
Abstract
Objectives
Medication non-adherence is one important reason behind sub-optimal outcome from treatment of bipolar affective disorder (BPAD). Though various reasons behind medication non-adherence have been identified, little is known about the medication adherence patterns across various predominant polarities (PP) in BPAD.
Methods
100 euthymic patients of BPAD were purposively recruited and the PP were determined. Subsequently, Morisky Medication adherence scale (MMAS); Global Assessment of Functioning (GAF); Oslo Social Support Scale and World Health Organization Quality of Life scale- Brief version (WHOQOL-Bref) were administered. Analysis of covariance (ANCOVA) was done to estimate the difference of scores of MMAS after adjusting for any potential confounders.
Results
Overall, 44 patients with manic PP (MPP), 17 with depressive PP (DPP) and 39 with indeterminate PP (IPP) were recruited. It was found that patients who presented with DPP showed significantly higher medication adherence as compared to MPP.
Conclusion
Knowledge of PP of a patient of BPAD can be useful in anticipating medication adherence and treatment outcome. The major limitations included non-probability sampling, cross-sectional design and limited generalizability of the results.
Introduction
Bipolar affective disorder (BPAD) is a chronic disorder usually with an episodic course, causing significant morbidity to the patients. This disorder is usually characterized by the occurrence of multiple episodes of either manic/hypomanic episodes (characterized by euphoric or irritable mood state, increase in psychomotor activities and other symptoms) or depressive episodes (characterized by low mood, anhedonia, anergia and other symptoms), often with good inter-episodic remission. The treatment of this disorder largely involves controlling the index mood episode and also prevention of relapse by use of prophylactic medicines, commonly referred to as mood stabilizers. Over the past years, the treatment of BPAD has been fortified with the advent of a number of evidence-based treatments. However, in-spite of that, the outcome of the treatment often leaves a lot to desire. One of the major issues pertaining to the sub-optimal response to pharmacotherapy is medication adherence. 1 Medication adherence is defined as ‘the degree to which a patient’s behavior matches agreed-upon recommendations from a prescribing clinician’ 2 The prevalence of medication non-adherence has been found to be ranging between 20-60% in the past studies.3–6 The variety in the range is largely attributed to difference of the study population, tools used in the measurement and recall methods. However, the significant burden arising out of medication non-adherence was ubiquitous across studies.
The reasons behind non-adherence to medication have received substantial attention from the researchers. A number of patient-level barriers like young age, being single, poor social support, more severe symptoms, high frequency of affective episodes, other medical or psychiatric comorbidity etc. have been identified. 7 In addition, a number of external barriers were also identified in the studies like poor side-effect profile, complex treatment regime, choice of medication and stigma. 8 Various factors arising out of the disorder has also been implicated for treatment non-adherence. Various studies in the past had found that bipolar I subtype, suicidality or presence of psychotic symptoms were more likely to be treatment non-adherent.9,10
Till now, the most common approach to study this problem has been to compare medication adherence in BPAD with other severe mental illnesses, most commonly schizophrenia. But, BPAD in itself, is a complex disorder and further research needs to be invested in delineating the various sub-types in BPAD. Predominant polarity (PP) is one such sub-type that garnered our interest by allowing classification of patients of BPAD by predominance of one polarity of affective episodes over the longitudinal course of the illness. Though there are variety of definitions, the stricter criterion deducts that, if two-thirds of the episodes in a patient of BPAD are of a particular polarity, the PP of that patient is the corresponding PP. 11 Patients with two-third majority of manic episodes are classified as manic PP (MPP); whereas patients with two-third majority of depressive episodes are classified as depressive PP (DPP). But, if neither manic nor depressive episodes gain two-thirds predominance in the course the patients is classified as indeterminate PP (IPP).
Our current understanding tells us that patients of various PP can vary from each other in terms of their cognitive functioning, 12 temperament or internalized stigma 13 ; basically allowing us to predict important clues in the further course of the patient. However, no study has been conducted about the patterns of treatment adherence in various PP in patients of BPAD. This information could also become important in the background of the fact that prescription patterns in various PP is unique. 14 Studies till now have shown that the medication adherence can vary according to the types of medication, pill burden and perceived side-effects. 15 Thus, it will be extremely beneficial for a clinician in decision-making to have the knowledge of when to expect medication non-adherence. With this background, the current study was conducted to compare medication adherence in euthymic patients of BPAD across the PP of their treatment regimen.
