
Abstract
The study sought to examine (1) the relationship between MD and MI; (2) the relationship between MD/MI and pandemic-related burnout and resilience; and (3) the degree to which HCPs experienced pandemic-related MD and MI based on background characteristics.
Introduction
COVID-19 has led to unprecedented stressors for global healthcare systems and personnel due to factors such as surges in patient volume, scarcity of personal protective equipment, prolonged hospital stays, and supply chain shortages.1,2 These challenges occurred during already stressful circumstances in healthcare that contributed to rising rates of burnout among clinicians. 3 Due to the additional exposure to stressors during the pandemic, COVID-19 has increased opportunities for moral distress (MD) and moral injury (MI) among healthcare professionals (HCPs). In this study, these 2 essential concepts, MD/MI were investigated in the context of the COVID-19 pandemic.
The concept of MD was first used to describe the institutional and external constraints hindering the moral autonomy of nurses. 4 Current definitions characterize MD as a serious compromise of an individual’s moral integrity, either because one feels unable to act in accordance with one’s core values and obligations or because attempted actions fail to achieve the desired outcome.5,6 While nurses have been the leading focal point for most of this research, MD in physicians, respiratory therapists, and pharmacists has also been assessed, demonstrating the breadth of MD in healthcare. 8 Prior research indicates that MD is associated with burnout and intent to leave a position.7,8
MI occurs when one’s moral or ethical beliefs have been violated repeatedly over time, leading to increased psychological, spiritual, behavioral, biological, or social distress.9,10 MI can also result from participating in an action or not stopping an action that leads to one reexamining their moral beliefs. 2 Risk factors for MI include: the MI event occurring at the same time as another stressful event, the death of a patient from a vulnerable population, lack of social support, staff feeling unprepared for the emotional or psychological consequences of burnout or traumatic stress, and team members who do not take responsibility for the MI event or are not supportive of their coworkers. 2
Although the concepts of MD/MI share some similarities, the relationship between MD/MI is unclear in the literature. Sources of MD/MI may be similar, if not identical, and both terms have been erroneously used interchangeably. Epstein and colleagues et al (2017) theorized that repeated episodes of MD result in MI. 11 In this theory, MI is a sense of residue that is long-lasting and powerfully integrated into thoughts and views of oneself and can be damaging to the self and one’s career, particularly when morally distressing episodes repeat over time. 11 Litz and Kerig (2019) describe MD/MI as occurring on a continuum, with MD appearing on the less severe end of the continuum. 12
This mixed-methods study aimed to explore the relationship between MD/MI among trauma and ambulatory HCPs in the context of the COVID-19 pandemic at 2 academic institutions in southeastern United States. It was Institutional Review Board exempted by both institutions. This research aimed to determine the relationship between MD/MI, the relationship between MD/MI and pandemic-related burnout and resilience, and whether HCPs experienced pandemic-related MD/MI differently based on their background.
Methods
Measuring MD/MI
A convergent mixed-methods approach was used to study MD/MI among HCPs. The research team collected and analyzed both quantitative and qualitative survey data and triangulated the findings.13,14 The survey was administered to HCPs at 2 institutions. It included 4 sections: demographic information, the Measure of MD for Healthcare Professionals (MMD-HP), 8 the MI Symptom Scale-Healthcare Professionals (MISS-HP), 15 and a section containing additional items. These items were as follows: a single item measure of burnout;16,17 2 questions on respondents' “intention to leave” their current position due to MD; a quantitative question pertaining to resilience and the impact of the COVID-19 pandemic; and 2 open-ended questions explicitly related to MD/MI during the COVID-19 pandemic.
The MMD-HP is a 27-item scale that measures both the frequency and intensity of MD and can be used in all healthcare settings; previous studies have indicated high internal consistency (α>.9) for the MMD-HP.8,18 Individual scores on this scale range from 0 to 432. The MISS-HP is 10-item scale measuring MI symptoms in HCPs; acceptable internal consistency (α>.7) has been reported for the MISS-HP. 15 Individual scores on this scale range from 0 to 100.
Survey Administration
Study data were collected and managed using REDCap electronic data capture tools.19,20 A survey link was emailed to HCPs with a reminder at week 2 and remained open for 4 weeks in March 2022, just after the height of the COVID-19 Omicron variant peak. Surveys were sent to approximately 706 people and were completed by 184 participants comprised of both inpatient and outpatient physicians, nurses, residents, respiratory therapists, and advanced practice providers (APP) for a response rate of 26%.
