
Abstract
Objective
Patients with epilepsy who have been charged with a serious offense may be referred by the courts for forensic psychiatric examination. A detailed psychiatric and neurological examination is often necessary to assist the courts in making the right decision, as exemplified in the current case presentation.
Method
The forensic case of a 30-year-old Tunisian male with temporal epilepsy who exhibited an inadequate response to the treatment is presented here. The patient attempted to kill his neighbor after a cluster of seizures, showing apparent postictal aggression. An antiepileptic treatment was introduced a few days after the person’s detention and was followed by forensic psychiatric examination, but the latter was not done until three months afterwards.
Results
On forensic examination, the patient’s thought processes were clear with no evidence of a thought disorder or psychosis. Both medical and psychiatric opinions stated that the attempted homicide was due to a postictal psychosis. The patient was transferred to a psychiatric facility for further management and was found not guilty by reason of insanity.
Conclusion
This case illustrates the difficulties that experts may encounter in establishing criminal liability after aggressive behavior associated with epilepsy. It highlights shortcomings in Tunisian law (and promptness of forensic psychiatric examination) that should be addressed to ensure fairness of the legal process.
Introduction
Although violence associated with epilepsy is well documented in the medical literature, reports of criminal behavior associated with seizure activity are scarce, which may cause a forensic challenge. Such behavior is notably a complex phenomenon with multifaceted causes. 1
International criteria to determine whether a violent crime was the result of an epileptic seizure. 2
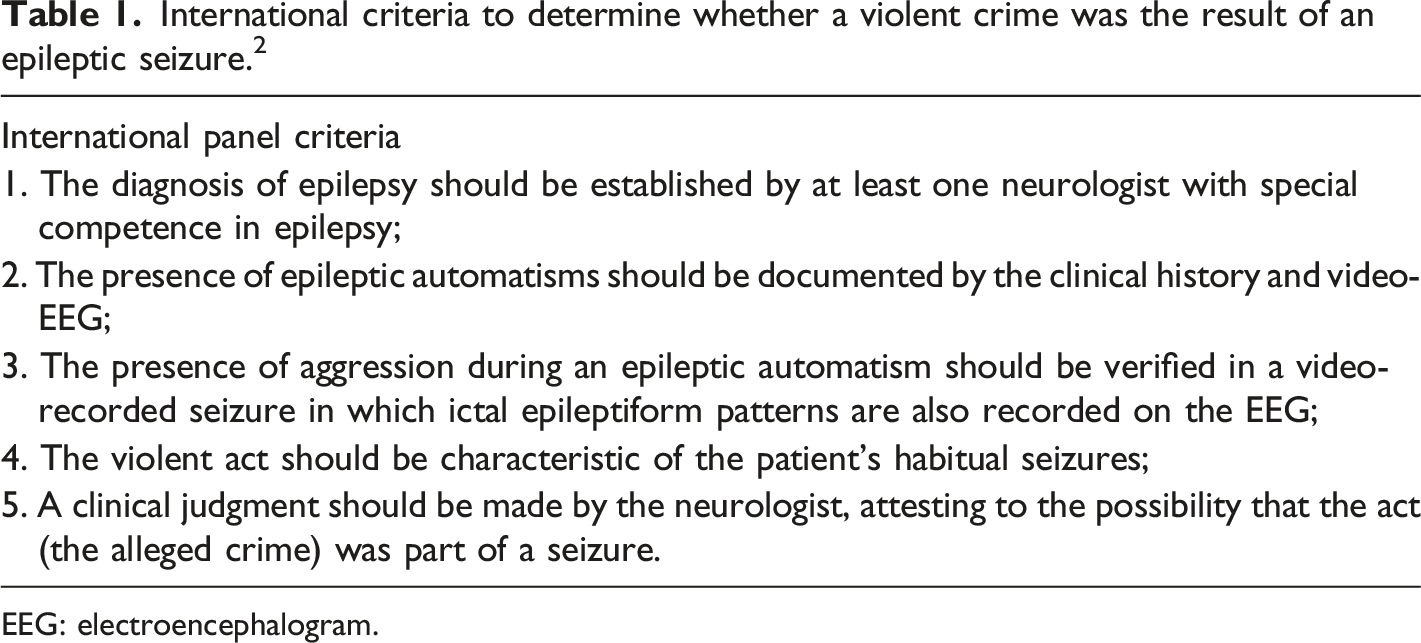
EEG: electroencephalogram.
