
Abstract
Objective
The present study aimed to understand how key risk factors of older adult suicide interact to ultimately lead to death by suicide using data collected post-mortem.
Method
A psychological autopsy was used to gather detailed information about psychiatric diagnosis, medical problems, social isolation, and negative attitudes expressed by the individual during the six months prior to their death. Interviews with next-of-kin, medical and psychiatric records, and the Cumulative Illness Rating Scale for Geriatrics were used. Subjects included 32 older adults who died by suicide and 45 older adults who died by natural causes.
Results
Hopelessness, depression, and negative health attitudes were strongly correlated with suicide. Older age was associated with social isolation, suggesting an indirect relationship with suicide via hopelessness, depression, and negative health attitudes. Physical illness did not increase risk. Multivariate analyses suggested that hopelessness fully mediated the effects of social isolation, negative health attitudes, and depression on suicide.
Conclusions
Psychological factors played the largest role in suicide deaths compared to social isolation and physical illness. Suicide interventions aimed at older adults should ensure hopelessness, depression, and negative health attitudes are primary targets.
Introduction
Older adults are at a heightened risk of dying by suicide. 1 In the US, adults between the ages of 45–54 years (20.2 per 100,000) and 85+ years (20.1 per 100,000) are the most at-risk age groups. 2 Individuals between 55 and 84 years of age remain at a relatively high risk, with the rate only dipping to 15.19 for 65–69 year olds.
Depression and hopelessness are established indicators of suicide risk across the life span. 3 Depression is associated with an increased likelihood of dying by suicide 4 and hopelessness further increases suicide risk. 5 In a study spanning over 13 years, hopelessness was most strongly associated with death by suicide compared to suicide attempts and suicidal ideation, even after controlling for sociodemographic factors and psychiatric diagnoses. 6 For older adults who died by suicide, expressing hopelessness and having a history of suicide attempts were stronger predictors than psychiatric illness. 4 Hopelessness was the most significant factor (OR = 7.25) in older adults who died by suicide compared to controls in a multivariate model that included depression (OR = 6.70) and loneliness (no independent effect). 7
Social isolation is associated with suicide risk in older adults 8 even after controlling for psychological conditions. 9 Perceived social isolation rather than social disconnectedness appears to be responsible for the most deleterious outcomes. 10 Moreover, older adults are specifically affected by factors related to isolation such as being widowed or not married, 11 living alone, and having poor social support. 12 Older adults who are more isolated than younger individuals have a reduced likelihood of rescue or risk detection 13 and heighted feelings of loneliness, further increasing the probability of suicide. 14 Including social isolation in a model of older adult suicide might add an age-specific factor and provide additional modifiable treatment targets.
Physical illness is another salient risk factor for older adults, even after controlling for psychological conditions. 15 A significant proportion of older adults receive healthcare services a month prior to dying by suicide and a large proportion complete a healthcare visit within that same year. 16 Physical decline also increases the likelihood that a given attempt will be fatal, 17 while negative perceptions of health further intensify risk. 18 Although specific medical diagnoses are related to greater risk, 11 the cumulative effect of comorbid diseases may be a more useful indicator in older adults. 19 When physical illness results in significant impairment, the likelihood of experiencing a suicidal crisis due to feelings of desperation and hopelessness increases. 20 Moreover, the subjective perception of one’s health, rather than medical illness itself, may be what increases late-life risk. 21 It remains unclear whether physical illness independently affects suicide risk, whether it is the individual’s perception of health, or if perceptions of health are moderated by depression, social isolation, or other negative consequences.
Despite their increased risk of dying by suicide and the number of risk factors associated with advanced age, older adults remain underrepresented in suicide research. 4 The present study was designed to explore how hopelessness, depression, social isolation, and physical illness interact with advanced age to distinguish between those who died by suicide and natural causes. It was predicted that older adults who died by suicide were significantly more hopeless and depressed than those who died by natural causes. It was also predicted that social isolation, physical illness, depression, and hopelessness would be closely related. Finally, analyses examined a model to clarify the way in which physical illness might be related to suicide in older adults.
Method
Sample
Next-of-kin of 451 individuals who died between the years 1989 and 2015 in Cuyahoga County, Ohio, were asked to participate in the study and the cases were assessed using psychological autopsy procedures. All individuals were processed through the county medical examiner's office, which determined cause of death. Written informed consent was obtained from the legally-defined next-of-kin (study approved by the University Hospitals Cleveland Medical Center IRB #11–88-233). Among the full sample, age ranged from 15–92 years (M = 48.61). For the present study, cases of individuals who were 65+ years of age and died by suicide (n = 32) or natural causes (n = 45) were selected, yielding a total of 77 older adults (M = 74.25, 63.6% male, 85.7% Caucasian).