Methodology
The current study was conducted in a tertiary center from Eastern India. The study obtained ethical clearance from the institute ethics committee. 100 patients of BPAD in remission were purposively sampled if they adhered to the inclusion criteria. The inclusion criteria were i) aged above 18 years, ii) presenting with a reliable informant, iii) able to converse and comprehend in English, Hindi or Bengali to the level of primary education and iv) willing to provide written informed consent. Remission of BPAD was defined as absence of clinically significant mood symptoms, current Young Mania Rating Scale score of <5, Hamilton Rating Scale for Depression score of <8 and no change in maintenance medication by more than 50% or hospitalization in the past 2 months. 16 Subjects were not recruited if clinical information is inadequate.
The study was conducted using a cross-sectional design with patients being recruited after fulfilling the inclusion criteria. They were then administered a semi-structured questionnaire to collect data regarding socio-demographic and clinical variables. Subsequently, all the tools mentioned as follows were administered: a) Morisky Medication adherence scale (MMAS) 17 - an 8-item self-reported measure of treatment adherence; b) Global Assessment of Functioning (GAF) 18 - a numeric scale used by mental health clinicians and physicians to rate subjectively the social, occupational, and psychological functioning of an individual; c) Oslo Social Support Scale 19 - a 3-item scale with scores ranging from 3–14 with higher scores indicating higher social support and d) World Health Organization Quality of Life scale- Brief version (WHOQOL-Bref) 20 - an international cross-culturally comparable quality of life assessment instrument comprising of 26 items and 4 domains.
The statistical analysis was conducted using the SPSS version 24. Descriptive statistics were compiled. Test for Normality was done by Kolmogorov Smirnov test. Recruited subjects were divided into three PP based on two-third predominance as per the criteria given by Colom et al. 11 Comparisons of socio-demographic and clinical variable were done using chi-square-test (for categorical variables) and one-way analysis of variance for continuous variables (ANOVA) (Kruskal-wallis test for non-parametric data) between the three predominant polarities. Subsequently, analysis of covariance (ANCOVA) was done to estimate the difference of scores of MMAS after adjusting for any potential confounders. The level of significance was kept at 5%.
Results
Overall, in our study, 100 euthymic patients were recruited of which there were 44 patients with MPP, 17 with DPP and 39 with IPP. Table 1 shows the comparison of the various socio-demographic and clinical parameters in the three groups. It was found that the patients with MPP had a significantly lower age; higher percentage of patients being not married (being single or divorced) and lower total duration of illness and duration of seeking treatment.
Comparison of socio-demographic and clinical variables across various predominant polarity.