Quantitative Analysis
For demographic information, categorical data are presented as numbers and percentages; continuous variables are presented as means, standard deviations, and ranges. Cronbach’s alphas were computed as measures of internal consistency to estimate the lower-bound reliabilities of the MMD-HP and MISS-HP. A linear regression analysis was conducted to determine the relationship between demographic characteristics and MD (MMD-HP), MI (MISS-HP), burnout, resilience, and intent to leave. All statistical analyses were conducted in Stata version 15 and SAS Enterprise Guide 8.3; a P-value of .05 was considered significant throughout.
Qualitative Analysis
Open-ended responses to 2 questions were collected for analysis. Individual responses were assigned a unique ID, and personal identifiers were removed. Coding and analysis were done according to the principles of the Creswell approach, specifically narrative thematic analysis.13,21,22 Individual research members performed a line-by-line analysis of the responses to identify important phrases. Members then reviewed identified phrases together to assess for agreement. Individual research members then created codes for each of the identified phrases. After consensus was reached, a consolidated list of codes was created. Overlapping concepts and themes in the code were then organized into categories and subcategories. Research members then mapped all quotes into their designated categories to ensure accuracy. The professions of respondents were then added back to each quote. At each stage, research members first analyzed the data alone and then as a team to increase the internal validity and reliability of the data analysis. The codes and categories were brought to a review content expert panel to assess the quality of the data analysis at each stage. Primary and secondary analysis alignment was greater than 95% within all reviews.
Results
Participant Characteristics
Participant characteristics (N = 184).
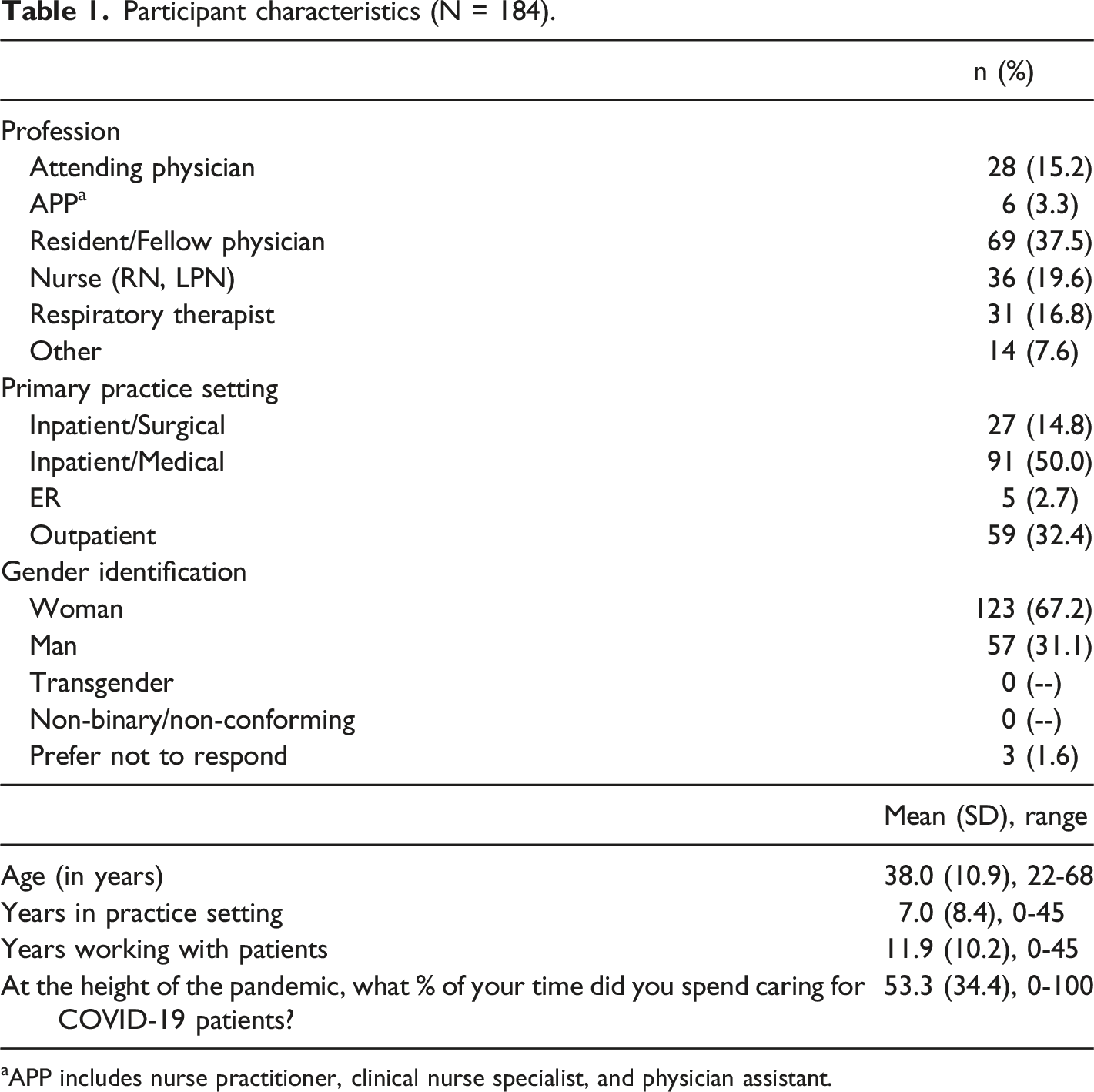
aAPP includes nurse practitioner, clinical nurse specialist, and physician assistant.