Measures
Demographic information (e.g., age, sex, race, marital status, cause and location of death) was obtained from the medical examiner's autopsy report. Additional information (e.g., education, employment status, living conditions, prior suicide attempts) was provided by family members. Presence of substances at time of death was assessed via the autopsy toxicology screen.
Structured diagnostic interviews with family members were conducted to determine the most accurate psychiatric diagnosis at time of death using DSM-IV diagnostic criteria. 22 Most cases (n = 41) relied on the Structured Clinical Interview for DSM-IV, 23 while the remaining cases (n = 34) were based on the Schedule for Affective Disorders and Schizophrenia. 24 Two cases were missing the diagnostic interview, but enough information was present to be included in the study. Psychological autopsy research has supported proxy diagnosis completed with family members when compared to diagnosis based on medical records (κ = 0.67 overall sample, κ = 0.63 for MDD) 25 and when completed between depressed patients and family members (MDD κ = 1.00). 26
Four separate severity rating scales were scored by a trained researcher after reviewing all materials describing each case. The Depression Severity Rating was based on the number and intensity of symptoms reported during the diagnostic interview. The Hopelessness Severity Index was adapted from attitudes expressed in the Beck Hopelessness Scale. 27 The Negative Attitude Severity Index was derived from the Cognitive Triad Inventory 28 to assess a global sense of negative attitudes. The Social Isolation Severity Index was based on the UCLA Loneliness Scale 29 and the short scales for emotional and social loneliness, 30 and included estimates of subjective (perceived social isolation) and objective (social disconnectedness) dimensions of isolation. Each severity rating scale ranged from 0 (not at all) to 155 (very much) based on the degree to which supporting evidence was found in all records.
The Cumulative Illness Rating Scale for Geriatrics (CIRS-G)31,32 evaluates 13 organ-specific categories (e.g., heart, vascular, respiratory) and can be completed through chart review. 33 The CIRS-G has good agreement, with intra-class correlations (ICC) between 0.81–0.83 for number of categories endorsed that represent a current physical problem. 31 The CIRS-G was used to assess the presence of aggregate physical problems through chart review and the autopsy report.
Procedure
Psychological autopsy procedures were used to reconstruct a person’s state-of-mind prior to death through the integration of information from interviews with knowledgeable informants, known life circumstances, and available records. 34 Mental health professionals with expertise in post-mortem work conceptualize each case until a consensus is reached. 35 Psychological autopsies are reliable and valid for determining psychological diagnoses 26 and psychological states 36 of individuals who have died by suicide. As recommended for psychological autopsy research, 37 the present assessment included structured interviews with family members, medical examiner’s report, police report, suicide notes, prior medical and psychiatric records, and autopsy toxicology results.
A master’s level social worker with extensive experience conducting diagnostic interviews conducted in-home interviews with next-of-kin 8–12 weeks after the death. For each decedent, an integrative report summarized all available information. Final diagnosis was based on the consensus of the diagnostic team, which included a board-certified psychiatrist, a board-certified clinical psychologist, a doctoral-level neuroscientist, and the master's-level social worker who conducted the interviews.
The severity rating scales were coded by two research assistants trained in psychological autopsy research. All records were reviewed prior to scoring the severity scales. A random subset of cases (n = 18, 23.4%) was coded independently by the two members of the research team to calculate inter-rater agreement on the severity scales. Due to the nature of the psychological autopsy method as a review of records, it was not possible for raters to be blinded to cause of death.
Intra-class correlation coefficients were used to assess inter-rater agreement on continuous variables of hopelessness, depression, social isolation, negative attitude, and physical illness. Coefficients were based on a single-rater, consistency, two-way random-effects model. Chi-square tests were used for descriptive group comparisons by cause of death and correlations were used to assess the strength of relationships between social isolation, depression, hopelessness, and physical illness. Structural equation modeling (SEM) was used to assess hypothesized paths. A p-value < .05 was considered significant across all analyses.
