
Abstract
This study investigates depressive symptoms among spousal caregivers in three groups: those who become caregivers, those who continue care, and those who exit caregiving, compared with those who remain non-caregivers. We also examine depressive symptoms among widowed caregivers by length of bereavement. We use four waves of the U.S. Health and Retirement Study (2006, 2008, 2010, and 2012), for a total of 43,262 observations. Findings show elevated levels of depressive symptoms for new caregivers, continuing caregivers, and exit caregivers. Among exit caregivers, symptoms were elevated when measured in the first 15 months after the spouse’s death but declined thereafter. These findings add to the evidence that spousal caregiving carries a risk for depression, and symptoms are likely to peak near the end of the caregiving episode. These results underscore the need to provide support to newly widowed individuals.
For older adults who need some level of daily care outside of nursing homes—about 5.5 million Americans—the majority of care is provided informally, often by a spouse or adult child (Commission on Long-Term Care, 2013). Caregiving strain is common and may lead to burden and depression (Adelman, Tmanova, Delgado, Dion, & Lachs, 2014). A meta-analysis of 84 studies found significant differences between caregivers and noncaregivers in terms of depression, especially for spousal caregivers (Pinquart & Sörensen, 2003b). Becoming a spousal caregiver is unique in that the caregiver’s “social and marital partner is now compromised” (Seltzer & Li, 2000, p. 175). In addition, spousal care is especially intensive (Hirst, 2005; Pinquart & Sörensen, 2011), and intensive (or heavy) caregiving, usually measured in terms of hours, has been associated with higher symptoms of stress (Lyons, Cauley, & Fredman, 2015), distress (Hirst, 2005), and depression (Burton, Zdaniuk, Schulz, Jackson, & Hirsch, 2003; Cannuscio et al., 2002).
The caregiving experience varies widely, depending on many factors, including gender, the relationship between the caregiver and recipient, the amount of care provided, and care recipient behavior problems (Pinquart & Sörensen, 2003a, 2003b). Gender may also modify the association between caregiving and depression. Most studies employing a gender comparison have found depression to be higher among caregiving wives than caregiving husbands (e.g., Marks, Lambert, & Choi, 2002; Pinquart & Sörensen, 2006; Schulz & Sherwood, 2008). Because women in the general population report more symptoms of depression (Pinquart & Sörensen 2003b, 2006), cross-sectional studies may reflect a preexisting disparity.
Indeed, while caregiving research is abundant, many studies are cross-sectional, limiting the inferences that can be drawn. A number of recent longitudinal studies have focused on particular groups of caregivers, such as those caring for a relative with dementia or cancer (Kim, Shaffer, Carver, & Cannady, 2014; Ornstein, Gaugler, Zahodne, & Stern, 2014; Romero-Moreno, Márquez-González, Mausbach, & Losada, 2012; Välimäki, Martikainen, Hallikainen, Väätäinen, & Koivisto, 2015). These studies use convenience samples of those who are caregivers at baseline; hence, they cannot account for possible higher depressive symptoms before caregiving began (Hirst, 2005; Unuigbe, Lee, Vaughon, Kaufman, & Gallo, 2017). Moreover, convenience samples tend to be drawn from more distressed caregivers, and their findings may therefore differ from those of probability samples; for example, gender differences have been found to be larger in probability samples (Pinquart & Sörensen, 2006). In addition, the focus on certain conditions means that the results are less applicable to the general population. In other research, baseline depressive symptoms were an exclusion criterion (Capistrant, Berkman, & Glymour, 2014).
Longitudinal research on the transitions into and out of caregiving is needed not only to control for baseline attributes but also to examine stressful points in the caregiving trajectory. The advent of spousal caregiving—often accompanied by unfamiliar and daunting tasks—would seem to be a significant event in itself, as would the transition out of the caregiving role, especially into widowhood. Research examining the depressive effects of such transitions has been emerging but is still limited; we identified eight studies of transitions in spousal caregiving in which one of the outcome variables was depression or distress. Although several studies include the full trajectory of caregiving (entry, exit, and continuing), the findings are equivocal (Cannuscio et al., 2002; Dunkle et al., 2014; Hirst, 2005; Liu & Lou, 2017; Seltzer & Li, 2000). Differences in study design and sample composition make these studies difficult to compare, and their definitions of caregiving cover a range of intensities.
The current analysis builds on this research to better understand particular points of concern in the progression of spousal caregiving, examining depressive symptoms among men and women in three groups: those who become caregivers, those who continue care, and those who exit caregiving, compared with those who remain non-caregivers. This study contributes to the field in four ways: First, it uses a population-based sample and defines a caregiver as the primary person providing help with activities of daily living or heavy caregiving (Burton et al., 2003). Second, the study aims to strengthen the currently limited and inconclusive research on the consequences of continuing care. Third, it analyzes the transition out of spousal caregiving while controlling for widowhood. Fourth, a final analysis examines depressive symptoms among the bereaved caregivers while accounting for time since the spouse’s death, compared with exit caregivers who were not bereaved. The results may be of use in identifying caregivers most at risk of depression and targeting interventions to sensitive points in the caregiving trajectory.
