
Abstract
This study identified profiles of health behaviors among Korean baby boomers and examined a set of individual characteristics associated with these latent profiles. We analyzed a sample of 4,047 middle-aged adults (aged 53–61) from the Korean Baby Boomer Panel Study (2014). Latent profile analysis was used to uncover distinct health behavior profiles, and multinomial regression was performed to investigate the associations between health behavior profiles and predisposing, enabling, and need factors—following from the behavioral models of health behaviors and health services use. Five profiles of health behaviors were identified: (a) low-risk and high-preventive behaviors (50%), (b) low-risk and low-preventive behaviors (35%), (c) moderate-risk and moderate-preventive behaviors (7%), (d) moderate-risk and high-preventive behaviors (6%), and (e) high-risk and low-preventive behaviors (2%). Further, individuals with more enabling and need characteristics, indicated by higher socioeconomic status and greater health concerns, were more likely to engage in healthier profiles.
Introduction
Korean baby boomers constitute a set of birth cohorts born after the Korean War between 1955 and 1963. These baby boomers represent 15% of the total Korean population (Han et al., 2011). Compared with baby boomers in the United States who are beginning to enter later life, Korean baby boomers are younger and considered to be middle-aged (ages 53–61). For many middle-aged persons, this period of the life course represents a transition time from peak performance of youth to early stages of decline in physical and mental abilities (Jokela et al., 2010). Most adults begin to notice age-related changes around this time, such as changes in their physical appearance (e.g., increased body weight and wrinkles), as well as other physiological changes (e.g., less endurance). However, individuals’ experiences with these changes vary greatly, in part due to their genetic makeup and health behaviors (Merrill & Verbrugge, 1999). Because genetic makeup cannot be altered, scholars have pointed to the importance of health behaviors in early adulthood and midlife to help understand overall health and well-being (Umberson, Crosnoe, & Reczek, 2010). Indeed, research shows that health behaviors in midlife are linked to the rate of physical decline and various health outcomes in later life, including longevity (Kim, 2011; Lachman & Agrigoroaei, 2010).
This study has two aims. The first aim is to identify profiles of health behaviors among Korean baby boomers. Health behaviors may be either risk inducing or preventive in nature. We considered two risk-inducing behaviors (i.e., alcohol consumption and smoking) and four preventive behaviors (i.e., exercise, supplement intake, herbal medicine intake, and biannual physical examinations). This set of health behaviors is relevant within the cultural context of Korean baby boomers. These risk-inducing and preventive health behaviors may be grouped together in unique ways. By using a person-centered approach, we formulated distinct profiles of risky and preventive health behaviors to capture more efficiently the array of individuals’ health behaviors identified in this study.
The second aim is to examine individual characteristics associated with the profiles of health behaviors among Korean baby boomers. Drawing on behavioral models of health behaviors and health services use (Andersen, Davidson, & Baumeister, 2013; Ma, Shive, Gao, Tan, & Wang, 2012), we focused on individual characteristics, reflecting predisposing, enabling, and need factors. Health behavioral models have provided a helpful framework for organizing different dimensions of factors associated with health behaviors and health outcomes in diverse contexts and cultures (Andersen et al., 2013).
Health Behavior Profiles
The first contribution of this study is the identification of health behavior profiles among Korean baby boomers. Most studies of health behaviors focused on a specific behavior (e.g., smoking or alcohol consumption) or pairwise associations between health behaviors (e.g., physical activity and sedentary behaviors; Noble, Paul, Turon, & Oldmeadow, 2015). Recently, research has paid more attention to unique combinations of different risky and preventive health behaviors (McAloney, Graham, Law, & Platt, 2013). On the other hand, some health-risk behaviors (e.g., alcohol consumption) appeared to be accompanied by preventive behaviors (e.g., physical activity), potentially reducing harmful effects from risky behaviors (Leasure, Neighbors, Henderson, & Young, 2015). Thus, the investigation of health behaviors as profiles that included multiple activities has the potential to provide a synergistic approach. The importance of identifying health behavior profiles also has been highlighted in recent research on U.S. populations (Olson, Hummer, & Harris, 2017; Shaw & Agahi, 2012). However, to the best of our knowledge, the identification of multidimensional health behavior profiles among Korean baby boomers has rarely been studied.
In this study, we used six indicators of health behaviors to identify latent health behavior profiles among Korean baby boomers, including two risk-inducing behaviors (i.e., alcohol consumption and smoking) and four preventive behaviors (i.e., exercise, nutritional supplement intake, herbal medicine intake, and physical examinations by a healthcare professional). Alcohol consumption and smoking are widely studied measures of risk-inducing behaviors (Heath et al., 2012; Solberg, Maciosek, & Edwards, 2008). Research shows that alcohol consumption and smoking have been leading causes of mortality and morbidity (Pruchno, Hahn, & Wilson-Genderson, 2012; Roerecke & Rehm, 2014). Korean culture is characterized by a long tradition supporting the consumption of alcohol in social and work settings, often involving consuming large amounts of alcohol, sometimes regardless of individuals’ alcohol consumption preferences (Kim, 2002; Park & Lee, 2011). The smoking rate in South Korea was about 17% in 2015, which is similar to other developed countries in the Organisation for Economic Co-operation and Development, but significant gender differences exist (31.4% for men vs. 3.4% for women; Organisation for Economic Co-operation and Development, 2018). Studies indicate that the co-occurrence of smoking and alcohol consumption increased the risk of poor health outcomes (Oliver et al., 2013).
