
Abstract
Objective
Many patients with bipolar disorder are treated exclusively in primary care settings, and the use of atypical antipsychotics as primary treatment for bipolar depression is increasing. Extrapyramidal symptoms (EPS) are common side effects of antipsychotic medications, and clinicians should actively monitor for these symptoms when prescribing antipsychotic medications. Accurate diagnosis of EPS is especially important as the symptoms can be highly distressing, and in some cases, life threatening. Our aim is to familiarize primary care providers and other clinicians prescribing antipsychotic medications with EPS and to aid in its rapid diagnosis and treatment.
Method
We describe a case of lurasidone induced dystonia with prominent laryngospasm and oculogyric crisis which was missed for many years in the primary care setting, largely due to misdiagnosis of symptoms as being related to anxiety and panic attacks.
Results
In addition to summarizing this illustrative case, we present the most common forms of EPS and summarize the primary therapies for each type of EPS.
Conclusions
With increased management of bipolar disorder in the primary care setting and increased use of atypical antipsychotics as the primary therapy for bipolar disorder, it is essential that all practitioners are prepared to actively monitor for EPS, followed by its rapid diagnosis and treatment.
Keywords
Introduction
Bipolar depression can be a chronic and debilitating condition. First line treatments vary among practice guidelines, but generally consist of lithium, lamotrigine, valproate, and select atypical antipsychotics, either as monotherapy or in combination with each other or an antidepressant. 1 Though atypical antipsychotic medications are widely used as primary therapies for bipolar depression, 2 these medications can have a host of side effects, including hyperlipidemia, sedation, impaired glucose tolerance, metabolic syndrome, hyperprolactinemia, and extrapyramidal symptoms (EPS). 3
Atypical antipsychotics have a lower risk of EPS than typical antipsychotics, but the risk is still present.4–6 EPS are a common cause of poor adherence and discontinuation of antipsychotic medications, and can significantly impact quality of life, sometimes permanently, as in the case of tardive dyskinesia. 4 EPS can also be serious and life threatening. Examples include laryngospasm, leading to upper airway obstruction, 7 and akathisia, leading to agitation and increased risk of suicide. 8 Research has shown that patients with bipolar disorder and major depressive disorder are more vulnerable to developing extrapyramidal side effects than patients with schizophrenia, making monitoring for EPS important in this population.9,10 With antipsychotics being used more and more by non-psychiatric clinicians, recognizing and treating EPS is of the utmost importance. 11
Case presentation
A 40-year-old woman with a history of bipolar disorder was referred to the embedded psychiatrist in a primary care practice for the management of “panic attacks”. The woman noted that she had suffered from these attacks for the past four years, but they had become progressively worse. She called these episodes “I can’t breathes [sic],” as she would be short of breath during the episodes. At the time of the referral to psychiatry, she told her primary care team that she was having between five and seven episodes per week, accompanied by neck tightness. During these episodes she reported that her airway felt a different shape. These episodes had no precipitating triggers and were not preceded by anxiety or panic. Some episodes were accompanied by an uncontrollable urge to look up with her eyes, preventing her from looking at the horizon. During other episodes, her mouth would get stuck in the open position and her jaw would lock and feel as though it could dislocate. These episodes lasted as long as 10 hours. For milder episodes, she continued to go to work, though many episodes were painful and distressing and required her to call out sick from work.
Review of the patient’s chart noted that in addition to lurasidone for her bipolar disorder, she took methylphenidate 20 mg twice daily for attention deficit hyperactivity disorder, propranolol 10 mg twice daily as needed for anxiety, buspirone 15 mg three times daily for anxiety, and melatonin 10 mg nightly as needed for insomnia. Her other medical problems included obesity and polycystic ovarian syndrome. She had called or visited her primary care clinic several times with similar complaints since starting lurasidone 80 mg four years prior for treatment of bipolar disorder. Her dose of lurasidone had been increased to 100 mg, and later to 120 mg for treatment of residual depressive symptoms, as well as perceived anxiety related to the aforementioned episodes. She typically requested lorazepam for these episodes, and when her primary care team noted that she was going through 14 pills every 2 months, it was recommended that she work with her therapist on mindfulness techniques. As her symptoms progressed, she was referred to psychiatry for management of these episodes that were thought to be panic attacks.