Burnout, Intent to Leave, and Resilience
Burnout, intent to leave, and resilience.
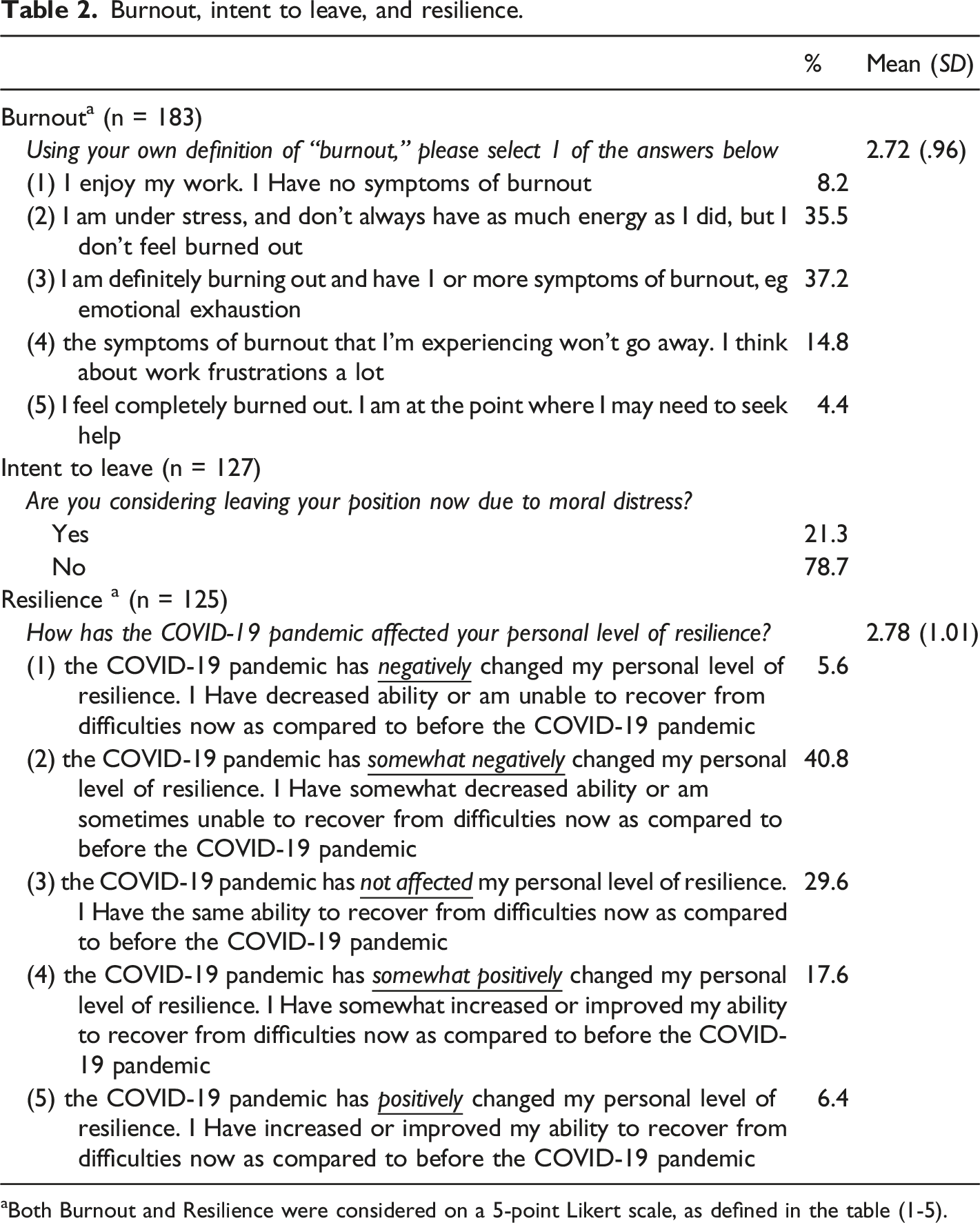
aBoth Burnout and Resilience were considered on a 5-point Likert scale, as defined in the table (1-5).
