
Abstract
The United States military is an organization composed of teams of various sizes and functions. The development of effective teams is comprised of several components: leadership, followership, training, and development of team traits. This article reviews the literature and military doctrines surrounding these components to establish a conceptual model of team development. This model is intended to summarize military team development principles and to facilitate team functioning and development within medical settings. Organizational values, leader attributes and competencies, and the role of team members are discussed.
Military culture and context
The United States military is composed of 3.5 million members including Active Duty components in the Army, Navy, Marine Corps, and Air Force; Reserve and National Guard units; and civilian personnel. 1 Each military branch possesses unique cultural characteristics, traditions, standards, and provides a specialized contribution to the national security of the U.S. Many are drawn to the military by a sense of patriotism, a determination to serve one’s country, and a desire for adventure. 2 These shared interests are reflected in each branch’s set of core values. Military values are integral for team development and performance, as they reflect institutional standards of conduct. 3
A detailed discussion of each military branch’s core values is beyond the scope of this article; therefore, the authors focus on the U.S. Air Force as an example. The values of the Air Force are “Integrity First, Service Before Self, and Excellence in All We Do.” 4 Put simply, integrity reflects an Airman’s willingness to do what is right even when no one is looking; service represents a constant commitment to duty; and excellence suggests the priority to achieve the highest standards to complete the mission. 3 These values can be tailored to promote communication, development, and teamwork within the family medicine training environment.
Lt Col Alley’s model Air Force Family Medicine Core Values (Figure 1) utilizes a tiered framework to outline the growth of a family physician as they progress through a graduate medical education (GME), specifically family medicine, residency. 5 At the foundational level, residents prepare themselves to be fully functioning family physicians by embracing the ethical values of the military and medical professionals. The next tier, excellence, addresses the heart of the GME mission; residents are expected to master their craft, develop a broad knowledge base, and embrace a mindset of lifelong learning. Finally, with a solid ethical and professional foundation, competence, and expertise within the field, they are prepared to serve patients in a variety of settings with full-spectrum care.

Air Force Family Medicine Core Values. 5
The team approach
Irrespective of the practice setting, an indisputable but evolving tenant of family medicine is a team-based approach to medical care. 6 A family medicine clinic comprises many medical professionals and paraprofessionals, who possess various levels of training but serve complimentary roles. Cohesion is paramount to maintain or enhance the functionality, productivity, and development of a family medicine team to provide high-quality care. 6 Cohesive, high-performance teams are developed through a combination of sound leadership, active followership, understanding stages of team development, enhancing team maturity, and effective training.
Effective teams have a leader to direct, guide, and encourage accomplishment of the team’s assigned tasks; the designation of a leader ensures accountability and responsibility for the outcomes. The leader functions, in part, to encourage others to follow by “providing purpose, direction, and motivation to accomplish the mission and improve the organization.” 7 A leader should be perceived as trustworthy to his/her followers, which is accomplished by simultaneously utilizing their competence and personal attributes. The U.S. Army developed a model to depict the competencies (leads, develops, and achieves) and the attributes (character, presence, and intellect) of a trustworthy and effective leader. 7 In other words, leaders seek to master a set of teachable skills, or competencies, while simultaneously striving to develop the key personal attributes necessary for leaders to make effective decisions for his/her team. To lead in a variety of settings with various groups and goals, the leader ideally tailors his/her style to the situation. In their foundational work, Hersey and Blanchard proposed four leadership styles: telling/directing, selling/coaching, participating/supporting, and delegating. 8 This situational leadership model describes a framework dependent upon the nature of the assigned task, as well as the maturity level of the team members. They proposed that teams have their own level of internal maturity: unable and insecure, unable but willing, capable with low confidence, and capable and confident. 8
Given the variety of leadership styles, understanding the dynamics between a leader and their followers proves critical. Followership, a key component of effective teams, is defined as a series of individual characteristics, as well as a dynamic relationship between subordinates and their leaders. 9 The military has taken strides to incorporate followership into their professional military education (PME) with the understanding that leadership and followership are complimentary competencies critical to mission success. 10 Dr. Kelley’s landmark work on followership codifies followers into four quadrants based upon their passive–active completion of tasks and their level of dependent–independent thinking. 11 The four types of followers are characterized as: alienated, sheep, yes-people, and effective. For example, effective followers are self-starters who carry out their tasks with enthusiasm while possessing the ability to think critically in relation to the larger organizational structure and mission. More recently, Dr. Kelley introduced the concept of courageous conscience—the ability to make ethical and legal judgments and then to advocate on behalf of those judgments. 12 This concept has direct implications for team development in any health system, particularly in the military.