At the time of the referral to psychiatry, the patient’s PHQ9 was noted to be 20, indicating severe depression, and her GAD7 was 18, indicating severe anxiety. 12 During the assessment with the psychiatrist, the patient described these “I can’t breathe” episodes as increasing in severity over the course of several years. The patient reported low dose diphenhydramine was sometimes helpful in episodes in which only breathing was affected, but was not helpful once her eye motion or jaw was affected. She specifically reported that the episodes often occurred when she was calm and that the episodes were not accompanied by hyperventilation. The psychiatrist made the diagnosis of acute dystonia with prominent lurasidone induced laryngospasm and oculogyric crisis. The patient was advised to rapidly taper off lurasidone and was prescribed benztropine 1 mg twice per day, and diphenhydramine 50 mg as needed for residual symptoms of dystonia. She was advised to go immediately to the emergency department if these symptoms recurred given the seriousness of laryngospasm and oculogyric crisis. Fortunately, these episodes resolved immediately with the prescribed treatment. She was ultimately managed on a combination of lithium and valproate to treat bipolar disorder, and while her symptoms of depression remained severe, (PHQ9 of 19), her anxiety improved to a GAD7 of 8, indicating mild anxiety. She had no recurrence of EPS. The patient provided written informed consent for the publication of this case report.
Discussion
According to the Naranjo Adverse Drug Reaction Probability Scale, this case describes a probable adverse drug reaction of acute dystonia, with prominent laryngospasm and oculogyric crisis. The reaction is considered probable because 1) this reaction is a known side effect, 2) followed a temporal and dose responsive sequence, 3) improved with withdrawal of lurasidone and administration of benztropine and diphenhydramine, and 4) couldn’t reasonably be explained otherwise by the patient’s clinical state. 13
This case highlights a common treatment course, as the use of atypical antipsychotics as primary treatment for bipolar depression is increasing. 2 Lurasidone in particular has many advantages in the treatment of bipolar depression. Ostacher et al. conducted a systematic review of lurasidone compared to other atypical antipsychotics as monotherapy for bipolar depression and found it to be more efficacious than aripiprazole and ziprasidone, have less weight gain than quetiapine and olanzapine, and have similar rate of EPS and similar rates of discontinuation. 14 There is evidence that the risk of EPS differs between patients with schizophrenia compared to patients with bipolar disorder, with Gao et al. noting that there was a higher risk of EPS for patients with bipolar disorder compared to patients with schizophrenia. Specifically, Gao et al. noted differences among atypical antipsychotics and their EPS risk, noting higher risk of EPS with ziprasidone or quetiapine compared to other antipsychotics, and a higher risk of akathisia with patients with bipolar disorder taking aripiprazole. 10
Currently, 10% to 38% of patients with bipolar disorder are being treated exclusively in primary care settings due to barriers accessing specialty mental health services. 11 There are several advantages to this, including increased appointment availability for patients, long term relationships with providers, and decreased cost barriers to access care. 15 However, in prescribing antipsychotics, it is important for providers to be aware that EPS are side effects of atypical antipsychotics, and that patients with bipolar disorder are at increased risk of these side effects, and therefore caution must be used in prescribing this choice of treatment. 10 Our aim is to familiarize primary care providers with EPS to aid in its rapid diagnosis and treatment.