In the following, we report the case of a patient with epilepsy and aggression resulting in an attempted homicide. We also discuss the legal aspects of epilepsy with reference to medical issues that might emerge within the context of Tunisian law.
Case report
We report the case of a 30-year-old man with a history of seizures that began at the age of 13. Even though his seizures were recurrent, he did not have a neurological follow-up for six years due to financial constraints.
At the age of 19, he began to experience diurnal seizures consisting of a rising epigastric sensation and hallucinatory aura that he described as terrifying, followed by rhythmic movements. Seizure frequency was several times per month. Therefore, he was referred to the neurology unit for diagnostic evaluation. His past medical history was non-contributory. He had no prior psychiatric history, and substance and alcohol use were not significant. The general physical exam was unremarkable, and so was the neurological exam. The findings of the electroencephalogram (EEG) were reported as normal. Neither magnetic resonance imaging (MRI) of the brain nor an EEG video was not performed due to financial constraints.
Based on clinical information, the diagnosis of focal impaired awareness automatism seizure evolving into a bilateral tonic-clonic seizure was made. Despite treatment with Valproic Acid (1000 mg per day), he continued to have weekly epileptic seizures. His medication was changed to a combination of Valproic Acid (1500 mg per day) and Carbamazepine (800 mg per day). He remained seizure-free without side effects while taking this treatment, but since then, his medical follow-up has been irregular due to financial constraints.
Valproic Acid was discontinued due to its unavailability in pharmacies, but the patient did not consult his physician for treatment adjustment. His seizures began to increase in frequency, and he became violent for several days after a cluster of seizures. The patient did not exhibit any sign of psychosis during this time. Moreover, because he previously had never been violent, the family neglected these episodes of violence.
Two months later, the patient had an altercation with his father, whom he accused of not being concerned with his safety; soon after that event, he had a cluster of seizures. A few hours after the resolution of the attack, he started hearing “voices” for the first time. These “voices” asserted that his father did not care about him because their neighbor had bewitched him. The following morning, he walked to the neighbor’s home and stabbed her with a kitchen knife, even though he had no prior conflicts with this neighbor. The neighbor’s daughter witnessed the incident and saved her mother from being strangled to death. Thereupon, the patient was arrested and charged with attempted homicide.
Upon the police interrogation, he kept repeating several times, “she bewitched my father; I have to kill her.” The psychotic symptoms regressed within a few days. While in jail, antiepileptic drugs (AEDs) were introduced again because he continued to have epileptic seizures. The patient had not been taking his AEDs properly months before the incident. He was therefore submitted to a forensic psychiatric examination. It was performed by two experts: a psychiatry professor and a neurology professor. The neuropsychological assessment occurred about three months after the crime. On examination, the patient was calm, and his speech was coherent and logical. He had no signs of delirium, and his thought process was clear, with no evidence of a thought disorder or a psychotic process. He denied having said that the neighbor had bewitched his father. He claimed that he never believed in the idea of bewitchment. He remembered stabbing the victim, but he could not explain how the incident happened. He felt guilt over this violent behavior. Furthermore, there was no evidence of drug use prior to the incident, and more importantly, there was a clear occurrence of a seizure before the attempted homicide.