MD/MI Scales
MD (MMD-HP) and MI (MISS-HP) scores by participant characteristics.
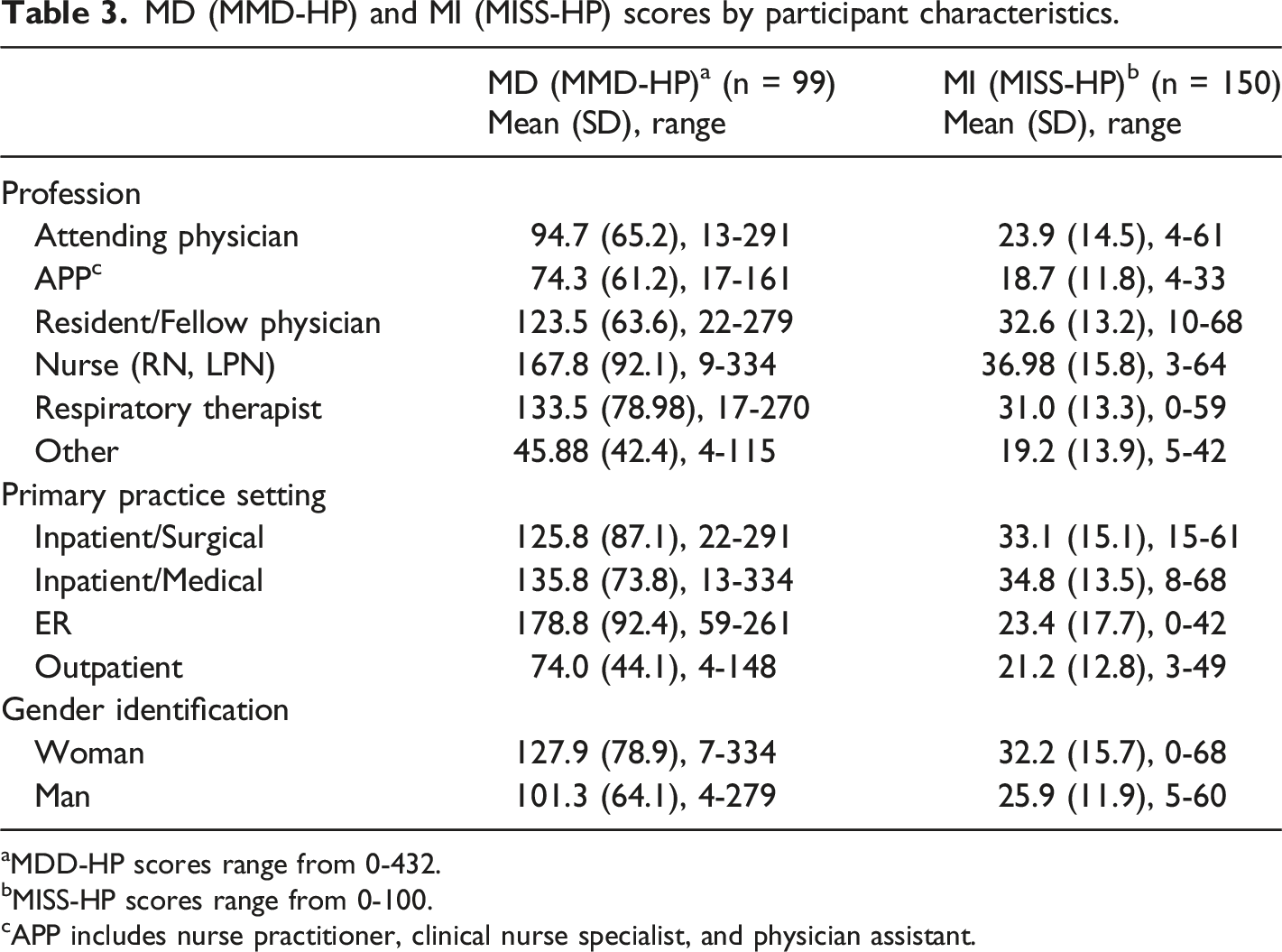
aMDD-HP scores range from 0-432.
bMISS-HP scores range from 0-100.
cAPP includes nurse practitioner, clinical nurse specialist, and physician assistant.