Tuckman’s seminal work provides a widely used model for understanding team development, with direct application to family medicine education and PME. He detailed the four stages of team development: forming, storming, norming, and performing. 13 Forming represents the group task of orienting to the team environment and beginning to develop boundaries. Once established, the “storming” of intragroup conflict develops from a lack of unity among group members. Norming occurs as group members resolve conflict and develop values and strategies for conflict resolution and group development. Finally, the performing stage is characterized by role clarity within the group and a consolidated effort towards a unified goal.
Team development model
The Air Force developed a model used in facilitating high-performance teams which incorporated types of leadership, stages of team development, and levels of team maturity; however, followership was not included. 14 A complementary model includes all four components (see Figure 2). This model is intended to help team members assess their own capacity using these components to facilitate team development and integration.
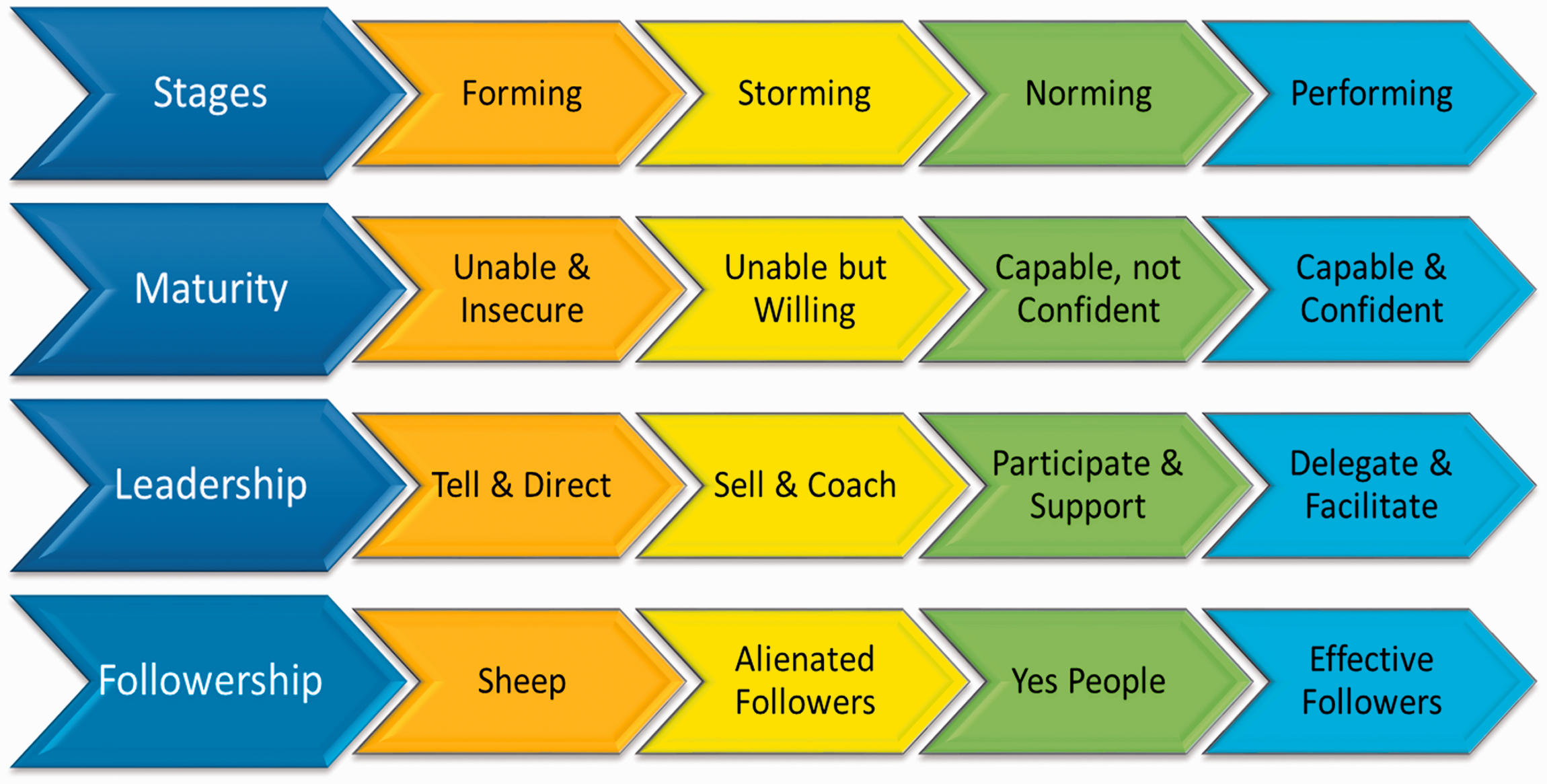
Team Development Model adapted from Office of Aerospace Studies High Performance Team (HPT) Facilitation Guidebook. 14
The following example illustrates how a team model plays out in a common family medicine residency activity. When a senior resident takes over an inpatient medical service team, he/she needs to determine in which stage the team is currently operating and the overall team maturity, which subsequently informs the leadership style to implement. The leader, in this case the senior resident, can then individually assess the type of followers within the group (interns, medical students, nurses, techs, etc.), their need for oversight, experience level, and degree of medical knowledge. For example, a team in the early stages of development may need specific directions from the senior resident and effective followers who can be used to help bolster the efficiency of the team. Followers can also use this model to determine if their performance and behaviors are in line with the team development and the requirements laid out by the team leader. Together, the leader and members of the team begin to collaborate more effectively and grow as a cohesive unit in pursuing their common goal of excellent patient care.