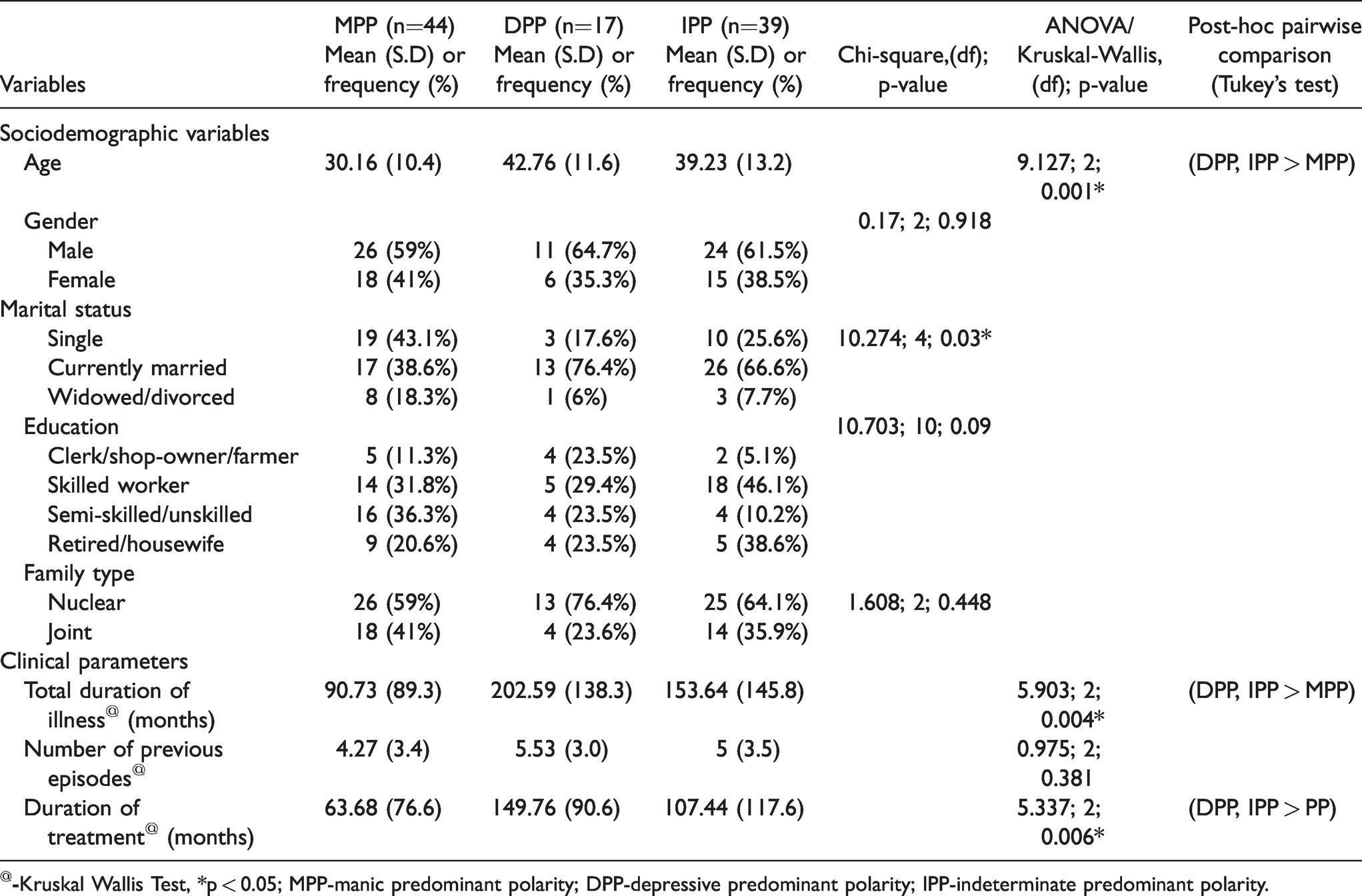
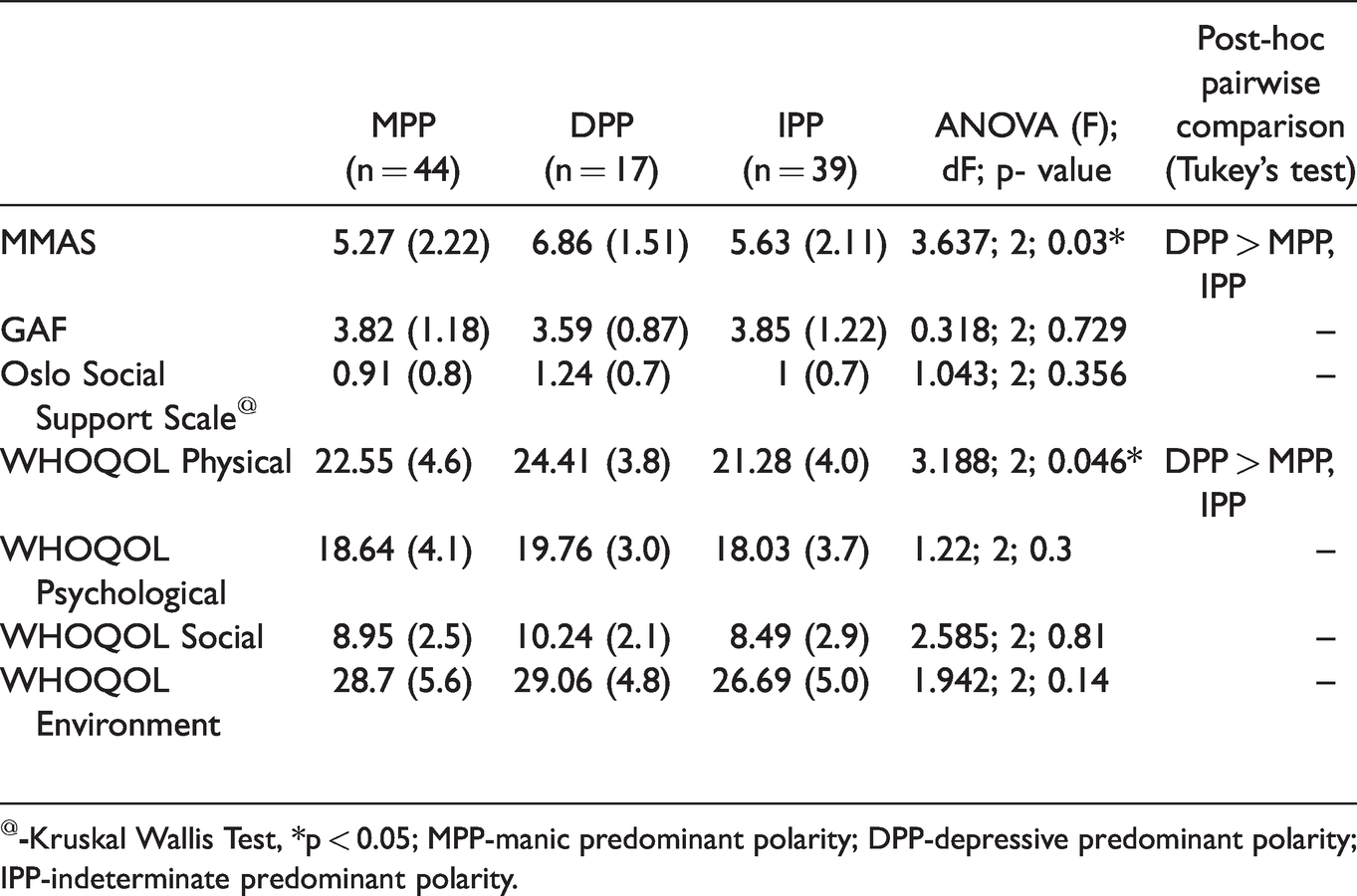
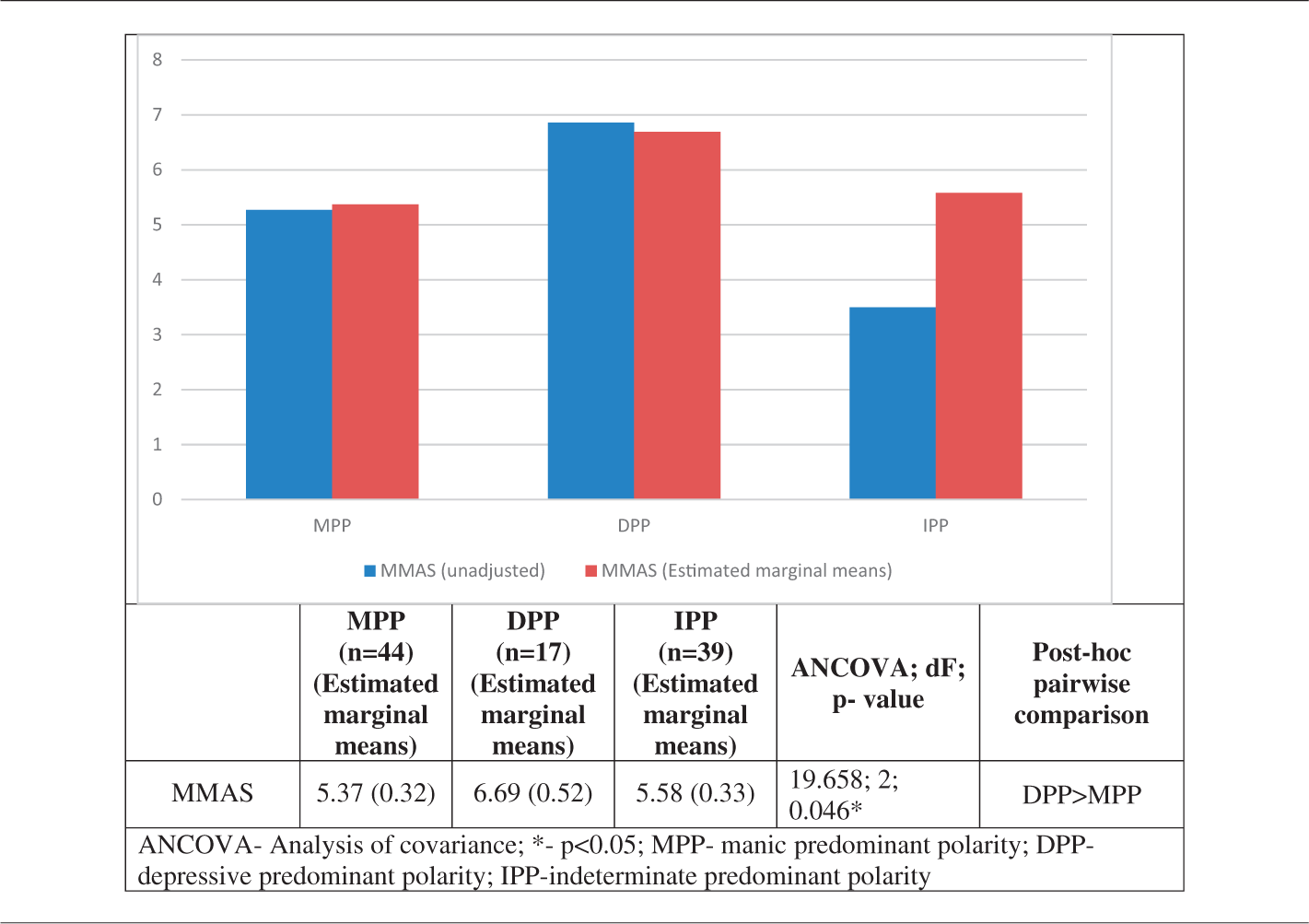
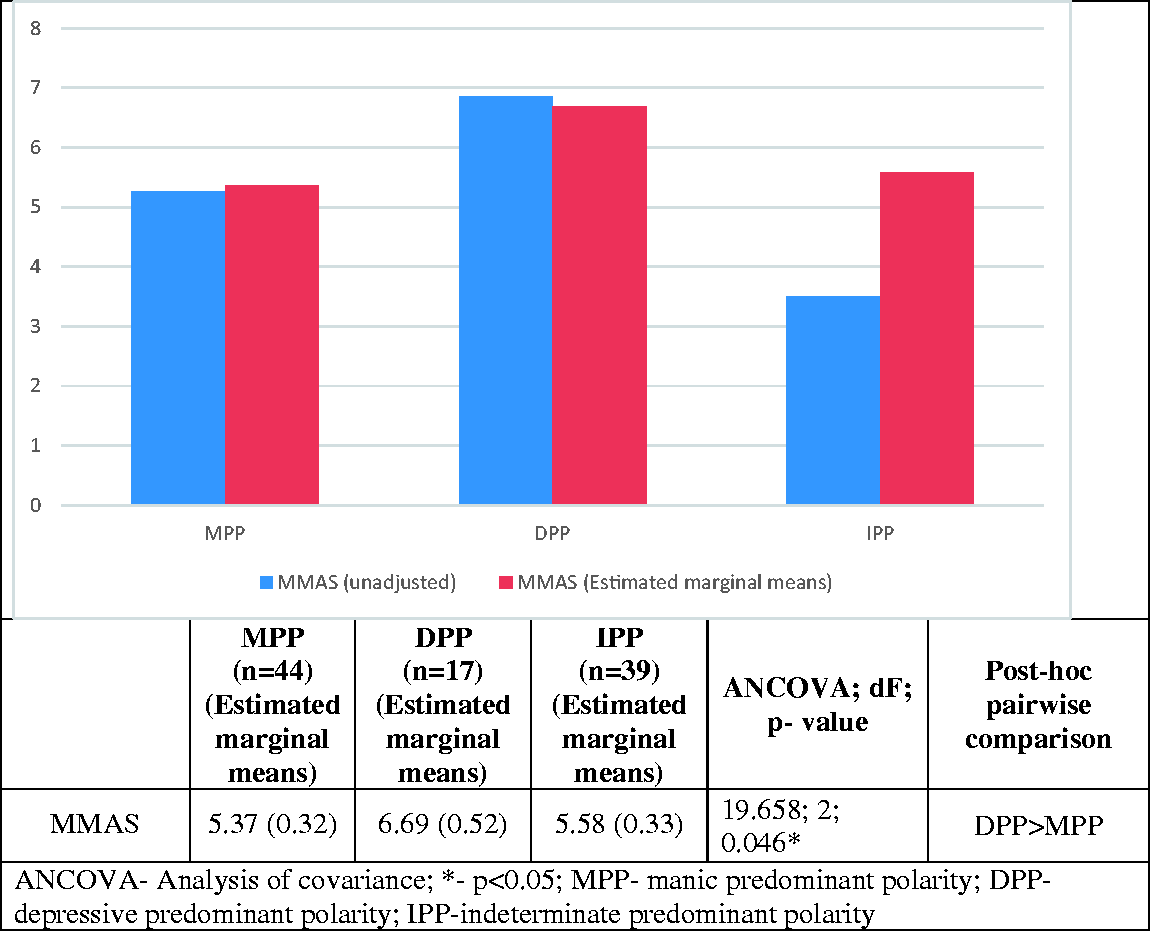
Table 2 which depicts the comparison of the clinical parameters in the three groups, showed that scores on MMAS and WHOQOL-Physical domain were significantly higher for DPP as compared to others. Subsequently, to look for difference in medication adherence in the three groups after adjusting for the effects of the potential confounders; analysis of covariance (ANCOVA) was conducted using age, duration of treatment