Results
Several significant differences were found between individuals who died by suicide and individuals who died by natural causes (Table 1). The suicide group had a higher percentage of males as compared to the natural death group, χ2 (1, N = 77) = 10.18, p = .001. Individuals who died by suicide were more likely to meet criteria for a psychiatric disorder at time of death than natural death cases, χ 2 (1, N = 76) = 34.15, p < .001, with a high rate of depressive disorders (87.5%). A history of lifetime psychiatric treatment (χ 2 [1, N = 76] = 6.59, p = .010) and suicide attempts (χ 2 [1, N = 76] = 8.48, p = .004) were also more likely within the suicide group. Based on toxicology screening at time of death, the groups were not significantly different in terms of prescription medications or recreational substances (χ 2 [1, N = 72] = 3.46, p = .063), although the natural death group displayed a higher rate of clean toxicology screens (33.3%) compared to the suicide group (12%). Similarly, there was no significant difference between groups in the presence of psychotropic medications (χ2[1, N = 73] = 3.24, p = .072) and only one person was prescribed an antiepileptic mood stabilizer. Additional analyses found no significant differences between the two groups in terms of assorted prescription medications (antidepressant, antipsychotic, mood stabilizers, and anxiolytic) or recreational drugs (alcohol, marijuana, cocaine, and opiates).
Comparison of suicidal cases versus natural deaths on background variables.
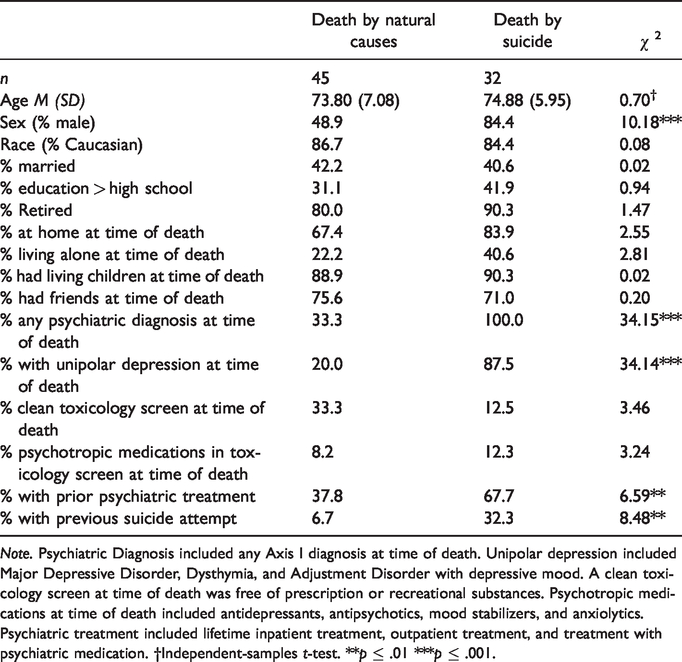
Note. Psychiatric Diagnosis included any Axis I diagnosis at time of death. Unipolar depression included Major Depressive Disorder, Dysthymia, and Adjustment Disorder with depressive mood. A clean toxicology screen at time of death was free of prescription or recreational substances. Psychotropic medications at time of death included antidepressants, antipsychotics, mood stabilizers, and anxiolytics. Psychiatric treatment included lifetime inpatient treatment, outpatient treatment, and treatment with psychiatric medication. †Independent-samples t-test. **p ≤ .01 ***p ≤ .001.
Inter-rater agreement was adequate for all four severity rating scales. Strong inter-rater agreement was found for the Depression Severity Rating (ICC = 0.87, 95% CI 0.69–0.95, p < .001), Hopelessness Severity Index (ICC = 0.83, 95% CI 0.57–0.94, p < .001), Negative Attitude Severity Index (ICC = 0.81, 95% CI 0.57–0.93, p < .001), and Social Isolation Severity Index (ICC = 0.94, 95% CI 0.85–0.98, p < .001). Number of physical illness categories present reached near-moderate agreement (ICC = 0.54, CI .11–0.80, p = .008).
The Depression and Hopelessness Severity Indices differentiated the two groups (see Table 2). Individuals who died by suicide were more severely depressed (t [75] = 6.90, p < .001) and hopeless (t [55.46] = 14.77, p < .001) than those who died by natural causes. Severity of social isolation and physical illness were not significantly different between the two groups.
Cases of suicide and natural death compared on depression severity, social isolation, hopelessness, negative attitude about physical health, and physical illness.