In the context of physical changes that occur during the aging process, middle-aged adults may adopt various preventive health behaviors to maintain or enhance their health status. Engaging in regular exercise, receiving routine physical examinations from healthcare providers, and consuming nutritional supplements are regarded as health-promoting behaviors (Heath et al., 2012; Solberg et al., 2008). Evidence suggested that exercising lowers the risk of chronic disease (Reiner, Niermann, Jekauc, & Woll, 2013). Along with exercising, nutritional supplements (e.g., vitamin D and calcium) have been shown to have beneficial effects for health among middle-aged adults (Brock et al., 2010; Kim & Choi, 2016). Similarly, physical examinations performed by doctors and other healthcare professionals are known to be helpful in detecting chronic and acute diseases, and these examinations offer an opportunity to learn about health promotion options.
The middle-aged Korean population has shown a high rate of participation in biannual physical examinations due to the Korean national health insurance system that provides financial support for a wide range of medical services (e.g., cancer screenings and blood tests) for adults over age 40 (Lee, Lim, & Park, 2010). Herbal medicines have been used in Asian countries for over 2,000 years (Wang, Li, Devinsky, Schachter, & Pacia, 2005), and more than 60% of the Korean population reported that they had taken herbal medicine at least once during their lifetime (Hyun, Lee, & Ryu, 2015). Given the cultural relevance of nutritional supplement use, examining herbal medicine intake may be useful for gaining a better understanding of health behaviors among Korean baby boomers.
Based on combinations of these risk-inducing and preventive behaviors present in the Korean context, as well as the empirical evidence discussed earlier, we expected to observe distinct health behavior profiles among Korean baby boomers (Hypothesis 1). Specifically, we expected healthy profiles to be characterized by low-to-moderate risk and high-preventive health behaviors and unhealthy profiles to be characterized by high-risk and low-preventive health behaviors. We also expected some Korean baby boomers to show compensatory profiles reflecting advantageous effects of preventive behaviors, such as high-risk and high-preventive health behaviors (Ernsting, Schwarzer, Lippke, & Schneider, 2013; Radtke, Scholz, Keller, Knäuper, & Hornung, 2011). Finally, we expected a low engagement pattern of low-risk and low-preventive health behaviors, whereby Korean baby boomers with this pattern will show low levels of engagement in the types of health behaviors investigated here.
Factors Associated With Health Behavior Profiles
For the second aim of this study, we examined factors associated with Korean baby boomer health behavior profiles. These analyses were guided by the behavioral models of health behavior and health services use (Andersen, 1995; Andersen et al., 2013; Ma et al., 2011, 2012). These behavioral models recognize that health behaviors are complex and influenced by multiple factors, encouraging researchers to consider cultural and interpersonal environments, as well as individual determinants.
Further, these behavioral models suggested different types of factors may contribute to health behaviors and that may ultimately have consequences for health outcomes; these include predisposing, enabling, and need characteristics. Predisposing characteristics are defined as conditions not directly responsible for health services use or health behaviors, such as demographic, social, and personal belief factors. Enabling characteristics are identified as resources that facilitate or impede health service use and health behaviors, such as income and education. Need characteristics were actual and perceived need for medical care.
Predisposing factors
This study examined demographic characteristics (i.e., age, gender, and marital status) and beliefs (i.e., mastery) as predisposing factors, which are shown to be associated with variability in health services use and health behaviors (McAloney et al., 2013). For example, older women were more likely to engage in preventive health behaviors than older men (Deeks, Lombard, Michelmore, & Teede, 2009). Compared with nonmarried individuals, married individuals reported their health in more positive terms (Zheng & Thomas, 2013) and were more likely to engage in health-preventive behaviors (Umberson, 1987).
Beliefs, attitudes, values, and knowledge also appear to have influenced perceptions about need for health behaviors and engagement in specific health behaviors. Mastery refers to how individuals viewed their ability to control their life circumstances (Pearlin & Schooler, 1978). High levels of mastery were associated with making positive health behavior changes, such as exercising and engaging in preventive care (Skaff, 2007). People with a higher level of mastery (e.g., belief in one’s ability to quit smoking) also were more likely to be successful in achieving their goals (Haidt & Rodin, 1999). Although the consequences of lifestyle changes are often not ultimately influential if they were not maintained, a higher level of mastery may help to initiate and maintain these behavioral changes (Bandura, 1997). A low sense of mastery was associated with less self-initiated preventive care, less optimism in early treatment phases, and more episodes of illness (Lachman, Neupert, & Agrigoroaei, 2011; Seeman & Seeman, 1983). Based on the empirical literature these two models, we expected that Korean baby boomers who are older, female, married, and reported higher levels of mastery will engage in healthier behavior profiles characterized by high-preventive and low-risk behaviors (Hypothesis 2a).
Enabling factors
We considered three specific enabling resources, including education, income, and employment status. Compared with individuals with fewer resources, individuals with more resources (i.e., higher educational attainment, higher income levels) are shown to be more likely to engage in healthy behaviors (e.g., exercise) and take advantage of health services (e.g., obtaining annual physical checkups; McAloney et al., 2013). In addition, employment may provide financial resources and opportunities for engaging in exercise (e.g., access to fitness centers). In this study, we expected Korean baby boomers with more socioeconomic resources (i.e., higher education, higher income, and currently working) will engage in healthier behavior profiles characterized by high-preventive behavior profiles (Hypothesis 2b).