and WHOQOL-Physical as covariates. Only one amongst total duration of treatment and total duration of illness was chosen as a covariate to avoid collinearity because both the parameters were significantly correlated (Pearson co-efficient = 0.875; p = 0.001). Table 3, which depicts the results of the ANCOVA, shows that there was significant difference in the estimated marginal means of MMAS scores between patients with DPP and MPP (but not with IPP).
Comparison of measures on clinical parameters in patients of BPAD with manic, depressive & indeterminate predominant polarity.
Analysis of covariance of scores on the Morisky Medication Adherence Scale in patients of BPAD with manic, depressive & indeterminate predominant polarity (using age, duration of treatment and WHOQOL-Physical as covariates).
Discussion
Our study found that patients who presented with DPP showed significantly higher medication adherence as compared to MPP and IPP. This difference of medication adherence persisted between DPP and MPP patients when the effects of age, duration of treatment and WHOQOL-Physical were adjusted. Though there is no literature to directly compare our results, it can be said, that our result is supported by another study which showed that the medication adherence is poorer in patients with bipolar I. 9 This is because conceptually, there is a high chance that patients with MPP had a higher prevalence of bipolar I disorder. In our sample of 100 patients, the proportion of MPP was higher than DPP and IPP, which was in line with various studies conducted on PP from Indian sub-continent. 13 This finding becomes even more important considering that medication non-adherence was found to be higher in patients of MPP.