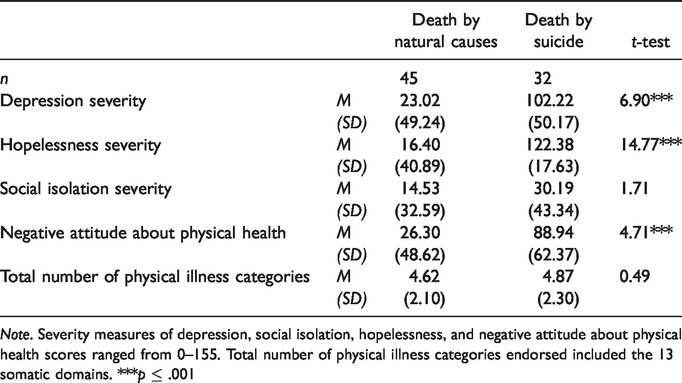
Note. Severity measures of depression, social isolation, hopelessness, and negative attitude about physical health scores ranged from 0–155. Total number of physical illness categories endorsed included the 13 somatic domains. ***p ≤ .001
To parse out the physical and psychological aspects of physical health, cases were scored as to whether or not problems with physical health was a factor contributing to the Negative Attitude Severity Index. The Negative Attitude about Physical Health Severity Index was significantly different from the Negative Attitude Severity Index (χ2[1, N = 75] = 29.50, p < .001) and the Hopelessness Severity Index (χ2[1, N = 72] = 25.73, p < .001). Comparisons suggested the new variable captured a different construct tapping into a subjectively low view of one’s health trajectory despite the objective presence or absence of physical illness. Compared to cumulative physical illness, individuals who died by suicide had more negative attitudes about their health than those who died by natural causes, t (56.80) = 4.71, p < .001.
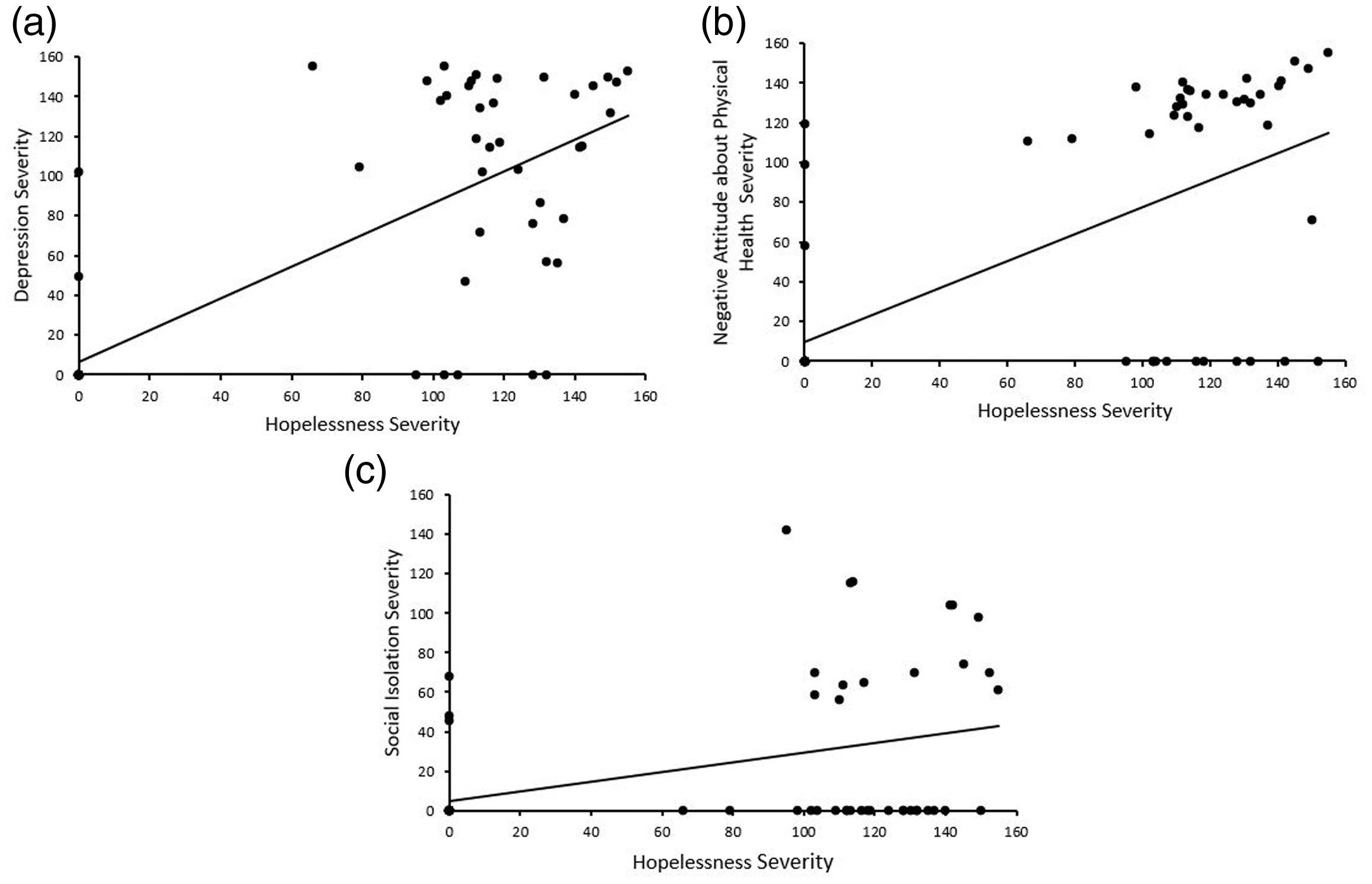
Older age was moderately associated with more severe social isolation (r = .39, p < .001) and a greater range of physical illnesses (r = .25, p = .03). Death by suicide was strongly associated with more severe depression (rpb = 0.62, p < .001) and hopelessness (rpb = 0.85, p < .001). Social isolation was moderately associated with depression (r = .29, p = .011) and hopelessness (r = .42, p < .001), and depression was significantly associated with hopelessness (r = .78, p < .001). Physical illness was not significantly correlated with any of the other severity measures. In contrast, a negative attitude about one’s health was associated with death by suicide (rpb = .50, p < .001), depression (r = .66, p < .001), social isolation (r = .27, p = .018), and hopelessness (r = .66, p < .001). Negative attitude about health was not significantly associated with age (p = .684). See Figures 1(a) to (c) for scatterplots displaying key correlations between variables associated with hopelessness.