Caregiving Transitions
Transitions into spousal caregiving are frequently associated with increased distress (Hirst, 2005) or depressive symptoms (Burton et al., 2003; Cannuscio et al., 2002; Dunkle et al., 2014; Marks et al., 2002; Liu & Lou, 2017), although not all studies have found a significant association (Seltzer & Li, 2000). Previous findings diverge to a greater degree at later stages of the caregiving experience. One possibility is that depressive symptoms persist or increase with continued high-intensity caregiving, based on the theory of allostatic load (McEwen & Stellar, 1993), in which sustained exposure to stressors impairs cognitive and physical functioning, in turn leading to negative effects on mental health (McEwen, 2003). An increase in depressive symptoms has some support (Burton et al., 2003), but Hirst (2005) found symptoms subsiding somewhat after the first year and back to baseline levels by the fourth year, suggesting adaptation to the role. In a study of female nurses, long-term caregivers did not show elevated symptoms (Cannuscio et al., 2002); however, women continuing care for at least 2 years did report more depressive symptoms than non-caregivers in a more recent, broader study, while men did not (Dunkle et al., 2014). The presumed advantage that nurses have through their experience with care provision may be a factor in mental health outcomes. Overall, poor health and low self-efficacy have been associated with caregiver status (Pinquart & Sörensen, 2003b).
Results are also mixed among spouses who cease caregiving, and transition studies seldom note the reason for caregiving exit, unless they are specifically studies of bereavement. We identified two exceptions: Dunkle et al. (2014) examined only couples living in the community at both baseline and follow-up; in that sample, exit caregivers reported depressive symptoms no higher than those reported by non-caregivers. And in a small Wisconsin study, bereaved caregiving wives scored much higher in depressive symptoms than noncaregivers but not significantly more than continuing caregivers (Seltzer & Li, 2000). In studies of caregivers who stop for any reason, results show inconsistent outcomes. Cannuscio et al. (2002) found improvements in mental health and well-being in the wake of caregiving, which is consistent with much of the literature on bereavement (e.g., Li, 2005; Schulz, Hebert, & Boerner, 2008), although some studies examine only dementia caregivers (Haley et al., 2008; Schulz et al., 2003). Other studies suggest that distress increases after caregiving ends (Hirst, 2005; Liu & Lou, 2017).
Important factors influencing depression trajectory in exit caregivers include previous distress levels (Aneshensel, Botticello, & Yamamoto-Mitani, 2004) and the amount of time since caregiving ended (Hirst, 2005). Failing to account for the amount of time since the spouse’s death would seem to mask a great deal of variation in depressive symptoms, yet duration of bereavement has seldom been examined in the context of caregiving research. Taylor, Kuchibhatla, Ostbye, Plassman, and Clipp (2008) focused on transitions out of caregiving due to both bereavement and nursing home placement and found high depressive symptoms immediately after the spouse’s death, but by 15 months after the death, depressive symptoms had declined substantially. Depressive symptoms also peaked following a spouse’s nursing home admission but subsequently remained elevated to a greater degree than those of the bereaved; this finding echoes that of Schulz et al. (2003).
The time frame of widowhood under study may also influence findings of gender differences in depression apart from caregiving status. Men tend to have shorter widowhoods, because of higher rates of remarriage and shorter life expectancy (Umberson, Wortman, & Kessler, 1992). Since the depressive effects of widowhood appear to dissipate over time, cross-sectional studies are likely to overstate the effects for widowed men (Sasson & Umberson, 2014). Using longitudinal data accounting for duration of bereavement, studies have found mental health effects to be equivalent among men and women who are newly widowed or soon-to-be widowed (Sasson & Umberson, 2014; Vable, Subramanian, Rist, & Glymour, 2015).
Differential Effects of Caregiving by Gender
Women have reported higher levels of caregiving stressors, such as time spent in caregiving (Yee & Schulz, 2000) and the care recipient’s impairment or behavioral problems (Pinquart & Sörensen, 2006). As a result, gender differences in caregiving stressors exacerbate the disparity in depression reported (Pinquart & Sörensen, 2006). A greater burden of care and more time spent in care and the performance of more personal tasks is associated with more negative psychological effects for women (Yee & Schulz, 2000).
Women and men may take different approaches to caregiving and have different expectations of themselves as caregivers; women may also receive more or less support than caregiving men (Yee & Schulz, 2000). The traditional roles of women as care providers and men as task-oriented workers or managers may figure into caregivers’ expectations of themselves and the way the work should be done (Calasanti & King, 2007). In this framework, a man may view caregiving as accomplishing tasks, such as getting his wife dressed, and may try to separate his emotions from the work at hand. At the same time, he might receive praise for efforts that transcend the typical masculine role. In contrast, a woman may see her responsibility as meeting all of her spouse’s needs—potentially a more difficult, if not impossible, goal—and may perceive shortcomings in her expected role as a nurturer. Women also may be more subject to outside criticism of their performance (Navaie-Waliser, Spriggs, & Feldman, 2002). Such different expectations could also affect one’s willingness to accept respite and take time for exercise and social life (Burton, Newsom, Schulz, Hirsch, & German, 1997), both factors that are associated with positive mental health outcomes in older adults (Arent, Landers, & Etnier, 2000; Thompson, Futterman, Gallagher-Thompson, Rose, & Lovett, 1993).
