
Abstract
Objective
Our goal is to improve the wellness of our Family Medicine residents now and in the future by educating them on more efficient use of our electronic health record (EHR). Resident physician burnout is a significant problem and is correlated with time spent using an EHR after work hours. Family physicians have the highest rate of burnout of all specialties, and the EHR is a significant contributor to this burnout. Studies have shown that increased EHR education can improve job satisfaction.
Method
Over 5 months, we provided weekly brief (15 minute) educational sessions covering 6 topics twice and a one-hour individualized meeting of each resident physician with an EHR trainer. We evaluated our intervention with wellness surveys and objective measures of EHR efficiency both pre and post intervention. We further evaluated efficiency by comparing pre and post-intervention values of the following: average keystrokes, mouseclicks, accelerator use, minutes per encounter and percent closed encounters at month’s end.
Results
Resident questionnaires showed lessons increased knowledge and intention to use EHR accelerators, but this was not statistically significant. Analysis of objective data showed most efficiency metrics worsened, though most not to a degree that was statistically significant. Residents reported subjective increases in efficiency, and paired data from wellness surveys showed an overall decrease in burnout post-intervention vs. baseline.
Conclusions
Much of the data in this pilot study does not reach statistical significance, but is highly suggestive that increased EHR training can improve at least perceived efficiency and thereby resident wellness.
Keywords
Introduction
Burnout is the antithesis of wellness, and Family Physicians have particularly high rates of burnout (approx. 36%). 1 Consequences of burnout are significant and include: increased rates of physician suicide, substance abuse, errors, malpractice, unnecessary tests and unnecessary consultations as well as decreased physician productivity and satisfaction.1–3
The EHR (Electronic Health Record) is a major contributor to burnout.3,4 Gardner et al. found that 70–80% of physicians report HIT (Health Information Technology) related stress secondary to time-consuming data entry, inefficiency, redundancy and overall inadequate documentation time at work necessitating EHR use during “non-work” hours. 1 Increased EHR education could improve efficiency and thereby decrease burnout (i.e., increase wellness). This has been previously demonstrated in other studies. Robinson and Kersey showed that enhanced EHR education resulted in self-reported improvements in quality, accuracy and efficiency with documentation which led to a 4–5 minutes time savings per hour. 5 Dastigir et al., further demonstrated that perceived job satisfaction and efficiency improved when EHR training was peer-led. 6 Our hypothesis was that increased peer-led EHR training could result in increased efficiency, thereby decreasing burnout and improving resident wellness.
Method
Within our Family Medicine residency over November 2019 to February 2020, we implemented two major interventions designed to educate our 26 residents on our outpatient EHR (Athena) and thereby increase efficiency and improve wellness. The first intervention was to have six resident-led EHR educational sessions conducted during regularly scheduled once weekly didactic sessions. The lessons covered six common EHR accelerators (1. Previous Encounters, 2. Saved Findings, 3. Macros, 4. Order Sets, 5. Creating & Using Encounter Plans, 6. Dragon) and took approximately 10–15 minutes each. In order to maximize the number of residents who received this training, each lesson was repeated twice over 12 weeks. Residents also spent an hour individually with an EHR transformation specialist during which time they were able to cover any topics on EHR use they felt were the most useful. The final intervention took place at the end of February 2020 at which time the final EHR knowledge survey data was collected. Final perceived EHR use and wellness survey data was collected in March 2020.
Results
To assess learning outcomes from the accelerator lessons, residents completed brief questionnaires before and after each lesson regarding knowledge as well as use of a given accelerator. The data was stored in REDCap 7 (a secure web application for managing and storing online surveys).