Need factors
This study also examined actual (i.e., number of chronic diseases and depression) and perceived (i.e., health concerns) health conditions as need factors. Studies have shown that health conditions are associated with engagement in preventive health behaviors and use of health services (Ellis, Orom, Giovino, & Kiviniemi, 2015). Individuals with chronic health conditions are more likely to see a doctor and adhere to prescribed therapies. Individuals with chronic health conditions may also find exercising difficult, and thus, they may be less inclined to engage in this behavior. Conversely, individuals in better physical condition may be less likely to engage in unhealthy behaviors, such as sedentariness. Regarding mental health status, evidence suggests that depressed adults were more likely to smoke and less likely to have nutritious diets (Ellis et al., 2015).
As a need factor, perceived health status may also be associated with engaging in healthy behaviors. Research suggested that intense health-related concerns serve as a major source of stress and may be related to poor health outcomes (Lachman et al., 2011). Studies based on clinical samples also indicated that health anxiety is linked to negative health behaviors (e.g., not engaging in treatment; Anttila, Knuuttila, Ylostalo, & Joukamaa, 2006; Skidmore, Dyson, Kupper, & Calabrese, 2014). However, health concerns that come from perceived lower health status may motivate individuals to engage in preventive behaviors. Regarding these need factors, we expected that Korean baby boomers with worse physical and mental health conditions and higher levels of health concerns will engage in healthier behavior profiles characterized by high-preventive behavior profiles (Hypothesis 2c).
Methods
Data Source and Study Sample
This study was based on data from Wave 3 of the Korean Baby Boomer Panel Study, which is a prospective survey of Korean baby boomers (born between 1955 and 1963) residing in urban areas in Korea (Han et al., 2011). The Korean Baby Boomer Panel Study collected the first wave of data in 2010, which included various life domains of community-residing households and individuals, such as health, financial status, retirement status, and social participation. For the data collection from community-dwelling baby boomers, the sampling areas included 15 city/province regions, not including Jeju province. The 15 city/province regions were then classified into seven districts, and a sample of respondents was selected from every district. Using probability sampling with the household as the sampling unit, 4,500 households were selected. After identifying whether baby boomers resided in the household, in-person interviews were conducted. The participants of the survey were offered 10,000 Won (about US$8.7) as an incentive. Out of 4,703 collected surveys, 35 households were excluded due to missing data, resulting in a final sample of 4,668 participants in Wave 1 (2010). This original sample members were followed biannually; Wave 2 occurred in 2012 (n = 3,272; 70.2%) and Wave 3 in 2014 (n = 2,933; 62.9%). To account for participant attrition at Wave 3, the sample was refreshed with new participants (n = 1,120).
This study analyzed health behavior items from Wave 3 of the survey because two of the preventive health behaviors (i.e., herbal medicine intake and biannual physical examination) were introduced in this wave. Of the 4,053 participants in Wave 3 (including the original and refreshed participants), 6 participants were excluded from the study sample due to missing data on key variables, resulting in a final study sample of 4,047 participants.
Measures
Health behaviors
We assessed six health behaviors, including two risk-inducing and four preventive behaviors (Montano & Kasprizyk, 2015): (a) alcohol consumption, (b) smoking, (c) exercise, (d) supplement intake, (e) herbal medicine intake, and (f) physical examination.
Participants were asked how often they consume alcohol: 0 = never, 1 = less than once a month to 6 = almost every day (five to seven times a week), and how much they consume when they drink on average: 1 = one or two cups, 2 = half a bottle, 3 = less than a bottle, 4 = one to less than one and half bottles, 5 = one and half to less than two bottles, and 6 = more than two bottles. By multiplying the alcohol consumption frequency and the amount of alcohol consumption at one sitting, we calculated the amount of alcohol consumption per month (in Soju cups, 50 ml per cup; Soju is the most popular liquor in Korea). Smoking was measured by the question “Do you currently smoke cigarettes?” and response options were 0 (never smoked), 1 (smoked before, but not smoking currently), 2 (smoke sometimes), and 3 (smoke almost every day). We combined second and third response options into one category, which yields a dichotomous variable indicating current smoking status (1 = smoker, 0 = not a smoker).
Exercise was assessed as number of hours that participants spent on physical activity per week. For supplement intake, participants were asked about their frequency of taking any kind of supplement (e.g., vitamins, omega-3, and calcium) in the past 2 years. Response options ranged from 0 (never), 1 (once a year) to 8 (almost daily). Participants also indicated whether they took herbal medicines and whether they had received a physical examination from a healthcare provider in the past 2 years (1 = yes, 0 = no, respectively).
Predisposing factors
We included age, gender, marital status, and mastery as predisposing factors. Participants provided sociodemographic information, including age (in years), gender (1 = female, 0 = male), and marital status (1 = married, 0 = not married). We assessed mastery using two items from the environmental mastery subscale of Ryff’s (1989) psychological well-being measure. The two items included the following: (a) In general, I feel I am in charge of the situation in which I live and (b) I am quite good at managing the many responsibilities of my daily life. Responses were rated on a 4-point scale ranging from 1 (never) to 4 (often). The mean score of these items was calculated (ρ = .50; Eisinga, Grotenhuis, & Pelzer, 2013); a higher score indicates a higher sense of mastery and competence in managing an individual’s environment.