Traditional gender roles may also emerge in the behavior of the care recipient, resulting in greater burden for women (Pinquart & Sörensen, 2006). Older men in traditional households may not want to relinquish control and may become more demanding; in contrast, women’s experience may make them more appreciative of the effort required by caregiving (Davidson, Arber, & Ginn, 2000).
Finally, caring for a spouse often also results in benefits to well-being, and some researchers have hypothesized that these may not be experienced or perceived equally among men and women (Marks et al., 2002; Yee & Schulz, 2000). There is some evidence that a “sense of meaning and accomplishment” from personal care of a spouse accrues to women more than to men (Freedman, Cornman, & Carr, 2014, p. 867).
Yet it is important not to overemphasize such generalizations about gender. Older male caregivers have also reported a sense of isolation and invisibility, and male and female caregivers are much more alike than different (Calasanti & King, 2007; Pinquart & Sörensen, 2006). Moreover, Pinquart and Sörensen (2006) observed a narrowing of the gender gap in caregiving stressors in more recent years.
In recent longitudinal research, the role of gender is less clear. Greater depressive effects of caregiving on women than on men have sometimes been found to persist after controlling for baseline levels (Dunkle et al., 2014; Hirst, 2005), but in one study depression levels for women in the heavy caregiver group were elevated even before such caregiving began, perhaps for reasons related to the imminent caregiving (Hirst, 2005). Other researchers found no gender differential effect (Taylor et al., 2008), and a German study using fixed-effects models found much higher mental health effects for caregiving husbands (Hajek & König, 2016).
Longitudinal research on caregiving transitions in the United States remains limited. Two of the studies cited earlier are from other countries (Hirst, 2005; Liu & Lou, 2017), and in other studies, the sample is not nationally representative (Burton et al., 2003; Cannuscio et al., 2002; Seltzer & Li, 2000). Among studies that use a large U.S. population sample, two examine only transitions into caregiving (Marks et al., 2002) or out of it (Taylor et al., 2008), and both of these studies consider a broader range of caregiving intensity. Dunkle et al. (2014) addressed all these factors but excluded widows. Finally, most work has been done with data from the 1990s.
To contribute to the understanding of depression along the caregiving trajectory, the present study explores two main research questions: (a) How do depressive symptoms differ for individuals who become primary caregivers for a spouse with daily needs, who continue such caregiving, or who exit such caregiving, compared with those who do not provide care? (b) If depressive symptoms are elevated at the time of bereavement, do they abate with time, and to what degree?
Method
Sample
The U.S. Health and Retirement Study (HRS) is a panel study of a nationally representative sample of adults 50 and over living in the community, sponsored by the National Institute on Aging (grant number NIA U01AG009740) and conducted by the University of Michigan (Health and Retirement Study, 2012; RAND, 2015). The present study uses data from four waves of the survey, in 2006, 2008, 2010, and 2012; each longitudinal observation contains baseline data from one wave and follow-up data from the next wave. Our sample is limited to respondents aged 50 and older with observations, including a measure of depression, at two consecutive waves, who were not parental caregivers at baseline or follow-up. These selection criteria resulted in a sample of 20,207 respondents and 43,262 observations.
Attrition is not high in the HRS, but 3.7% of the sample present in the 2006 wave did not participate in the 2008 wave or consecutive waves thereafter (up to 2012) and are therefore not included in the sample. These individuals were significantly different from the sample in most characteristics; overall, they were older and more likely to be male, less likely to be married or employed, and less healthy. HRS respondents excluded for missing Center for Epidemiological Studies Depression Scale (CES-D) variables (7.6% of the observations) had a similar profile, except that there was no difference in marital status. Among sample members, about 10% dropped out after the first or second wave pair. These individuals were older and more likely to be male, Hispanic, and widowed, with less wealth and education and more activities of daily living (ADL) impairment; they were less likely to be married, employed, healthy, and active.
Measures
The dependent variable in this analysis is depressive symptoms, measured as a count variable by the respondent’s score on an eight-item version of the commonly used CES-D. The score is the total of responses to six unfavorable indicators (always or much of the time feeling depressed, sad, or lonely, feeling that everything is an effort, feeling unable to get going, or having restless sleep) and two favorable indicators (feeling happy, enjoying life), with the favorable indicators reverse scored (Chien et al., 2015). The scale is 0 to 8, with 8 representing the highest level of depressive symptoms. The original CES-D consists of 20 items and has been clinically validated (Radloff, 1977). The reliability and internal consistency of the eight-item CES-D instrument in the HRS sample have also been established in research with the HRS data (Steffick, 2000), and Cronbach alpha coefficients for baseline and follow-up depression scores have been assessed at .82 and .88, respectively (Gallo, Bradley, Siegel, & Kasl, 2000). The eight-item CES-D has also been assessed from a gender perspective (Van de Velde, Levecque, & Bracke, 2009). While the eight-item CES-D does not include an established cutoff point for a diagnosis of depression, some researchers have suggested using a score of 3 (Turvey, Wallace, & Herzog, 1999).
