14
Making a face to face interview with the entire sample by a psychiatrist is the strength of our study. Also, as far as we know, this is the only study which investigates the correlation between QOL and diagnostic complement parameters of HAE; first study that explores separation anxiety and anxiety sensitivity in HAE patients. Besides, this study has some limitations. As the study was cross-sectional, it was not possible to detect a certain causal relationship. Recall periods for patients’ most recent attack varied from patient to patient. Prospective studies will be helpful in understanding the relationship between disease progression and QOL. Another limitation is population bias. Patients who are willing to attend this research may differ from the ones who do not want to participate. Also, the sample was selected from a group of patients who were managed by an HAE specialist. As it is mentioned in the study of Bouillet et al.; 4 patients who are not managed by HAE specialist may be undertreated and so have worse QOL. On the other hand, underdiagnosed patients may have a milder form of the disease, and so they have a better QOL. In addition, the sample size is small; but it is noteworthy that such a sample is sizeable for this rare condition.
As a conclusion, HAE results in significant impairment in QOL of the patients and has an impact on the family life and the life style of the patients. Based on our results, we may recommend that the patients with depressive and anxious symptoms should be referred to a psychiatrist as these symptoms may further decrease the QOL of the HAE patients and increase their perceived discrimination. The finding of the correlation between QOL and the separation anxiety scores and social support scores of the patients proves the importance of the caregivers in the treatment of HAE. These should be studied in prospective projects. Further psycho-immunological studies are needed to explain the relationship found between the complement proteins and QOL.
Footnotes
Authors’ note
The preliminary results of this study had been presented in EAACI Congress 2017 in Helsinki by the title “Health related quality of life in hereditary angioedema patients” and selected as an abstract prize winner.
Acknowledgments
The authors are thankful to their colleague Nazlı Kahraman for her assistance in data collection. The authors are also grateful to Timur Köse and Semiha Özgül from Biostatistics and Medical Informatics Department of Ege University.
declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.