Enabling factors
We considered three characteristics (i.e., education, household income, and work status) as enabling resources. Educational attainment was coded into three categories: (a) less than a high school education, (b) high school diploma, and (c) more than a high school education. The high school diploma category was chosen as the reference category. Household income was measured in Korean currency (unit of 10,000 Won; ≈ US$8.70); given the skewed distribution, this variable was transformed into a logarithmic form for the regression analyses. Work status was coded as a dichotomous variable (1 = participating in paid work, 0 = not participating in paid work).
Need factors
Participants provided information related to their chronic diseases and depressive symptoms. Chronic diseases included 12 conditions (i.e., hypertension, stroke, heart disease, diabetes, cancer, lung disease, liver disease, stomach disease, arthritis, psychological conditions, reproductive diseases, and other diseases). Each item was coded 1 (yes) or 0 (no), and a count of these items was calculated. Participants were also asked whether they experienced any depressive symptoms for more than 2 weeks in the past 2 years. Participants who answered yes to this question, as well as those who reported currently taking medication for depression, were coded 1 (yes), and all others were coded 0 (no) for the presence of any depressive symptoms.
We measured health and illness concerns using six items adapted from the Illness Attitude Scale (Kellner, Fava, Lisansky, Perini, & Zielezny, 1986). The items included (a) worrying about health, (b) worrying about getting a serious illness in the future, (c) worrying whether pain experienced is caused by a serious illness, (d) believing that doctors have not diagnosed physical disease correctly, (e) fear of other serious illnesses, and (f) having symptoms similar to the illness when reading or hearing about certain illnesses. All items were rated on a 4-point scale from 1 (never) to 4 (often), and the mean score was calculated across six items (α = .85). A higher score indicates more frequent concerns or worries about participant’s health and illness concerns.
Analytic Strategy
The statistical analyses involved two phases. First, we conducted latent profile analysis (LPA) to identify unique profiles of health behaviors, using Mplus (version 6). LPA is a probabilistic-based mixture modeling technique, commonly used to identify a set of discrete latent classes (Tein, Coxe, & Cham, 2013). We included two indicators of health risk-inducing behaviors (i.e., alcohol consumption and smoking) and four preventive behaviors (i.e., exercise, supplement