The primary independent variable is whether a respondent was the caregiver of a spouse at baseline or follow-up. Respondents fall into four categories: those who began caregiving after baseline (entry caregivers), stopped caregiving after baseline (exit caregivers), remained caregiving from baseline to follow-up (continuing caregivers), or were not providing spousal care at either point (non-caregivers). Spousal caregiver status was established by first identifying respondents who reported needing help with ADLs (dressing, eating, bathing, walking across a room, or getting in or out of bed) and who identified their spouse as the primary caregiver and then labeling that spouse as a caregiver. Virtually all spousal caregivers were coresident; fewer than 1% identified themselves as “married, spouse absent.”
Covariates include baseline CES-D score, marital status, age, race/ethnicity, education, current employment, household assets (excluding primary residence), self-reported health, limitations in mobility and ADLs, physical activity, and whether the care recipient had been diagnosed with dementia. Age was treated as a continuous variable. Dummy variables were created for marital status, race/ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, other), education, employment, and good health. For marital status, “married” includes those who define themselves as “married,” “married, spouse absent,” and “partnered”; dummy variables were also created for widowed, divorced/separated, and never married. Education is categorized, according to responses, as less than high school, high school (including responses “GED” or “high school graduate”), some college, and college graduate. Employment represents the respondent’s answer to the question “Are you currently working for pay?”
Overall, poor health has been associated with caregiver status (Pinquart & Sörensen, 2003b); this is accounted for through self-reported health as well as mobility and ADL limitations, given that such limitations can be expected to make care work more difficult. Self-reported health was recoded to a dichotomous variable with excellent, very good, or good the referent. ADL limitations are represented in an index (0–5) of yes/no answers to questions about difficulty performing the five ADL tasks listed earlier. Mobility (0–5) is constructed in the same way for the following five tasks: walking several blocks, walking one block, walking across the room, climbing several flights of stairs, and climbing one flight of stairs. Physical activity is determined by frequency of moderate physical activity, reverse-coded so that 4 = daily, 3 = more than once per week, 2 = once per week, 1 = one to three times per month, and 0 = never. The spouse’s dementia status is a dichotomous variable based on the answer given by the respondent’s spouse to the question “Has a doctor ever told you that you have a memory-related disease?” in Waves 8 and 9; in Waves 10 and 11, the question was expanded to two questions, specifying Alzheimer’s disease or dementia. The value was coded as missing for unmarried respondents. Household assets are reported as the median in descriptive statistics but are represented in thousands of dollars in the regression analyses.
Analysis
The analyses are stratified by gender. Descriptive statistics of the entire sample and subgroups by gender are presented at each respondent’s first baseline (2006, or at entry into the sample if later than 2006). For the main longitudinal analyses, we combined the three pairs of waves and used a repeated measures adjustment for intrasubject correlation (Zeger & Liang, 1986). Because CES-D score is a count variable with nonnormal distribution, we estimated a negative binomial regression model (Byers, Allore, Gill, & Peduzzi, 2003), with non-caregivers as the reference group. Stratifying the sample by gender, we fitted models for entry caregivers (424 women, 341 men), exit caregivers (435 women, 375 men), and continuing caregivers (325 women, 298 men) compared with noncaregivers (24,192 women, 16,892 men). We report both unadjusted models and a model adjusted for all covariates as well as survey year and attrition (dropping out of the sample after participating in at least one wave pair).
For the separate regression analysis of exit caregivers (N = 808), we compared widowed caregivers with nonwidowed caregivers based on the length of time since the death of the care recipient: 0–3 months, 3–15 months, and more than 15 months. These durations were chosen primarily for consistency with Taylor et al. (2008), in order to promote comparability of data. Because of the smaller sample size, we present results for the total sample as well as for men and women separately, in both unadjusted and adjusted models. Two widowed exit caregivers without a reliable date of spouse’s death were excluded from this analysis. All statistical analyses use a significance level of 5%. Analyses were performed with SAS version 9.4 (SAS Institute, Cary, NC).