Relationship between MD/MI and Burnout, Resilience, and Intent to Leave
Correlation matrix for MD, MI, burnout, resilience, and intent to leave (n = 96).
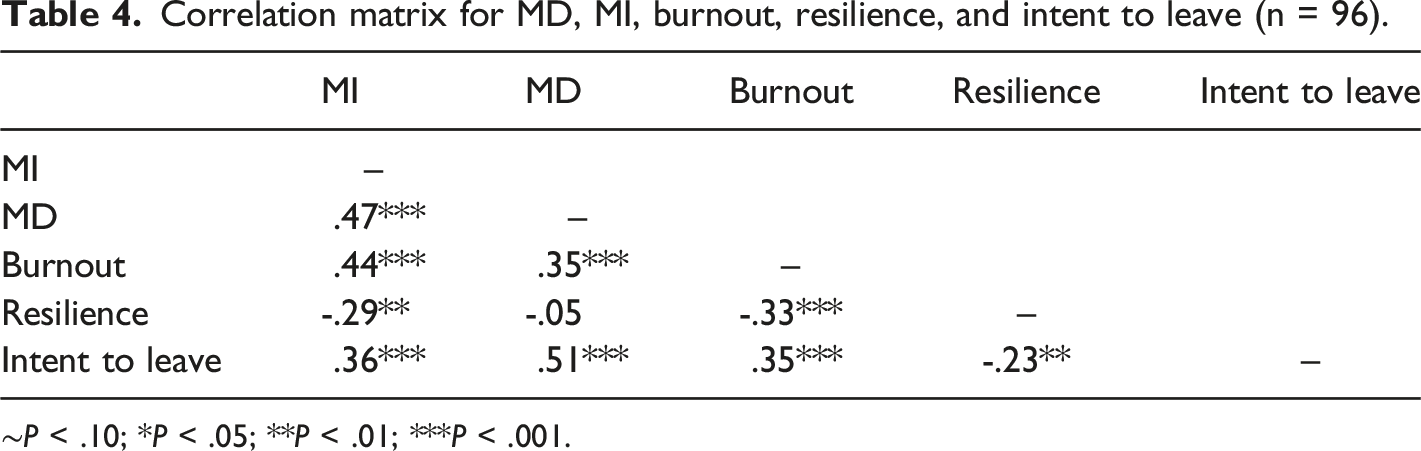
∼P < .10; *P < .05; **P < .01; ***P < .001.
Regression results for moral distress and moral injury.
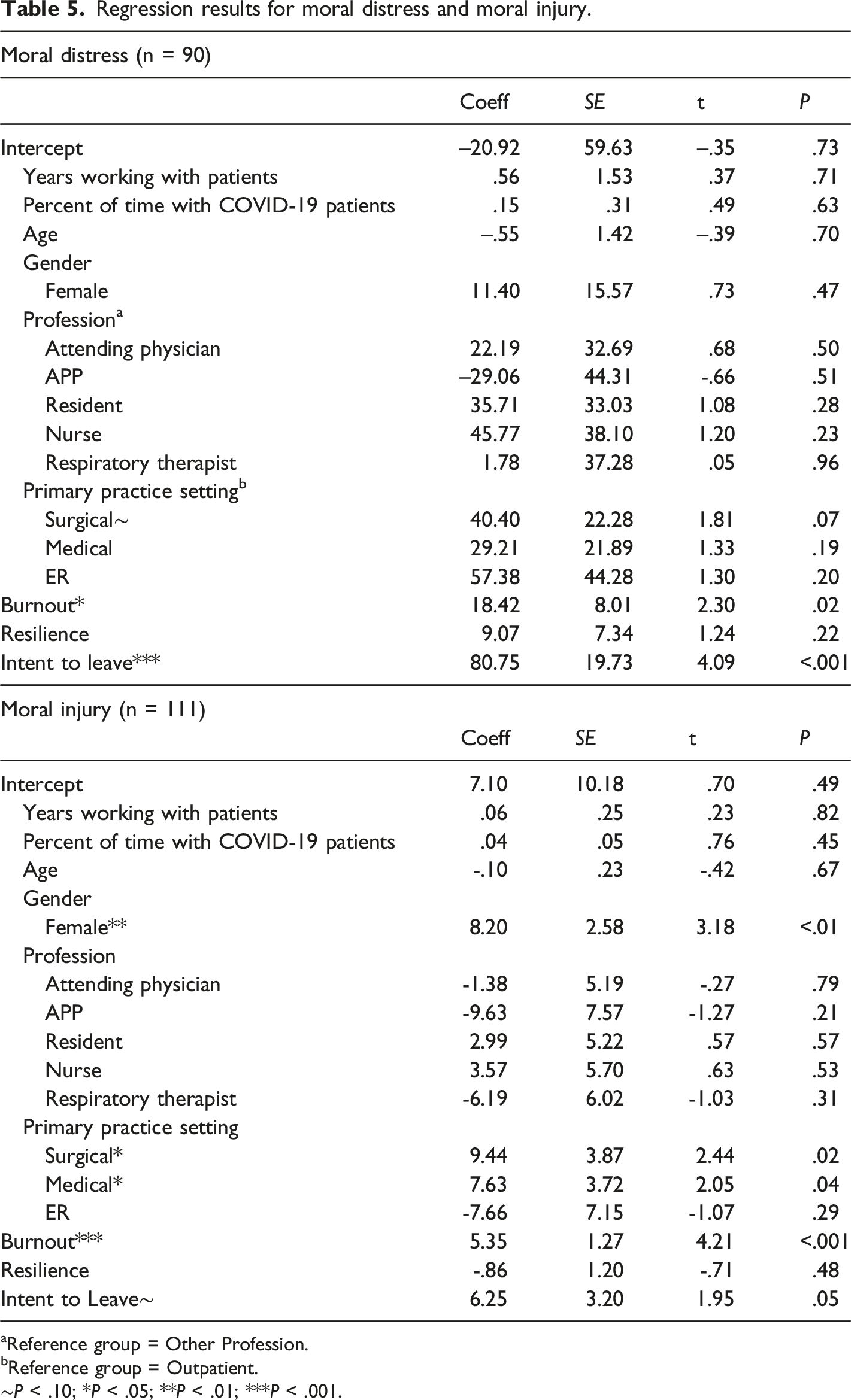
aReference group = Other Profession.
bReference group = Outpatient.
∼P < .10; *P < .05; **P < .01; ***P < .001.
Qualitative Results
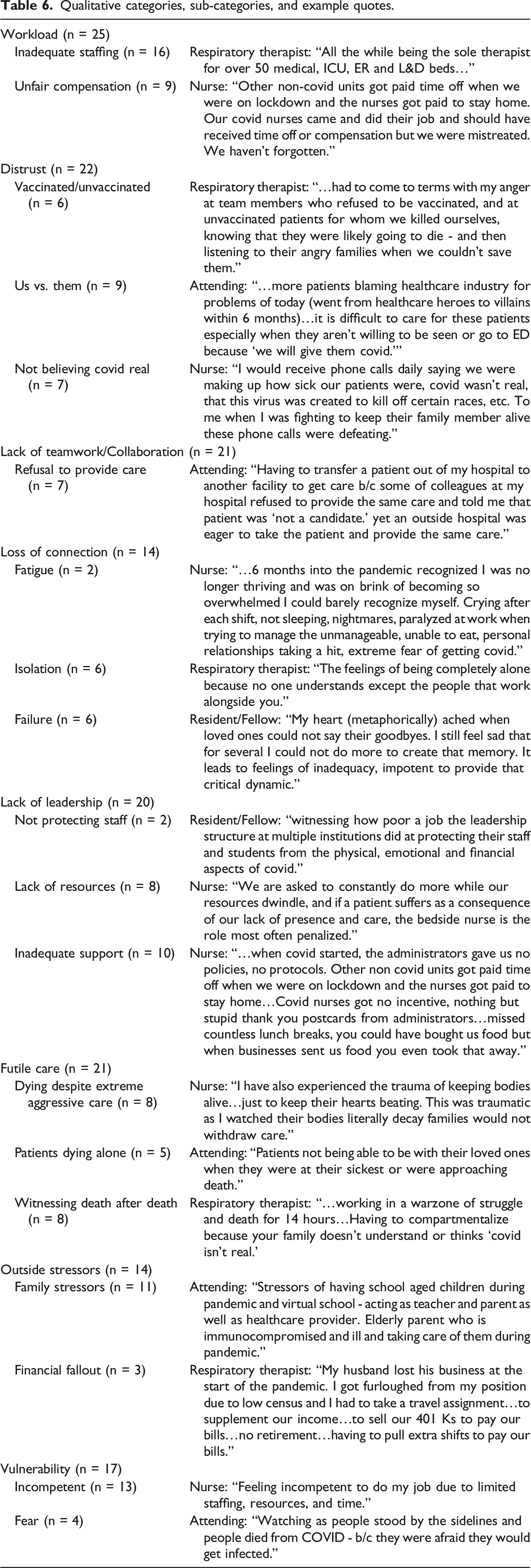
Analyzing 2 open-ended questions related to sources of MD/MI during the pandemic, 8 categories and 19 subcategories were identified in the data. Among the categories, workload (n = 25) was the most referenced by respondents as a source of MD/MI. Examples supporting this category are: …Less personnel support to get the work done… (Attending Physician)
Being under paid for our professional care and being shown time and time again our institute doesn't care about us. (Respiratory Therapist)
…Our covid nurses came and did their job and should have received time off or compensation but we were mistreated… (Nurse)
A prevalent subcategory identified was a lack of resources, as referenced by 8 respondents. A response from a nurse demonstrates this: We are asked to constantly do more while our resources dwindle, and if a patient suffers as a consequence of our lack of presence and care, the bedside nurse is the role most often penalized. (Nurse)
Fourteen respondents identified personal and family stressors as sources of MD/MI as evidenced by the following quote: Stressors of having school aged children during pandemic and virtual school - acting as teacher and parent as well as HCP… (Attending Physician)
Other categories and subcategories such as isolation (n = 16), distrust (n = 22), loss of connection (n = 14), and futile care (n = 21), were major and recurrent themes in survey results. The following responses represent these categories: …working in a warzone of struggle and death… (Respiratory Therapist) Dealing with very sick patients on a consistent basis and witnessing death… (Nurse) …Watching as people stood by the sidelines and people died from COVID - b/c they were afraid they would get infected… (Resident/Fellow) ...continue to torture patients even though our actions are futile… (Attending Physician)