Both medical and psychiatric opinions stated that the offender met the criteria for a DSM-5 diagnosis of psychosis due to the organic mental disorder. The attempted homicide was due to a post-ictal psychosis (PIP), and the forensic psychiatric examination concluded that the offender was mentally disturbed when the crime was perpetrated. Therefore, he was discharged and sent to a psychiatric facility for further management. The court’s system ordered involuntary commitment for a period of three months. During the hospitalization, the patient received a combination of Valproic Acid (1500 mg per day) and Carbamazepine (800 mg per day). The dosages were adjusted based on valproic acid and carbamazepine blood levels. Since there were no signs of psychosis, no antipsychotic was used. Once the period of mandatory hospitalization was completed, article 30 of Act No. 92-83 of 3 August 1992 on mental health and conditions of hospitalization for mental disorders was applied to ensure regular follow-up.
Unfortunately, the patient did not attend the medical control regularly. However, he showed good adherence to the combination of AEDs prescribed during the psychiatric hospitalization, resulting in a noticeably lower seizure frequency and the disappearance of behavioral disorders.
Discussion
This report describes the case of a young man with a clinical diagnosis of focal impaired awareness automatism seizure evolving into a bilateral tonic-clonic seizure. He developed increasingly violent behavior culminating in an attempted homicide due to irregular follow-up and poor compliance with AEDs. The evidence from history and medical records supports the idea that this attempted homicide was due to a PIP. These findings are in consonance with previously reported demographic and clinical characteristics of an epileptic population who commits violent crimes. Many of these patients are male, aged between 20 and 50 years, typically with seizure onset starting in childhood or adolescence.3,4
Patients with epilepsy may be involved in criminal activities. This case is challenging for forensic psychiatrists and neurologists who may be required to assist in defining the level of criminal responsibility. The forensic assessment of violent behavior in this population requires careful consideration of several factors: whether the act is directly related to the epileptic seizure, a feature of post or preictal mental state changes, a complication of other pathologies that increase the risk of aggressive behavior, or unrelated to epilepsy. 5
Logsdail and Toone’s Diagnostic Criteria for Postictal Psychosis. 6
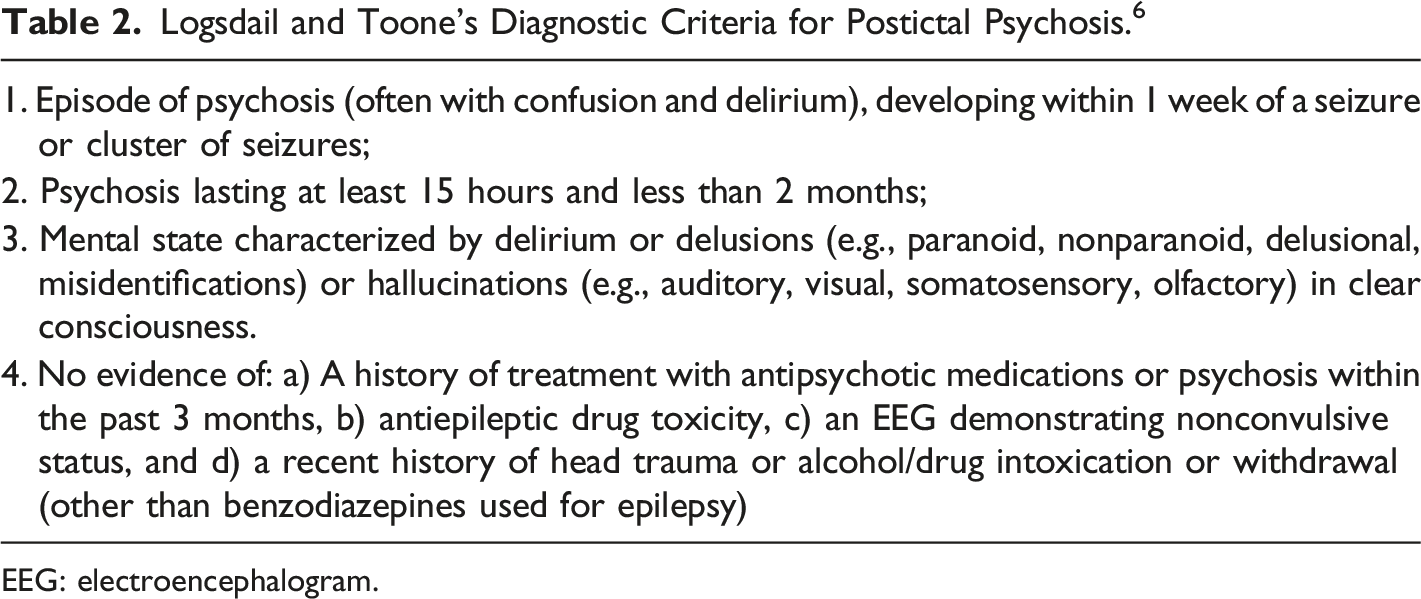
EEG: electroencephalogram.