When prescribing atypical antipsychotics, in addition to routine monitoring of metabolic symptoms (e.g. weight gain, hyperlipidemia, hypertension, fasting glucose, and hemoglobin A1C), routine monitoring for EPS is important. 16 EPS include acute dystonia (muscle spasms, rigidity, and abnormal postures, typically of the neck, tongue, face, and back), akathisia (restlessness, anxiety, and pacing), parkinsonism (rigidity, tremor, and bradykinesia), and tardive dyskinesia (involuntary repetitive facial movements, buccal and tongue motions, as well as torso and limb movements).4,17 Acute EPS of dystonia, akathisia, and parkinsonism can be recognized by their time course (symptoms tend to occur within days to weeks of starting an antipsychotic or with increased dose of an antipsychotic), as well as by subjective descriptions of symptoms and objective findings of movements on exam. 4
Evaluation for EPS should take place every three to twelve months, as well as when adding or increasing the dose of an antipsychotic. Determining the spacing of these assessments is typically based on patient risk factors such as an individual patient’s history of EPS. There are several commonly used rating scales for EPS that can assist in objective monitoring for the development or worsening of EPS, including the Simpson-Angus Scale (SAS) for parkinsonism, the Barnes Akathisia Rating Scale (BARS) for akathisia, and the Abnormal Involuntary Movement Scale (AIMS) for tardive dyskinesia. The Drug-Induced Extrapyramidal Symptoms Scale (DIEPSS) is a combined rating scale for parkinsonism, dystonia, dyskinesia, and akathisia and might be a good choice to ensure that thorough evaluations of EPS take place regularly and efficiently. 18 Any trained healthcare provider can administer most EPS scales, and these scales can be used for any patient, regardless of psychiatric diagnosis. Of note, the score must be taken in context with the patient’s history, as the scales are often not linear. 19 The emergence or worsening of EPS should prompt treatment consideration, and if possible, medication adjustments or dose reductions, as described in detail below.
One challenge of EPS diagnosis is that there can be significant overlap between EPS and anxiety, with muscle tightness, restlessness, irritability, agitation, anxiety and difficulty breathing commonly seen in both scenarios. 17 In the case above, the patient’s description of oculogyric crisis, forced jaw opening, and laryngospasm were misinterpreted as symptoms of a panic attack. When assessing symptoms of anxiety in patients taking antipsychotic medications, it is important to first rule out EPS. Oculogyric crisis (upward, involuntary movement of the eyes) and trismus (forced jaw opening) should immediately alert the clinician that the patient is having a dystonic reaction, as these are not commonly seen in patients with anxiety disorders. Laryngospasm can be harder to diagnose, as the patient often presents with “shortness of breath” as their chief complaint, which has a lengthy differential diagnosis, including panic attack. In the case above, clues that the shortness of breath was due to laryngospasm rather than anxiety include the absence of other symptoms of anxiety during these episodes, and a sensation of tightening around the vocal cords. Laryngospasm is particularly important to correctly diagnose, as it can lead to dysphonia, stridor, and respiratory distress, and in severe cases hypoxia and death.7,20