Structural equation modeling was used to assess the relationships between the risk factors and death by suicide. The maximum likelihood method was used to evaluate measurement model fit and handle missing data. Absolute and relative fit indices were employed to determine goodness of fit. The final model was constructed based on hypothesized relationships between the variables that showed significant correlations (see Figure 2). The model had acceptable fit to the data (χ2[1, N = 77] = 10.84, p = .211, RMSEA = .07, CFI = 0.99, TLI = 0.95, and NFI = 0.96) and explained 71% of the variance in death by suicide.
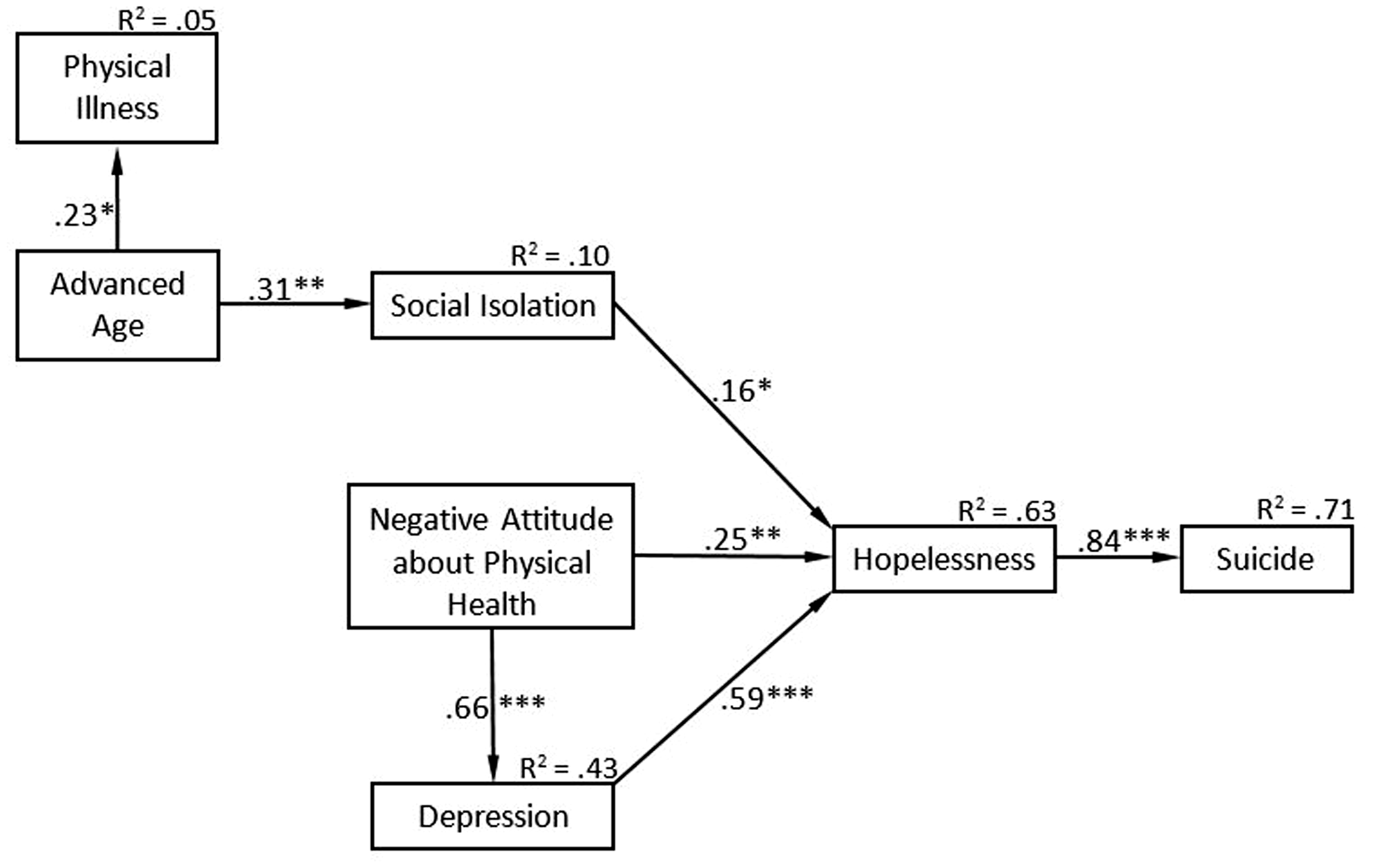
The relationship between advanced age and death by suicide mediated by social isolation, negative attitude about physical health, depression, and hopelessness examined by structural equation modeling. Only significant paths were included in the final structural model that is shown in the figure. Values above variables (R2) indicate proportion of the variance in the dependent variable explained by the independent variables. Values above paths indicate standardized estimates (β). *p ≤ .05 **p ≤ .01 ***p ≤ .001.
As Figure 2 illustrates, hopelessness was the only variable directly associated with death by suicide (B = .01, β = 0.84, Standard Error [SE] = 13.31, p ≤ .001). Hopelessness operated as a full mediator between depression and suicide (B = 0.55, β = 0.59, SE = .09, p ≤ .001), negative health attitudes and suicide (B = .24, β = .25, SE = .09, p = .009), and social isolation and suicide (B = .25, β = .16, SE = .11, p = .024). That is, more severe depression, more negative health attitudes, and more severe isolation were significantly associated with more severe hopelessness, indirectly contributing to death by suicide via increased hopelessness. Additional analyses revealed that making hopelessness a non-mediator resulted in a poorly fitting model, while eliminating hopelessness altogether resulted in a model that only explained 40% of the variance in death by suicide. Model comparisons provide additional evidence for the mediating role of hopelessness in death by suicide.