The interval between the onset of epilepsy and the episode of PIP was 17 years. The literature indicates that it ranges from 7 to 44 years. 7 This interval is long enough to provide additional evidence of the kindling mechanism in the pathogenesis of psychosis in chronic epileptics through long-term epileptic discharges. While the detailed pathophysiology of psychosis in epilepsy is unknown, dopaminergic activity and frontal-subcortical circuits (resembling the present model of psychosis) are believed to be involved. 7 PIP has been attributed to neurochemical and ultrastructural dysfunctions in a much wider set of limbic circuits, including the ones directly affected by temporal lobe epilepsy.8,9 These mechanisms may increase the propensity to develop psychotic symptoms by altering the perception of reality. In fact, the patient interpreted the altercation with his father as a sign that he was not caring adequately for him. Such behavior was then explained as bewitchment by the neighbor. Interestingly, the secondary generalization of the seizure disturbs the frontal cortex leading to the modulation of emotional reaction. This disruption facilitates violent acts.
The patient denied having said that the neighbor bewitched his father. Another finding that may be relevant to our patient is that hallucinations, delusion, and confusion are particularly common when the etiology of the psychosis is related to an underlying neurological disorder, particularly epilepsy. 10
We argued that the issue of non-compliance to treatment should be addressed. There may have been a contributing role in the discontinuation of AEDs in this post-ictal aggression. The discontinuation of Valproic Acid, which has a mood-stabilizer property, can be related to the development of psychosis through different mechanisms: the increase in the frequency, severity of clusters, and the propensity for post-ictal mood dysregulation.
On forensic psychiatric examination, the patient was receiving his AEDs. There was no evidence of hallucinations or delusions, and cognition was intact. Theoretically, PIP is preventable if seizures are well-controlled. 11 It is worth mentioning that in some cases, AEDs on their own are insufficient to treat PIP. Thus, the combination of antipsychotics with AEDs becomes imperative, but the lack of treatment recommendations makes their use problematic. Practitioners should be vigilant with the prescription of antipsychotics due to the risk of pharmacokinetic interactions with AEDs, resulting in a reduced epileptogenic threshold.12,13 The literature indicates that the pro-convulsive effect of Risperidone, Aripiprazole, and Ziprazidone seems to be at a tolerable level, at least if these drugs are prescribed within a therapeutic range. 14
Preventive measures are also necessary for managing this kind of psychosis. As PIP is triggered by repetitive seizures, the importance of good treatment compliance must be emphasized. Owing to the lowering of the seizure threshold, recent literature highlights that the long-term use of antipsychotics is largely discredited and recommends the prompt administration of benzodiazepines for the preventive treatment of PIP. 15 Indeed, preventing PIP requires eliminating seizures. Benzodiazepines are effective at controlling and preventing seizures.