The results of this data (Figure 1) revealed several findings: 1) most of the residents reported knowledge of the common accelerators but despite that, reported using it less frequently. 2) The pre-knowledge surveys from the second round of lessons showed increased reported knowledge and use of accelerators, which may reflect both retention as well as increased use by residents who attended previous training. 3) Following a lesson, more residents reported the intention to use a given accelerator. None of these findings reached statistical significance. 8

Self reported EHR accelerator knowledge and use pre and post lesson. EHR accelerator lesson topics: (1) previous encounters, (2) saved findings, (3) macros, (4) order sets, (5) creating & using encounter plans, (6) dragon. Where shown as “#-1,” this represents the first time the lesson was taught and where shown as “#-2,” this represents the second time the lesson was taught.
Objective measures of efficiency were tracked through the EHR as well. They include such metrics as median number of keystrokes and mouse clicks per encounter as well as accelerator use and number of closed encounters at month’s end. Data was examined for all residents participating in the intervention, regardless of survey response rates. Analysis of the objective data shows that despite increases in use of Macros, Saved Findings and Previous Encounters, most efficiency metrics actually worsened (Figure 2). A review of Figure 2 shows that use of Previous Encounters, Saved Findings and Macros increased after the intervention when compared to baseline while the number of keystrokes, mouse clicks, and minutes per encounter also increased. The increase in macro use is statistically significant but may have been confounded by the start of the COVID pandemic and initiation of telehealth visits for which Macro use became standard. Notably, the number of encounters per month and percentage of closed encounters also increased in this period reflecting an increase in productivity.

Carecheck data, baseline vs. immediately post-intervention.
In order to measure and track wellness throughout this process, brief anonymous surveys were emailed to residents. Prior to the intervention, we obtained baseline wellness surveys using a modified Maslach Burnout Inventory composed of two questions: 1) “I feel burned out from my work.” 2) “I have become more callous toward people since I took this job.” Paired data from a modified Maslach Burnout Inventory (MBI) show an overall decrease in burnout post-intervention vs. baseline (Figures 3 and 4). Looking specifically at responses to the statement “I feel burned out from my work.” at baseline, 50% of residents reported this occurring weekly compared to 33% post-intervention. We see the same trend in responses to the statement “I have become more callous toward people since I took this job.” with 41.7% of residents reporting feeling this on a weekly basis pre-intervention vs. 25% post-intervention.