intake, herbal medicine intake, and physical examination). The optimal number of profiles was selected based on goodness-of-fit statistics, including the Akaike information criterion (AIC), Bayesian information criterion (BIC), adjusted BIC, entropy, and the Vuong–Lo–Mendell–Rubin likelihood ratio test. Analysis of variance (ANOVA) and chi-square tests were conducted to estimate the bivariate relationships between the derived profiles and participant characteristics.
Second, multinomial logistic regression analyses were performed to investigate the associations between the most-likely profile membership based on latent profile posterior distributions and participant characteristics, using STATA (version 14). These models included the predisposing, enabling, and need characteristics identified earlier.
Results
Descriptive statistics of participants’ characteristics and their health behaviors are presented in Table 1. The participants consumed about 12 cups (50 ml per cup) of alcohol per month, and about one fifth of the participants smoked cigarettes (19%). The mean hours of exercising per week were about 2.5 hours, and the participants took supplements once a week, on average. About one quarter of participants took herbal medicines (25%), and most of the participants had received a physical examination in the past 2 years (85%).
Descriptive Summary of Study Sample Characteristics and Health Behaviors (N = 4,047).
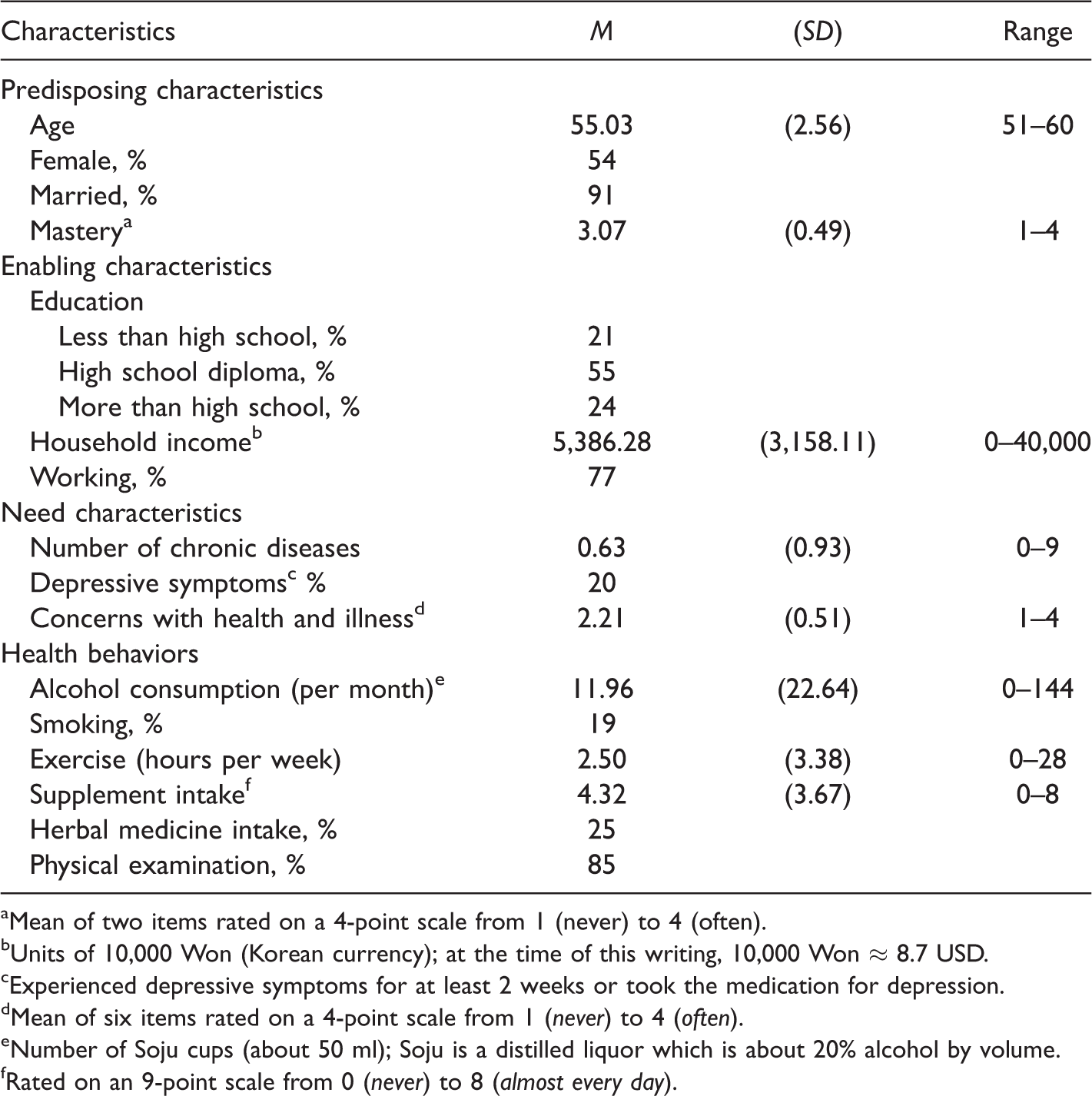
aMean of two items rated on a 4-point scale from 1 (never) to 4 (often).
bUnits of 10,000 Won (Korean currency); at the time of this writing, 10,000 Won ≈ 8.7 USD.
cExperienced depressive symptoms for at least 2 weeks or took the medication for depression.
dMean of six items rated on a 4-point scale from 1 (never) to 4 (often).
eNumber of Soju cups (about 50 ml); Soju is a distilled liquor which is about 20% alcohol by volume.
fRated on an 9-point scale from 0 (never) to 8 (almost every day).
Identification of Health Behavior Profiles
To address the first hypothesis regarding profiles of health behaviors among Korean baby boomers, we performed LPA using six indicators of health behavior. The LPA identified five profiles of health behaviors as optimal for fitting the observed data, with the smallest AIC, BIC, and adjusted BIC, and the highest entropy statistics (see Table 2).
Latent Profile Analysis and Model Fit Statistics.
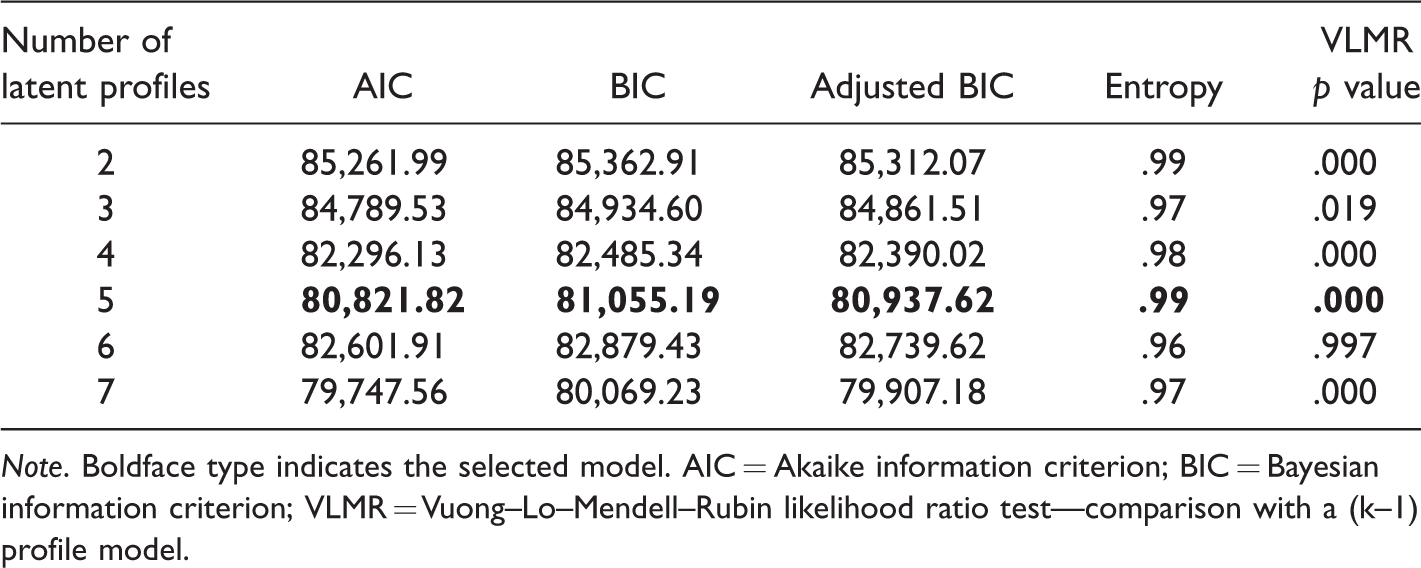
Note. Boldface type indicates the selected model. AIC = Akaike information criterion; BIC = Bayesian information criterion; VLMR = Vuong–Lo–Mendell–Rubin likelihood ratio test—comparison with a (k–1) profile model.