Qualitative categories, sub-categories, and example quotes.
Discussion
The primary finding is the establishment of a significant association between MD and MI among HCPs serving during the COVID-19 pandemic. Deeper understanding of the quantitative relationship between MD/MI is seen through participant comments. Overwhelming workloads and patient volumes along with perceived poor compensation contributed to MD/MI among all categories of HCPs. A sense of inadequate leadership, collaboration, and supplies/equipment as well as the negative impact on personal relationships and health were clearly expressed by all participants.
The pandemic’s emotional impact upon HCPs was an overwhelming source of MD/MI as supported by other research. 23 Isolation, lack of trust and connection between patients and HCPs, and the massive number of deaths despite aggressive care were significant and recurrent MD/MI themes within this study.
This study is the first to measure both MD/MI among HCPs and supports the theory that, while interrelated conceptually, their moderate but significant positive inverse relationship (r = .47, P < .001) indicated that although they share some variability, MD/MI should be viewed as different constructs. Hence, and that precise measurement of these distinct concepts requires unique instruments. Although the study was not designed to specifically test this theory, a logical inference is that if one’s MD goes unmitigated over time, it may lead to MI.12,24 Furthermore, the more intense, longer the duration, and greater exposure frequency to MD and MI, the higher the probability of burnout and leaving a position and/or the profession.
The study also revealed that a high percentage of study participants (56%) were at risk for burnout, with burnout being significantly associated with both MD/MI but with relatively modest levels of association. More specifically, when participants perceived a higher level of MD (r = .35, P < .001) and/or MI (r = .44, P < .001), they were also more likely to perceive higher burnout. Thus, the higher the MD and MI, the greater the probability of burnout. MD and MI are different constructs but are related depending on the intensity/severity of the morally distressing events. MD residue builds over time and is compounded by ongoing exposure to sources/causes. MD may lead to MI depending upon the intensity and duration of these distressing sources. MI results in psychological injury and disorders such as Post Traumatic Stress Disorder (PTSD) which is not seen with MD.