Further examination of Figure 2 revealed that depression severity partially mediated the relationship between negative health attitudes and hopelessness. More negative health attitudes were associated with more severe hopelessness through its significant association with depression severity (B = 0.66, β = 0.66, SE = .09, p ≤ .001), as well as its direct relationship to hopelessness severity (B = .24, β = .25, SE = .09, p = .008). Lastly, older age was directly related to more physical illnesses (B = 1.00, β = .23, SE = .45, p = .045) and indirectly related to hopelessness via social isolation (B = 23.36, β = .31, SE = 8.32, p = .005). Thus, older age indirectly contributed to more severe hopelessness through greater levels of social isolation.
Discussion
Despite being a high-risk group, few evidence-based interventions have been developed for the prevention of older adult suicide. 38 Unlike other studies that have examined suicide risk in individuals who have reported recent suicidal thoughts or suicide attempts, the current findings are useful because they examined psychosocial factors in a sample of older adults who died by suicide using well-established psychological autopsy methodology. More specifically, the current study extended beyond the examination of group differences or independent associations to cause of death by examining the relationships between key factors related to late-life suicide. Overall, the results support prevalent theories of suicide (e.g., Interpersonal Theory of Suicide, 39 Three-Step Theory 40 ): negative perceptions of the future (hopelessness), self (depression, health attitudes), and others (social isolation) appear to play an active role in the suicidal process that culminates in death.