Akathisia, in particular, can often be difficult to differentiate from anxiety. Patients struggling with akathisia often describe either a feeling of wanting to crawl out their skin or an inability to sit still. Though these symptoms can also be seen in patients with anxiety, there should be a high suspicion for akathisia in any patient developing these symptoms after starting or increasing the dose of an antipsychotic medication. These symptoms can often come in the absence of cognitive symptoms of anxiety (such as worry thoughts), or other physiological symptoms of anxiety (such as chest pain, diaphoresis, and tachycardia). 21
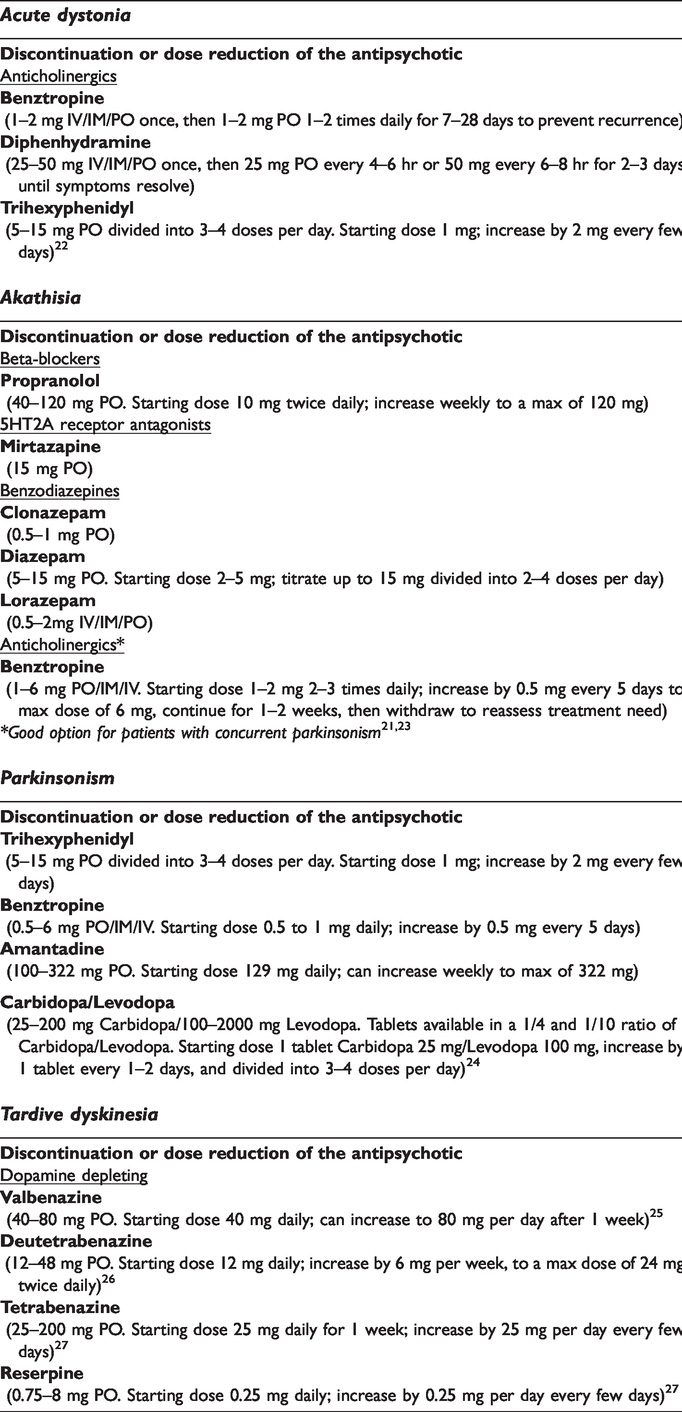
The first step in the treatment of any type of EPS is dose reduction or discontinuation of the offending agent, or a switch to an alternative therapy less likely to induce EPS. However, this decision is patient specific, and is often influenced by the efficacy of alternative therapy options, as well as the possibility of worsening psychiatric symptoms. In addition, each variant of EPS has specific treatments (see Table 1). Acute dystonia typically responds to administration of anticholinergic agents such as benztropine or diphenhydramine.20,22 When the dystonia is severe or life threatening, it is recommended that the anticholinergic agent be administered intravenously. 7 First line treatments for akathisia are generally propranolol, benzodiazepines, or mirtazapine, though anticholinergic agents are also an option if akathisia is accompanied by parkinsonism.21,23 Parkinsonism can be treated with anticholinergic agents or dopamine agonists, though there is a risk of worsening psychosis when initiating a dopamine agonist, and therefore anticholinergic agents are generally preferred.20,24 Tardive dyskinesia is generally considered to be irreversible, unless caught and treated early, in which case some cases do remit. First line treatments for tardive dyskinesia include dopamine-depleting medications such as valbenazine, deutetrabenazine or tetrabenazine.25–27
Extrapyramidal symptoms: treatments and management.
Conclusion
EPS is a common side effect of antipsychotic medications, and clinicians should actively monitor for these symptoms when prescribing antipsychotic medications. Accurate diagnosis of EPS is especially important as the symptoms can be highly distressing and, in some cases, life threatening. With increased management of bipolar disorder in the primary care setting and increased use of atypical antipsychotics as primary therapy for bipolar disorder, monitoring for EPS, followed by rapid diagnosis and appropriate treatment, is essential.
Footnotes
Declaration of conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.