The health behavior profiles are described in Table 3. The five profiles of health behaviors were labeled based on the response probabilities and mean scores for risky and preventive behaviors. The low-risk and high-preventive profile (Profile 1) included 50% of the sample. This profile had the lowest probability/mean level of alcohol consumption and smoking and the highest probability/mean level of preventive behaviors (i.e., exercise, supplement intake, herbal medicine intake, and physical examination). This profile represents the most healthy pattern.
Five Latent Profiles of Health Behaviors.
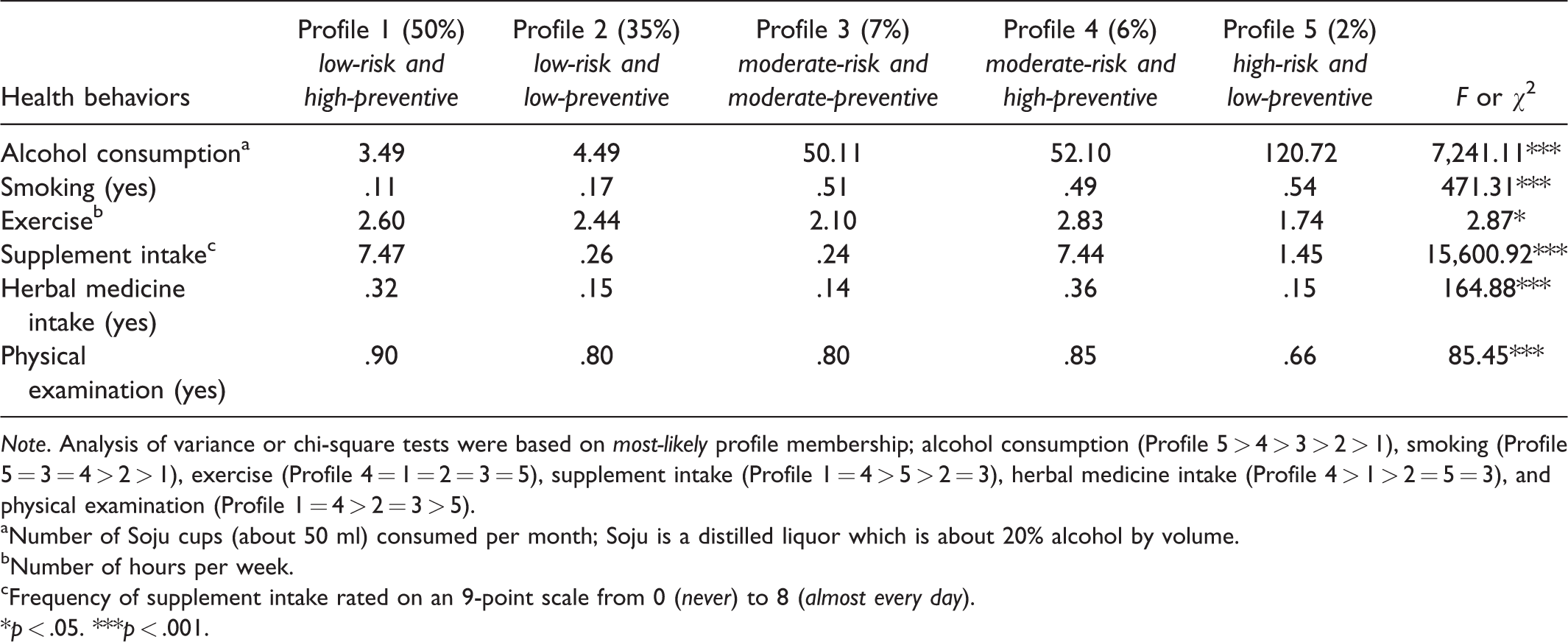
Note. Analysis of variance or chi-square tests were based on most-likely profile membership; alcohol consumption (Profile 5 > 4 > 3 > 2 > 1), smoking (Profile 5 = 3 = 4 > 2 > 1), exercise (Profile 4 = 1 = 2 = 3 = 5), supplement intake (Profile 1 = 4 > 5 > 2 = 3), herbal medicine intake (Profile 4 > 1 > 2 = 5 = 3), and physical examination (Profile 1 = 4 > 2 = 3 > 5).
aNumber of Soju cups (about 50 ml) consumed per month; Soju is a distilled liquor which is about 20% alcohol by volume.
bNumber of hours per week.
cFrequency of supplement intake rated on an 9-point scale from 0 (never) to 8 (almost every day).
*p < .05. ***p < .001.
The low-risk and low-preventive profile (Profile 2) included 35% of the participants. Participants in this profile were less likely than other participants to engage in both risky behaviors and preventive behaviors. The moderate-risk and moderate-preventive profile (Profile 3) included 7% of sample participants, and participants characterized by this profile were likely to engage in some of the preventive behaviors (i.e., exercise and physical examination) while engaging in moderate levels of alcohol consumption and smoking.