Regarding prognosis, recurrence is the main long-term risk of PIP, especially when coupled with poor adherence to AEDs. Progression to severe mood disorders or to poor prognosis interictal psychosis is possible. Around 10% of patients with PIP may become chronically psychotic. 7 Thus, early diagnosis and effective management of PIP may inhibit or prevent the development of interictal psychosis. 7
Under the Tunisian legal system, regardless of the gravity of the crime perpetrated, the forensic psychiatric examination is not ordered systematically. 16 Generally, it is performed in case the accused has a history of psychiatric follow-up or upon evidence that the offense committed was of psychiatric origin. Article 38 of the Tunisian Criminal Code states that “an offense is not punishable if the accused has not reached the age of 13 years or has a mental disorder at the time of the incident”. The lack of criminal responsibility for reasons of mental disorders is recognized, with some precisions, in many European countries (France, Germany, Italy, Austria, Spain, Denmark, Netherlands, and Britain) and Canada. For instance, in Sweden, the pervasiveness of mental disorders does not exclude criminal liability, but it is an attenuating circumstance.17,18 In the United States, federal laws can authorize mandatory commitment to a psychiatric institution when a person suffering from a serious mental illness is accused of a crime or adjudicated under the federal criminal justice system or found not guilty by reason of insanity. 19
The French criminal code provides two grades of lack of responsibility: absence or attenuation of liability. In contrast, Tunisia’s legal system operates on an ‘all-or-nothing' basis: responsible or not responsible. 17 In this case, PIP has been used as a justification for insanity. The patient exhibited a post-ictal aggressive behavior after an epileptic attack. He had a clear history of post-ictal delusions, hallucinations, and discontinuation of his AEDs, which led to an increase in the frequency and severity of seizure clusters. Although he manifested aggressive behavior, he could not explain why he did not control it at that time.
AEDs were reintroduced a few days after the detention and the accused was referred to forensic psychiatric examination after three months, which makes the retrospective assessment of the mental state at the time of the aggression very challenging. Therefore, the task of experts to establish the criminal liability of the accused was difficult. The French National Authority for Health 20 recommends early psychiatric assessment if there is any doubt about the defendant’s mental state. Subsequently, the evaluation findings are helpful to psychiatric examiners. In Tunisia, the long waiting list for observations and the lengthy legal procedures are contributing factors to delays in referrals. This raises ethical issues surrounding the delays in the psychiatric observation, as the accused may not benefit from a fair observation. It is recommended that forensic psychiatric observations be conducted as soon as possible after the offense to avoid compromising the fairness of the assessment. It should be stipulated in the Tunisian legislative text to facilitate the experts’ task.
Although the psychiatric experts stressed the importance of good adherence to AEDs to avoid relapses, the condition of involuntary treatment in the community was not respected in the presented case. It seems that the exact nature and requirements of the community treatment order were not well understood. Thus, a better understanding of legal dispositions of involuntary treatment is required. We propose that following a request for the measure of mandatory hospitalization to be lifted, the experts of the commission should recommend the application of article 30 of the mental health law, with a minimum length that has to be specified. It consists of an involuntary outpatient commitment ordered by the court that forces the patient to adhere to an outpatient treatment plan designed to prevent relapse. Forensic experts shall outline the area of expertise to address a doctor who should take over once the patient is released. In order to improve compliance to care, the Ministry of Justice shall designate an adult family member or a social worker from the patient's area of residence to care for the patient outside the hospital, if necessary, upon his release. The decision to maintain or to discontinue the procedure of involuntary outpatient commitment should be determined after the evaluation of the patient’s dangerousness.
Conclusion
PIP is a serious psychiatric complication of chronic epilepsy that may lead to criminal liability. This case highlights the importance of early PIP diagnosis to provide adequate treatment and avoid or reduce a significant risk of violence against self and others. It also emphasizes the particular need for collaboration between neurologists and psychiatrists in the assessment and management of such neuropsychiatric manifestations. With regard to the legal situation, some shortcomings in the Tunisian legislation related to the processing delay of psychiatric observation and the condition of involuntary treatment in the community ought to be observed. It is, however, important to address these crucial issues in the legal framework in order to have a more objective and accurate assessment of criminal liability.
Footnotes
Authors’ contribution
Maalej M: performed the forensic psychiatric examination and revised the manuscrit
Omri S, Charfi N, Smaoui N : drafted the manuscrit
Zouari L, Ben Thabet J, Gassara I, Feki R : critically reviewed
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All authors read and approved the final version of the manuscript.