It has been found in the previous research that patients with poor medication adherence tended to have prominent cognitive impairments. The most common cognitive impairments associated with medication non-adherence were impairments in verbal memory and executive dysfunction. This is further supported by the results of the study by Belizario et al. 12 which showed that patients with MPP tended to present with more significant cognitive deficits as compared to other PP and healthy controls. In this context, it becomes imperative to discuss the psychological model of medication adherence which has been named as ‘Health Belief Model’. 21 According to this theory the two major deciding factors for medication adherence are a) patient being able to comprehend his own condition and b) ability to perceive the benefits of being compliant on medication. It is postulated that both these factors are affected by the cognitive deficits and the effects are even more magnified in patients with MPP. In addition, the ever-growing volume of research on cognitive impairment in BPAD, has been able to identify that the impairment of neurocognitive profile in BPAD is very similar to what is seen in other severe mental illnesses like schizophrenia. Authors have commented that the differences in neurocognitive impairments amongst these disorders are rather quantitative than qualitative. 22 By the use of cluster analysis approach in patients of BPAD, authors have been able to identify distinct groups in BPAD, some with normal profile, others with modest impairment and some with more profound impairments. 23 We believe that our study adds a new dimension to this research question, and further research regarding the neurocognitive profiling of patients of various PP can provide us with more answers.
Another important factor that plays a role in medication adherence is the treatment-emergent side-effects. The common side-effects reported to be troublesome by the patients include extrapyramidal symptoms or neuroleptic-induced dysphoria. 24 It has been proven that drugs that are commonly used to treat mania (first generation antipsychotics- including long-acting depot preparations) are more likely to cause these side-effects as compared to drugs used to treat depressive episodes (drugs like Quetiapine, Lurasidone or anti-depressants). 25 As a result, medication non-adherence could be higher in MPP (because of the higher proportion of manic episodes). However, with the advent of newer antipsychotic drugs like Cariprazine for the treatment of bipolar depression, the gap arising due to adverse effect profile between the two groups are now being narrowed down. Another important predictor of non-adherence to medication was found to be history of substance use in patients. 26 Various substance use disorders like alcohol use disorder and cannabis use disorders have been found to be poorly correlated to medication adherence. In the same vein, substance use disorders were also found to be higher in patients with MPP.27,28
Finally, the relationship of the patient with the healthcare provider and social support is one of the most important predictor of medication adherence. 29 Current evidence shows that patients with MPP tended to have a poor social support, 30 which may play an adverse role in the management. In addition to that, higher internalized stigma can also play a deterrent role in medication adherence. 8 Current evidence also shows that patients with MPP tended to report higher internalized stigma as compared to other PP. 13
The strength of our study included use of validated tools and a stringent selection criteria. The major limitations of the study included non-probability method of sampling and use of cross-sectional design. In addition, since medication adherence was measured using a questionnaire, possibility of recall bias remains. Also, since the study was conducted in hospital settings, generalizability of the results to other sectors may be limited. Further studies in this field should be conducted using a larger sample size, prospective designs and more stringent methods of assessing medication adherence. 39% of our sample belonged to the IPP, which is considered to be an exclusive sub-group in the construct of PP. But, it should be remembered that, a longer follow-up for such patients could reclassify them to other PP, and therefore the results may vary. Also, it is imperative to replicate similar studies in other centers, more so in the light of the fact that the prevalence of different PP could vary across different countries. 27
To conclude, our study intended to find the difference of medication adherence in euthymic patients of BPAD across its various PP. It was found that patients who presented with DPP showed significantly higher medication adherence as compared to MPP, even after adjusting for possible confounding factors.
Study highlights
What is the current knowledge?
Medication adherence in bipolar disorder, which one of the prime reasons of sub-optimal therapeutic response, has a scope for improvement.
What is new here?
Medication adherence is worse in patients with manic predominant polarity as compared to patients with depressive predominant polarity.
Footnotes
Author Contribution
Conceived and designed the experiments: SG, NM, RA, GD, DKM & AP. Collection of data: SG, NM, RA Analyzed the data: AP. Wrote the first draft of the manuscript: AP. Contributed to the writing of the manuscript: SG, NM, RA, GD, DKM & AP. Agree with manuscript results and conclusions: SG, NM, RA, GD, DKM & AP. Jointly developed the structure and arguments for the paper: SG, NM, RA, GD, DKM & AP. Made critical revisions and approved final version: SG, NM, RA, GD, DKM & AP. All authors reviewed and approved of the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.