Additionally, these findings contribute to the evolving conceptual literature concerning how MD/MI may be related to resilience. Among study participants, resilience was significantly negatively inversely associated with burnout, and MD/MI was moderately positively inversely associated with burnout. This finding may explain how some HCPs are not as negatively impacted by MD and MI as well as devising strategies in mitigating MD and MI. The results are similar to a 2019 study by Krautscheid and colleagues et al, which found an inverse correlation between certain aspects of resilience and MD among nursing students at 2 universities. 25 However, the results differed from those presented in a 2021 cross-sectional study by Talebian and colleagues et al, which found a positive association between resilience and MD among critical care nurses. 26 Similarly, Clark and colleagues et al (2020) found no association between resilience and MD among emergency department nurses. 26
Our findings are similar to those of Ferreira and Gomes (2021), who found inverse relationships between burnout and resilience among physicians and nurses. 27 However, the findings are dissimilar from Shoorideh and colleagues’et al.’s (2014), which found no association between burnout and MD among critical care nurses. 28 Tetzlaff and colleagues et al (2021) found no significant association between burnout and MD among physician assistants but did find that risk of burnout was associated with increasing levels of MD. 29 A comprehensive discussion of burnout and how it relates to other concepts, such as MD, MI, is beyond the scope of this study. Taken together, the research and the cited studies indicate that the relationship between resilience, burnout and MD/MI is still evolving, which makes firm conclusions about the relationships difficult to reach. This presents a future opportunity for clearer definitions of these terms to develop more precise measurement tools.