Results
Characteristics of the Sample at Baseline
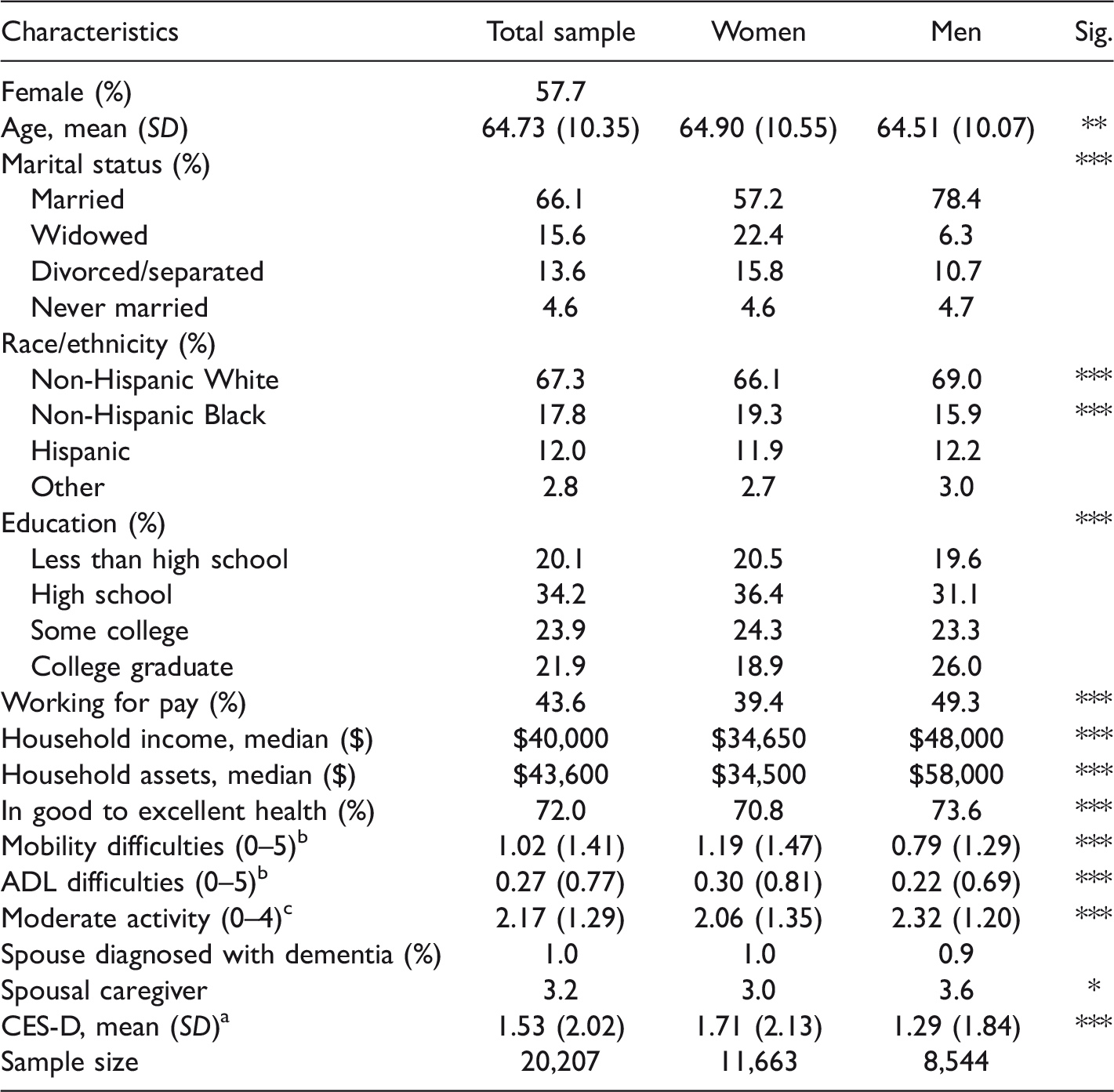
Table 1 shows participant characteristics in 2006, or at entry into the sample if later than 2006 (30%). The sample population is predominantly female, averaging 65 years old. Two thirds are married, and two thirds are non-Hispanic White. One third have a high school degree and no further education, and the remaining two thirds are about evenly split between those with no high school diploma, those with some college, and college graduates. Median household income was $40,000, and median household assets were $43,600. Self-rated health was good, very good, or excellent for 72% of the sample. Just 1% had a spouse diagnosed with dementia at baseline (1.5% among married individuals; not shown), and 3% of the sample were spousal caregivers. The overall mean CES-D score was 1.53.
Demographic Characteristics of the Sample at Baseline.
Note. Sample represents population at baseline in 2006 (n
aCES-D score is on a scale of 0–8, with 8 representing the highest level of depression symptoms.
bIndex represents number of mobility impairments or impairments in ADLs.
cModerate activity index: 4 = daily, 3 = more than once per week, 2 = weekly, 1 = 1–3 times per month, 0 = never.
*p < .05. **p < .01. ***p < .001.
Men and women differed significantly on all characteristics except Hispanic ethnicity, identifying as “other” race, and having a spouse with dementia. Men were slightly younger, more likely to be married, and less likely to be widowed, and a greater proportion were spousal caregivers. A larger share of men were working for pay (49% of men vs. 39% of women), and men reported significantly more education and greater household income and assets. Women were in worse health and had markedly more symptoms of depression (CES-D of 1.71 vs. 1.29 for men).