The moderate-risk and high-preventive profile (Profile 4) included 6% of the participants. This profile is characterized by engaging in a moderate level of alcohol consumption and smoking. In terms of preventive health behaviors, participants in this profile were highly engaged in preventive behaviors. The last profile, high-risk and low preventive profile (Profile 5), was the least healthy profile, where participants showed the highest levels of alcohol consumption and smoking while being less likely than other participants to engage in preventive behaviors.
Factors Associated With Health Behavior Profiles
We first examined bivariate relationships for participant characteristics and the derived health behavior profiles described earlier, using ANOVA and chi-square tests (see Table 4). The associations between predisposing factors (i.e., gender, marital status, and mastery—but not age) and health behavior profiles varied by profile. Enabling resources, including education, household income, and work status, were significantly different across profiles, as well. For need factors, self-report of depressive symptoms and perceived health (i.e., health concerns) showed significant differences across profiles, while the coefficient for number of chronic diseases was not statistically significant.
Participant Characteristic Differences by Health Behavior Profiles.
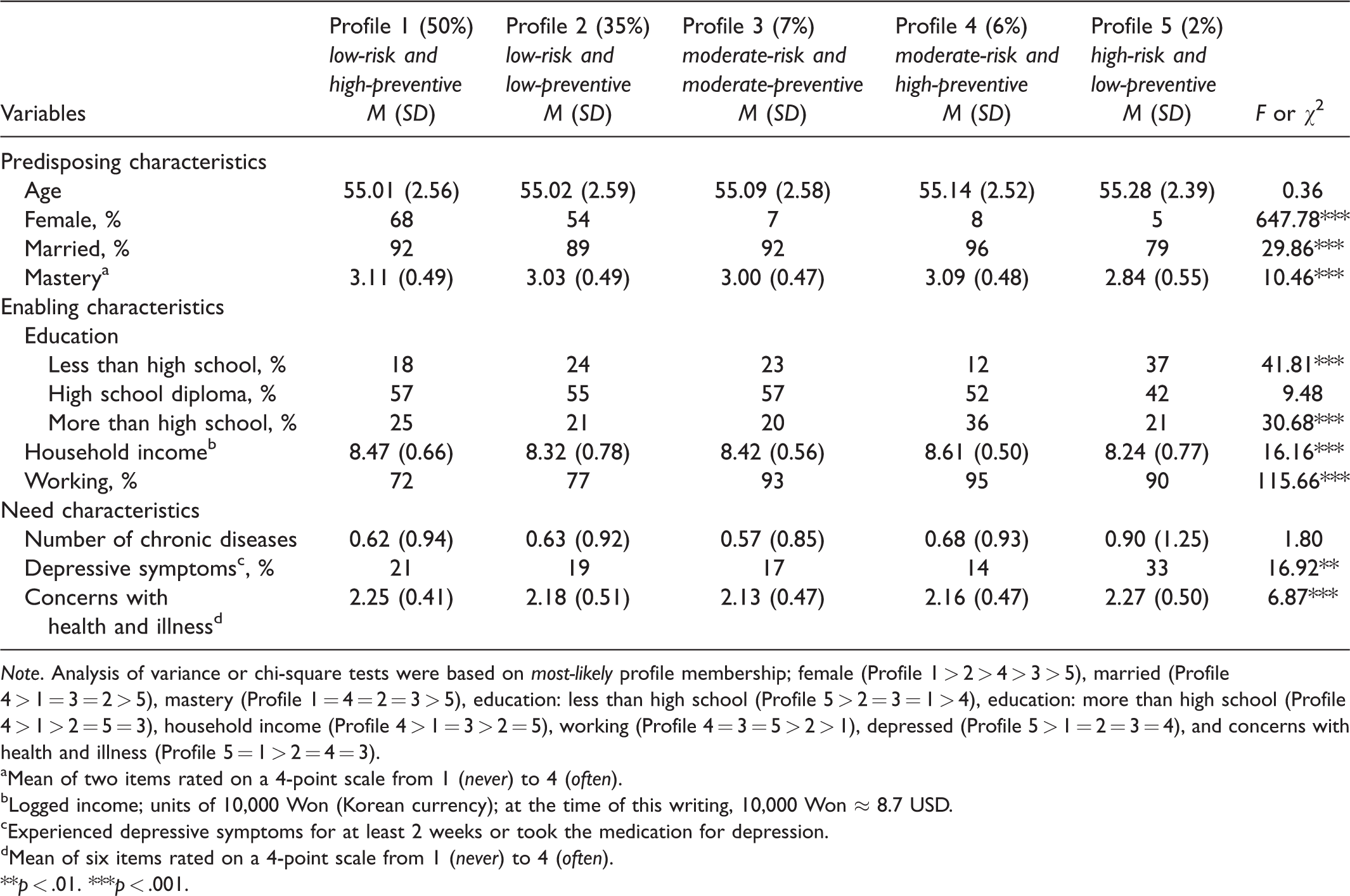
Note. Analysis of variance or chi-square tests were based on most-likely profile membership; female (Profile 1 > 2 > 4 > 3 > 5), married (Profile 4 > 1 = 3 = 2 > 5), mastery (Profile 1 = 4 = 2 = 3 > 5), education: less than high school (Profile 5 > 2 = 3 = 1 > 4), education: more than high school (Profile 4 > 1 > 2 = 5 = 3), household income (Profile 4 > 1 = 3 > 2 = 5), working (Profile 4 = 3 = 5 > 2 > 1), depressed (Profile 5 > 1 = 2 = 3 = 4), and concerns with health and illness (Profile 5 = 1 > 2 = 4 = 3).
aMean of two items rated on a 4-point scale from 1 (never) to 4 (often).
bLogged income; units of 10,000 Won (Korean currency); at the time of this writing, 10,000 Won ≈ 8.7 USD.
cExperienced depressive symptoms for at least 2 weeks or took the medication for depression.
dMean of six items rated on a 4-point scale from 1 (never) to 4 (often).