However, the data suggest that burnout, while perhaps sharing similar characteristics, is distinct from MD/MI. This contention is supported by Cherny and colleagues et al (2015), who theorized that burnout, compassion fatigue, and MD are interrelated syndromes, each of which can lower the threshold for the development of the others. 30 Researchers posited (1) burnout occurs from stresses that arise from the clinician’s interaction with the work environment, (2) compassion fatigue evolves specifically from the relationship between the clinician and the patient, and (3) MD is related to the situation in which clinicians are asked to carry out acts that run contrary to their moral compass. 30
Nurses working during the COVID-19 pandemic showed the highest level of MD/MI and risk for burnout which is consistent with results from other studies.31,32 This is especially evident by the following nurse comment: …6 months into the pandemic recognized I was no longer thriving and was on the brink of becoming so overwhelmed I could barely recognize myself. Crying after each shift, not sleeping, nightmares, paralyzed at work when trying to manage the unmanageable, unable to eat, personal relationships taking a hit, extreme fear of getting Covid.
Learners working in the pandemic environment were also shown to have higher levels of both MD/MI compared to their attending physicians or APP colleagues working in the same environment. This compares with other studies with MD/MI risk factors as younger age,18,31 less time in practice 33 and being in a learner role in medicine. 34 This finding is consistent with Nieuwsma (2022) who showed that less empowerment in one’s practice environment increases the risk for MI. 23 Residency is already stressful; therefore, it is reasonable that learners could experience higher levels of MD/MI because of these stressors. This is supported by a resident/fellow who responded, “Teaching suffers when we are in constant crisis mode, and residents and medical students suffer the downstream effects of that.” This compares with other studies with MD/MI risk factors as younger age,18,31 less time in practice 33 and being in a learner role in medicine. 34
Limitations
A significant limitation of this study is its cross-sectional nature wherein participants reported MD/MI at a fixed point in time. The study was not designed to account for the fundamental problem of causal inference. 35 The extent of MD/MI may have impacted the results in at least 2 ways. Providers who experienced the highest levels of MD/MI may not have had the mental or emotional reserves to complete an extensive survey assessing MD/MI thus contributing to the response rate of 26% and the potential under-reporting of the presence of MD/MI. Alternatively, those experiencing the highest levels of MD/MI may have taken the opportunity to express their frustrations and perceived failures of the healthcare system, thus over-representing the extent of MD/MI. Other study limitations include a small sample size and low response rate, both of which affect the generalizability and interpretation of results as well as limited participants in specific surveyed groups, especially in lower volumes of APPs and providers who practice in the ED and surgical settings compared to medical outpatient and inpatient environments.
Future research
Further research focused on the similarities and differences between MD/MI are warranted. The impact of gender on MD/MI is a possible area of future consideration, given the stronger predictive value of female gender and MI, but not MD. Additionally, studies designed to delineate the impact of unmitigated MD and whether this leads to MI are needed. Further exploration of the benefits of enhancing coping strategies and resilience among HCPs would be beneficial to ensure that resources are directed towards the most effective preventative action plan for the reduction of MD/MI.
Conclusion
This study shows that HCPs, including all professions and levels of training, were dramatically impacted by the COVID-19 pandemic, with MD/MI being experienced by all categories of HCPs. As the understanding of these concepts increases, the lasting impact of MD/MI on the healthcare system is an area ripe for future study. Understanding the potential sources of MD/MI between different HCPs could foster widespread culture change among healthcare systems to improve HCPs’ wellbeing. Strategies need to be tailored for all HCPs with the aim of reducing MD/MI, burnout, and turnover. It is the hope that the experiences of these colleagues will contribute to a better future for all HCPs who give so much.
Footnotes
Author Note
All authors listed above have made substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND the drafting the work or revising it critically for important intellectual content; AND give their final approval of the version to be published; AND agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.