Entry Caregivers
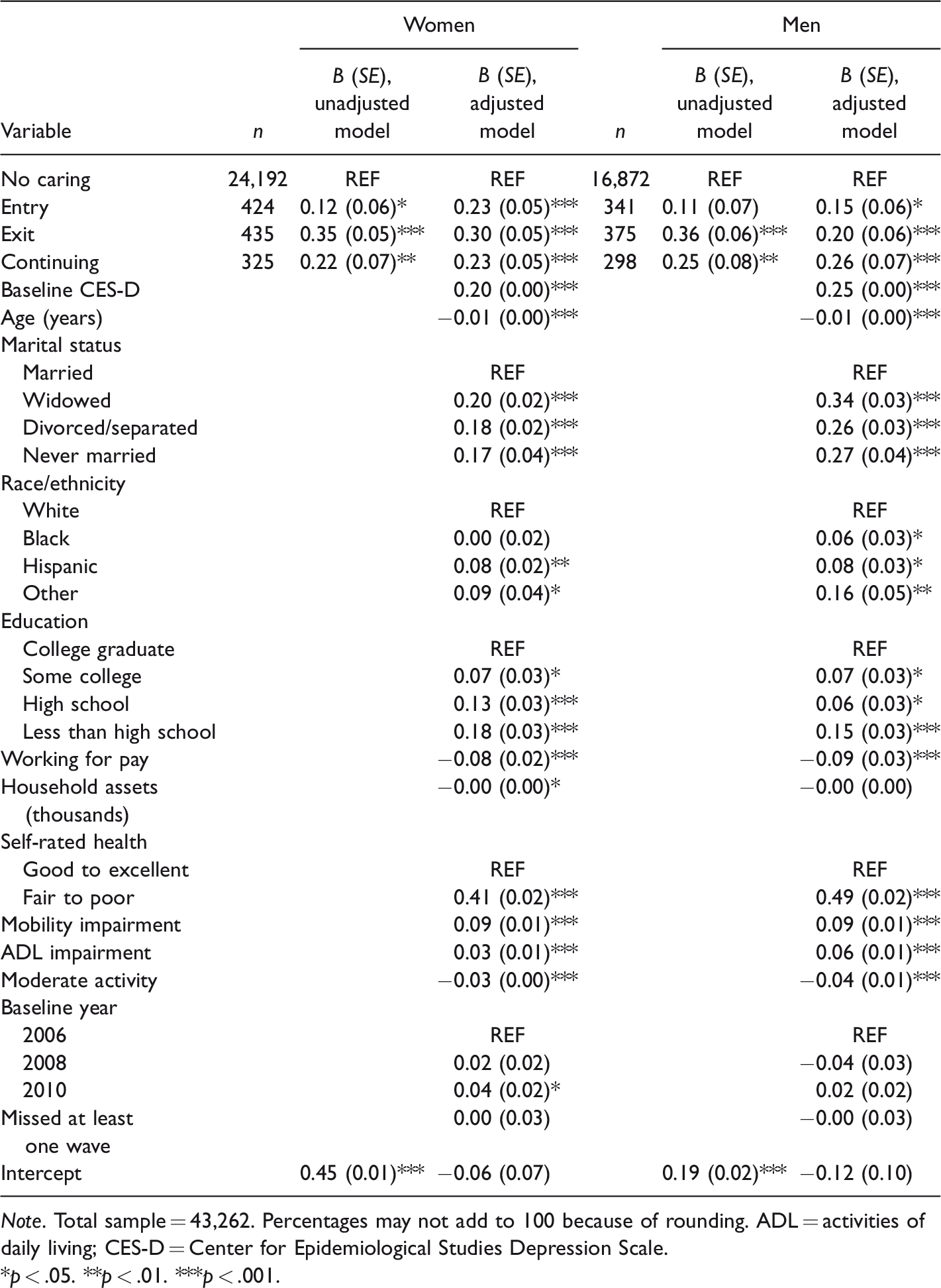
As shown in Table 2, both women and men who became spousal caregivers had significantly higher depressive symptoms at follow-up than non-caregivers after adjusting for all covariates (among women, B = 0.23, p < .001; among men, B = 0.15, p = .025).
Regression Analysis of Depressive Symptoms, by Type of Caregiving Transition and Gender.
Note. Total sample = 43,262. Percentages may not add to 100 because of rounding. ADL = activities of daily living; CES-D = Center for Epidemiological Studies Depression Scale.
*p < .05. **p < .01. ***p < .001.
Nearly all the covariates had significant associations with depressive symptoms as well, with the exception of household assets and most of the interview participation variables. Among dichotomous variables, negative mental health was predicted notably by baseline CES-D, fair to poor health, and being unmarried.
Continuing Caregivers
Women and men who were spousal caregivers at both baseline and follow-up also showed a higher level of depressive symptoms than noncaregivers in the fully adjusted model (among women, B = 0.23, p < .001; among men, B = 0.26, p < .001).
Exit Caregivers
Women and men who made the transition out of spousal caregiving over a 2-year period also showed significantly higher depressive symptoms at follow-up than those who did not provide care (among women, B = 0.30, p < .001; among men, B = 0.20, p < .001). Additional multivariable regression models examined depressive symptoms between continuing caregivers and entry caregivers and between exit caregivers and continuing caregivers (results not shown). No significant differences were found.