Understanding team dynamics and components is not enough for long-term development of a team—training is required. A euphemism exists in the military to “train as you will fight.” 15 Military teams develop and exercise team capabilities prior to being called upon to execute a real-world scenario. The structure of military exercises serves as a model for a team development approach in family medicine education. Many military exercises follow a five-step format: (1) establish objectives, (2) understand requirements, (3) prepare for situational, (4) execute training scenario, and (5) review performance. Several questions can guide this process and increase the utility of the training scenario: What is the objective? Are there limitations on how to achieve the objective? What are the responsibilities of each team member? What else is going on that can influence the outcomes? How should these instructions be communicated to team members? Once roles and responsibilities are assigned, then a training scenario can be developed where team members have a discussion about how each member of the team would respond given the specific scenario. 16 The team then develops contingency plans and responses to the changing scenario which mimic real-world situations requiring flexible reactions. Following the exercise or training scenario, leaders seek to understand the developmental level of their subordinate teams and their competencies through analyzing performance gaps. 17 This pattern can be replicated with family medicine training programs and clinics. Consistent, intense, and engaging training scenarios help to develop all aspects of the team and serve as a catalyst to team cohesion.
Application to family medicine teams
There are several key characteristics which exemplify a cohesive team: relationship-focused interactions, group competence and expertise, shared vision, purpose, and experiences, and team problem-solving. These characteristics can be examined among the many intraworkings of family medicine practitioners and staff. Relationship-focused interactions involve reciprocal communication and shared decision-making to optimize experiences and outcomes. 6 Within a medical team, exchanges of information, development of knowledge, and enhancement of skills demand a team effort and cannot occur in a silo. Group competence and expertise are the synergistic amalgamation of each team member’s knowledge and scope of practice. Rapid development of cohesive medical teams facilitates successful outcomes and high levels of productivity, particularly in austere, limited resourced environments. 18 Learning to respect the capabilities and expertise of each individual helps to establish group competence. Within a medical team, this may be clouded by the hierarchy of rank, position and distribution of power.
Team competence and expertise provides the foundational skills necessary to pursue a shared vision and purpose, which generally emerges from a group’s experience of the storming stage. Within family medicine residency programs, development of an explicit vision and stated purpose comes from several sources including the Program Director, Chief Resident(s), faculty, and other team members. A shared vision encourages team-based problem identification and problem-solving processes to achieve the vision and goals. Furthermore, collective efforts in problem-solving buffer the occupational burnout among physicians, which is a growing concern in primary care. 19
Cohesive medical teams are more likely to experience problem-solving success and subsequently good outcomes. However, it is not necessary that cohesion be achieved first. At times, the conflict of problem-solving creates a shared experience, which can force a leader to emerge, strategies to change, interactions to become more relationship focused, and the exhaustion due to chaos to make space for group competence and expertise. Upon settling the “storm,” the team “norm” can become trust within the group, interdependence, confidence in goal achievement, flexible communication, and resourcefulness. Such characteristics, among many others, positively impact functioning of medical teams, in and out of military environments, especially when resources (e.g., time, supplies, personnel) are limited.
Team development consists of four essential categories: effective leadership, followership, training, and team development traits. As already seen, the leader takes the predominant role in communicating the intent and goals, helps to ensure full organization of the team, and focuses on accomplishment. Followers on the other hand are responsible for individual initiative, ownership of outcomes, and interdependence. As organizations and groups engage in realistic training scenarios, they begin to meld into effective teams with traits such as shared purpose, cohesion, and adaptability. The components of leadership, followership, training, and team traits serve as guideposts for medical team development and expanding the ability of medical teams to provide high-quality patient care in an ever-changing environment.
Footnotes
Authors’ Note
The views expressed in this study are those of the author The views expressed in this study are those of the author and do not reflect the official policy and do not reflect the official policy or position of the United States Air Force, Department of Defense, or the U.S. Government.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.