Consistent with previous findings, the current study highlights the central importance of depression 41 and hopelessness 7 in suicide risk among older adults. Depression was a significant contributing factor in older adult suicide and was associated with social isolation and negative self-perceptions of health. As a basic precursor, depression appears crucial in the development and maintenance of a desire to die 42 and should remain a core aspect of prevention and intervention. However, simply targeting depression is likely insufficient to achieve clinically significant change in suicidal thinking among older individuals. 43 As in prior studies,4,7 hopelessness was the strongest factor associated with death by suicide. Multivariate analyses suggested that hopelessness fully mediated the relationships between established risk factors, including depression. The hopelessness experienced by suicidal older adults appears to be driven by low mood, perceptions of poor physical health, 44 and to a lesser extent, social isolation. 7 In addition to targeting depression, specifically focusing on hopeless cognitions may yield greater effectiveness in reducing suicide risk. 45 The present study also supports the use of a new hopelessness severity rating that can be used in proxy-based assessments.
Contrary to prediction, accumulation of physical health problems had minimal impact on suicide risk for older adults. More than actual illness, negative self-perceptions of health differentiated older adults who died by suicide from those who died by natural causes. Although individuals with more advanced age had more health problems, a negative health attitude was the third-strongest factor after hopelessness and depression. The apparent distinction between perceived and actual physical illness provides a window of opportunity for mitigating risk. Primary care is more widespread than mental health care among older populations, placing providers in a unique position to help identify vulnerable older adults. 16 Education on prognosis and disease management, patient involvement in care, and promotion of healthy behaviors may be specific ways in which health providers can help improve pessimistic health attitudes. Moreover, training medical providers in the screening of depression and suicide can increase detection of at-risk individuals. 16 Programs integrating primary and mental health care are among the most effective in reducing suicidal ideation in depressed older adults. 38
As in previous research, social isolation appears to be indirectly associated with suicide through depression, 46 as well as negative health attitudes and hopelessness. 7 Thus, social isolation may be better described as a precursor or consequence of poor psychological health that contributes to suicide risk. Additionally, more advanced age minimally contributed to risk by its association with social isolation, including reduced social support due to widowhood and having no living children at time of death. Increasing a sense of connection with others may help alleviate the negative consequences depression and hopelessness have on late-life suicide risk.
Psychological autopsies are based upon structured interviews with family members and rely on detailed records from police and health care professionals. Moreover, due to the heavy reliance on narrative of the records, blinding to cause of death was not possible. It may be that the non-blinded nature of the study design played a role in how raters scored the measures. Nonetheless, raters were trained to identify and score specific variables relevant to the study and displayed a strong level of inter-rater agreement. Additionally, the heterogeneous quality of medical records in the present study created difficulties for scoring the CIRS-G. Furthermore, several new rating scales were developed for scoring psychological variables from comprehensive records. Although inter-rater agreement was high, the severity measures were scored as zero when the problem was deemed absent, resulting in a skewed distribution of scores. The present findings should be viewed with caution in light of these limitations.
The present study provides supporting evidence for the strong impact hopelessness had on older adults who died by suicide compared to older adults who died by natural causes. The finding that hopelessness was one of the most significant factors is actually hopeful for prevention efforts, as it is amenable to significant therapeutic change through primary-care based programs, 38 a range of psychotherapies, 47 and phone counseling 44 specific to this population. Although depression, negative health perceptions, and social isolation were also significant factors to varying degrees, hopelessness appeared to mediate their relationship to death by suicide. Additionally, physical illness did not account for any variance in suicide deaths, further illustrating the potency of negative cognitions in suicidal behaviors. Prevention efforts are likely to see greater effectiveness when hopelessness, depression, and perceived health status are targets for intervention. 48
Footnotes
Acknowledgements
Portions of this paper were presented at the Gerontological Society of America Scientific Meeting in Austin, TX (November, 2019) and at the Aging in America Conference in New Orleans, LA (April, 2019).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Center of Biomedical Research Excellence (COBRE) grant from the National Institutes of Health IDeA Program (grant number P30 GM103328).