Table 3 examines exit caregivers by length of time since the care recipient’s death, compared with exit caregivers who were not bereaved. Almost one third of exit caregivers were bereaved. For exit caregivers interviewed within 3 months of the spouse’s death, there was a notable association with depressive symptoms (B = 0.65, p < .001), which was significant for both women (B = 0.65, p < .001) and men (B = 0.57, p = .006). For exit caregivers bereaved between 3 and 15 months, depressive symptoms were still elevated compared with those not bereaved (B = 0.45, p < .001). While the subgroup of women in this category also shows an association (B = 0.50, p < .001), men bereaved in the medium term did not show a significant increase in depressive symptoms compared with their still-married counterparts (B = 0.30, p = .128). And finally, among those bereaved more than 15 months, the association with depressive symptoms was no longer significant (B = 0.14, p = .243) for the group as a whole or for men and women separately. Additional multivariable regression models tested depressive symptoms between the groups of bereaved caregivers; no significant difference was found between the newly bereaved and those bereaved in the middle term, but the long bereaved showed significantly lower symptoms of depression than those in the middle category (B = −0.27, p = .037).
Regression Analysis of Depressive Symptoms in Exit Caregivers, by Length of Bereavement.

Note. Percentages may not add to 100 because of rounding. One female exit caregiver and one male exit caregiver were excluded because of an absent or unreliable date of bereavement. ADL = activities of daily living; CES-D = Center for Epidemiological Studies Depression Scale.
*p < .05. **p < .01. ***p < .001.
Among exit caregivers, covariates showing positive association with depression in the full sample were baseline CES-D, fair to poor health, and being in the final wave pair (2010 baseline); negative associations with depression were significant for being non-Hispanic Black and working for pay. In the sample of women, the only significant covariates were baseline CES-D, moderate activity, and baseline year. In the sample of men, significant positive associations were found for baseline CES-D, fair to poor health, and mobility impairment, and significant negative associations were found for being non-Hispanic Black and working for pay.
Discussion
This study used a national sample to examine the degree to which transitions in caregiving and continued caregiving for a spouse are associated with symptoms of depression. Findings show elevated levels of depressive symptoms for entry caregivers, continuing caregivers, and exit caregivers of both genders. Among exit caregivers, symptoms were significantly lower by 15 months after bereavement than among the more recently bereaved.
The first research question concerned the depressive effects of three caregiving conditions. The association of depression with entry into caregiving among women is significant; among men, it is significant but weak. The association does not subside for continuing caregivers of both genders, even after controlling for baseline mental health, which is consistent with Burton et al. (2003) and Seltzer and Li (2000). This is in contrast to studies that suggest adjustment to the role (Cannuscio et al., 2002; Liu & Lou, 2017). Because the period studied is only 2 years, these results do not directly contradict other work that found amelioration over a longer period of caregiving (Hirst, 2005). The gender difference found in Dunkle et al. (2014), in which women but not men showed greater depressive symptoms, is not supported here. Among exit caregivers, almost one third were bereaved. Controlling for widowhood, depressive symptoms were greater than for non-caregivers, as predicted by Hirst (2005) and Liu and Lou (2017).
On the caregiving variables in the full sample, no significant difference between men and women was found. As discussed in the introduction, the potential contributors to gender differences in the effects of caregiving include the intensity of care provided, coping methods, care recipient behavior, and preexisting depression. With caregiver defined as the primary helper with a spouse’s ADLs, and controlling baseline CES-D scores, gender differences in the current study appear to be negligible. This study uses more recent data than similar research, and it is possible that the influence of gender roles is waning in the later generations.
This study also asked whether depressive symptoms eventually abate for those who cease caregiving. Comparing depressive symptoms by length of time bereaved versus exit caregivers who were not bereaved, the results suggest that depressive symptoms are likely to peak around the time of the spouse’s death, although the findings here are not conclusive on that question. On average, caregivers widowed for more than 15 months have depressive symptoms no greater than exit caregivers whose spouses have recovered or made a transition into different care arrangements. These findings strongly support those of Li (2005) and Taylor et al. (2008). Considering bereavement status and length of bereavement when examining depression among exit caregivers reveals a great deal of variation that has been masked in previous studies that could not specify why the caregiving ended.
Overall, the results of this study suggest a trajectory in which depressive symptoms begin after the onset of spousal caregiving; possibly increase with the strain of continued caregiving and perhaps the declining health of the care recipient, consistent with the theory of allostatic load; and peak around the time of caregiving exit, if it coincides with bereavement. Among bereaved caregivers, symptoms appear to decline with time, suggesting that resilience is the rule.
This study contributes to the literature in this area by examining depressive symptoms across the entire trajectory of caregiving as well as in the postbereavement period, allowing a comparison of newly bereaved, long bereaved, and nonbereaved exit caregivers. In combination with Taylor et al. (2008), it suggests that differing results in previous research may be due in part to the conflation of postcaring experiences. Trends among men are consistent with those among women. The findings among continuing caregivers and exit caregivers may reflect both caregiver burden and anticipatory grief (Vable et al., 2015).