Burnout/wellness data. Pie charts on the left reflect baseline (pre-intervention) responses collected in October of 2019 while pie charts on the right reflect post-intervention responses collected in March 2020.
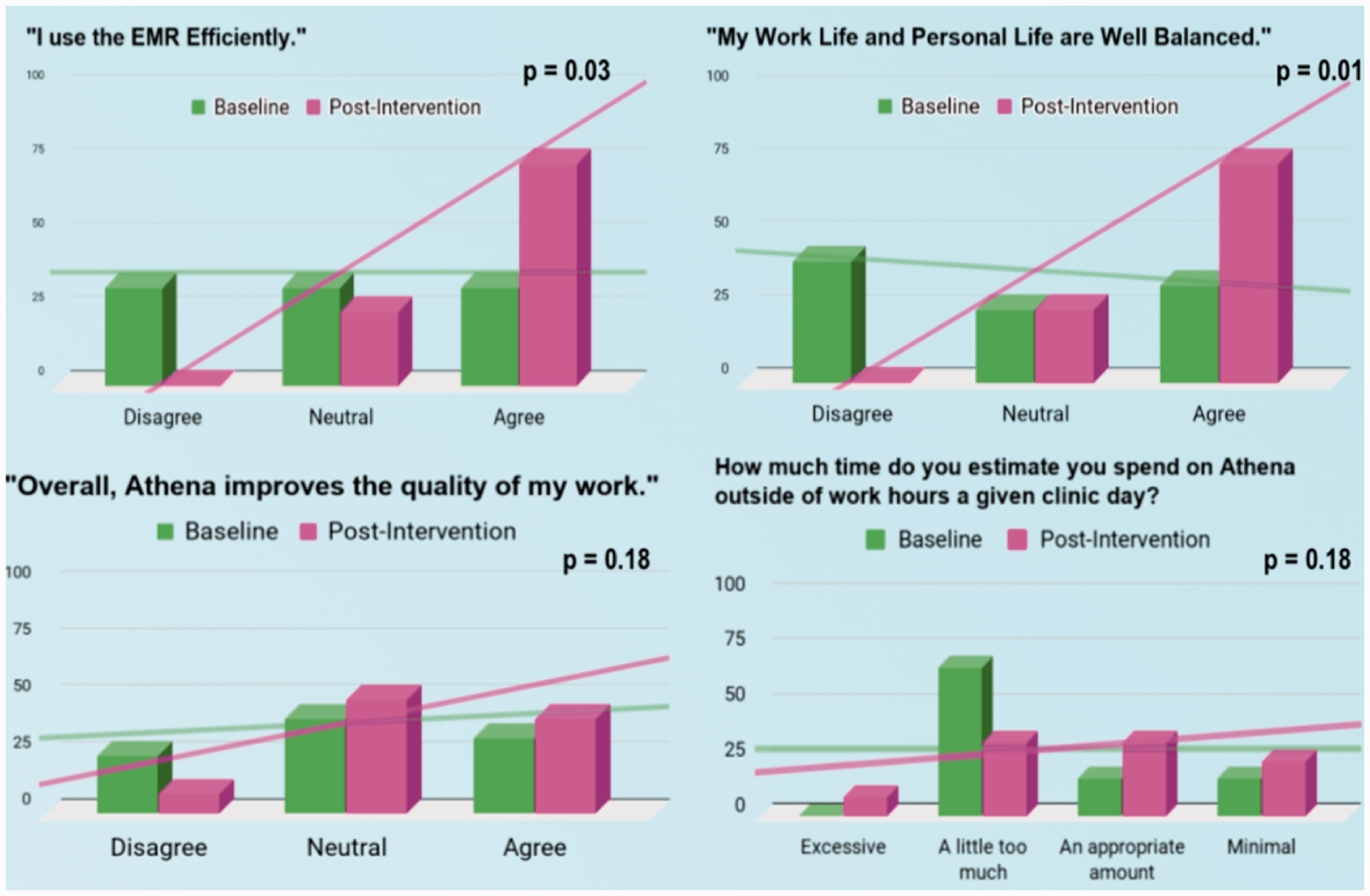
Perceived use and wellness impact. Y-axis values are percent paired respondents unless otherwise indicated.
Discussion
Our study was significantly limited by resident availability and participant numbers due largely to the nature of residency wherein rotations change on a monthly basis (e.g., a resident may be working in the clinic one month and therefore available to attend didactic to participate in our study and the next month is fully occupied by inpatient work and thus unable to attend and participate). Hence, fewer than half of the residents were available at any lesson. Though much of the data in this pilot study does not reach statistical significance, it is highly suggestive that increased EHR training can improve at least perceived efficiency and thereby resident wellness. This data also implies that EHR training may improve efficient use of the EHR even when knowledge is already present. Further, there may even be a placebo effect to the EHR training, as perceived efficiency improved while most objective efficiency metrics worsened.
Future research will need to examine and address which accelerators will best impact EHR knowledge deficit as well as barriers to training and use. The effect of training year was also not accounted for in our study but certainly impacts EHR efficiency and wellness and therefore needs to be studied. Finally, any such study needs to be compared to a control group before any true conclusions can be drawn about the impact of such an intervention.
Conclusions
While much of the data in this pilot study does not reach statistical significance, the observed increases in EHR accelerator knowledge and overall accelerator use following enhanced training, combined with the subsequent improvement in wellness self assessments, is highly suggestive that increased EHR training can improve at least perceived efficiency and thereby resident wellness. Regardless of why wellness metrics improved, the fact that they did in an era when physician burnout is prevalent and costly, suggests at the very least that this topic warrants further investigation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.