The eventual easing of depressive symptoms found here does not contradict evidence that caregivers’ individual trajectories are likely to vary. Bereaved dementia caregivers in one study showed four distinct trajectories of symptoms, with only about one in five showing the pattern observed here (Aneshensel et al., 2004). Li (2005) found moderating elements in low income; in problematic behavior by the care recipient, which seemed to slow recovery after bereavement, perhaps due to depletion of resources; and in caregiver feelings of overload, which may have promoted a feeling of relief. Given the intensity of spousal caregiving and the presumed bond between spouses, it is possible that the course of illness drives the caregiver to devote herself or himself more and more to that relationship and caregiving duties, to the exclusion of outside social life (Drentea, Clay, Roth, & Mittelman, 2006). The resilient trajectory therefore may represent a restoration of leisure and social contact (Seltzer & Li, 2000); if so, it is important to provide support to widows who may be more isolated or financially burdened. The timing of depressive symptoms may also be affected by the presence of dementia on the part of the care recipient, which may give rise to prolonged grief before caregiving ends (Ott, Sanders, & Kelber, 2007), in turn affecting depressive symptoms in bereavement (Aneshensel et al., 2004).
In corroborating the evidence that symptoms peak just before and after bereavement, this study supports two principles. First, preventive care should be offered to caregivers before the death of the spouse (Schulz et al., 2008). Second, depressive symptoms continuing for more than a year may signal complicated grief. In the case of complicated grief, cognitive behavioral therapy specifically tailored toward loss has shown better results than standard interpersonal therapy (Shear et al., 2014). The condition has been identified as a stress response syndrome, and cognitive grief therapy is modeled on the prolonged exposure therapy used with posttraumatic stress disorder.
Given the possibility that allostatic load caused by prolonged stress may be a factor in caregiver depression, future research could examine the relationship between caregiving and complicated grief. It would be beneficial to continue to parse the characteristics and circumstances that may predict the onset or worsening of depression, including health behaviors and their cumulative impact. Research on the time-varying influence of covariates would help illuminate the potential bidirectionality between such conditions as depression and physical health. Even if depressive symptoms ease with the passing of grief, they may lead to negative physical effects that persist.
While this study did not find strong evidence that services should target men or women in particular, the influence of gender roles remains an important question, and one that may vary in future cohorts (Pinquart & Sörensen, 2006). It is also important to consider whether certain interventions may be more effective for men or women, who may respond to different approaches (Yee & Schulz, 2000).
Strengths and Limitations
Notable strengths of this study include its observation of the transition into and out of caregiving and length of bereavement, adjustment for pre-caregiving depressive symptoms, and the use of population-based data. Research examining men and women separately often includes both adult child and spousal caregivers, or includes spouses who provided varying degrees of care, but higher effects among women have been partly attributed to differences in time spent and type of caregiving tasks. This study, restricted to primary caregivers assisting with ADLs, examines men and women with more similar care burdens. It also updates the literature with more recent data.
The study has several limitations worthy of mention. Given the complex and dynamic nature of the caregiving relationship, there are plausibly many unobserved covariates. Informal caregiving is measured dichotomously and through the recipient's report. While the nature of primary assistance with ADLs is intensive, the number of hours of care is not measured, nor is caregiver assistance from other informal sources or from paid home care taken into account. Attributes of the care recipient’s functionality and behavior are not controlled; in particular, it would be valuable to control for dementia on the part of the care recipient, but that information was often missing, especially in cases where the care recipient had died. In addition, although the main analysis controls for widowhood, the data do not include a consistent measure of duration of widowhood in the overall sample, which no doubt varies widely among the non-caregiving comparison group. Other factors thought to be important in moderating depression in older adults, such as social support, contact and relationships with adult children, and social and religious participation, were measured for only a portion of the sample in any given wave and were therefore omitted from the analysis.
Attrition in the HRS is not high, but the attrition that exists, along with the exclusion of respondents without CES-D scores, is likely to bias results away from the mean. The exclusion of parental caregivers, who have been shown to experience elevated depressive symptoms in some studies, but not all (e.g., Cannuscio et al., 2002; Hajek & König, 2016), is expected to do likewise, although only slightly given their relatively small number. Finally, in the analysis by length of bereavement, sample sizes are small, and the significance of covariates is particularly vulnerable to noise, for example, in the fairly large association of race with depressive symptoms in men.
Conclusions
While these limitations somewhat restrict our ability to interpret the results, this analysis nonetheless adds evidence that depression may rise in a population that faces greater caregiving responsibilities. There are more than 43 million informal caregivers of older people in the United States, and with the population age 65 and older expected to reach 20% by 2030, that number will surely increase (National Alliance for Caregiving & AARP, 2009; Ortman, Velkoff, & Hogan, 2014). Understanding the possible trajectory of caregiver depression and burden will allow practitioners and policy makers to target interventions to the most critical points of the spousal caregiving experience. Although the average estimated effect of caregiving transitions on depression is not large, it may have practical significance, especially for former spousal caregivers in their first year of widowhood. These results underscore the need to provide support to newly widowed individuals, especially those whose well-being may have been reduced over the course of the spouse’s illness. This research adds to the evidence that caregiver support is needed, but it is also consistent with the idea that caregiver burden can be managed.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.