**p < .01. ***p < .001.
To address the second set of hypotheses (Hypotheses 2a, 2b, and 2c) regarding the association between individual characteristics and health behavior profiles, we performed multinomial logistic regression analyses. Table 5 shows the multinomial logistic regression results, where the low-risk and high-preventive profile (i.e., the healthiest) is the reference group. We repeated this analysis using each of the derived profiles as the reference group to examine all possible profile comparisons.
Multinomial Logistic Regression Models for Health Behavior Profiles Among Korean Baby Boomers (Relative Risk Ratios).

Note. Reference profile = Profile 1 (low-risk and high-preventive). Likelihood ratio chi-square = 985.30.
aMean of two items rated on a 4-point scale from 1 (never) to 4 (often).
bOmitted category = high school diploma.
cLogged income; units of 10,000 Won (Korean currency); at the time of this writing, 10,000 Won ≈ 8.7 USD.
dExperienced depressive symptoms for at least 2 weeks or took the medication for depression.
eMean of six items rated on a 4-point scale from 1 (never) to 4 (often).
*p < .05. **p < .01. ***p < .001.
Predisposing factors
Compared with the low-risk and high-preventive profile, older participants, women, and those who were married were less likely to belong to one of the other four profiles, with the lowest likelihood of belonging to the high-risk and low-preventive profile. Similarly, participants who reported higher levels of mastery were less likely to belong to the more unhealthy behavior profiles (Profiles 2, 3, and 5), with the lowest likelihood of belonging to the high-risk and low-preventive profile.
Enabling factors
Participants with higher education and household income were more likely to belong to healthier behavior profiles (Profiles 1 and 4), which is consistent with our hypothesis. On the other hand, workers were more likely to belong to the moderate-risk and high-preventive profile.
Need factors
As shown in the bivariate analyses, the number of chronic illnesses was not associated with profile membership. Those who experienced depressive symptoms were more likely to belong to the high-risk and low-preventive profile, compared with the moderate-risk and high-preventive profile (see Supplementary Table 1 for this comparison). Participants with a higher level of health concerns were less likely to belong to the low-risk and low-preventive profile and the moderate-risk and moderate-preventive health behavior profile.
Discussion
The first aim of this study was to identify profiles of health behaviors among Korean baby boomers. Examining health behaviors as latent profiles allowed us to identify unobservable subtypes, capturing an array of health behaviors (McAloney et al., 2013). Indeed, the LPA results showed that six behaviors could efficiently be grouped into five distinct profiles with varying combinations of risky and preventive health behaviors. The most prevalent profile for this sample of Korean baby boomers was the low-risk and high-preventive profile, which indicated that they engaged in lower levels of risky health behaviors and higher levels of preventive health behaviors. This is in line with other studies that reported Korean middle-aged adults tend to engage in more positive health-related behaviors (e.g., herbal medicine intake, massage, and acupuncture) compared with other Korean age groups (Han & Lee, 2012). The next most prevalent group was the low-risk and low-preventive profile, in which participants were less likely to be engaged in risky and preventive health behaviors. Although not engaging in risky health behaviors, such as smoking and alcohol consumption, is healthful, there is also a need to raise the awareness about the benefits of engaging in preventive health behaviors because midlife is an important time for preparing for later life (Lachman & Agrigoroaei, 2010).
Two profiles, moderate-risk and moderate-preventive and moderate-risk and high-preventive profiles may be considered as representing compensating health behavior patterns, where participants demonstrated moderate levels of risky health behaviors, while at the same time engaging in moderate to high levels of preventive behaviors. Engaging in preventive health behaviors may be a way to offset the negative consequences of participating in risky health behaviors (Ernsting et al., 2013; Radtke et al., 2011). Although we are unable to test this compensatory hypothesis with these data, researchers with appropriate data should examine whether such behaviors have consequences for health outcomes. The last profile, high risk and low preventive included only a small portion of participants (2%), but participants in this group reveal the least healthy pattern of behaviors. Participants in this profile consumed more than double the amount of alcohol (i.e., about 56 cups for men and 40 cups for women per month) recommended by the Korea Centers for Disease Control and Prevention (2018) and also showed the highest probability of smoking.
These five profiles of health behaviors showed different levels of risk-inducing or preventive health behaviors. First, the level of alcohol consumption varied greatly across profiles, ranging from 3.5 cups to 120 cups per month. The probability of smoking also significantly differed across profiles (.11 to .54). Relatively speaking, engaging in exercise was similar across profiles; participants engaged in physical activity on average about 2 to 3 hours per week, which corresponds to the recommended hours of physical activity (2.5 hours; World Health Organization, 2010). On the other hand, most participants took supplements either daily (Profiles 1 and 4) or never (Profiles 2, 3, and 5). Because physical examinations are covered by the national health insurance program in Korea (National Health Insurance Service, 2013), the probability of participating in physical examination was generally high among all profiles with exception of the last profile.
Next, we examined the association between health behavior profiles and a set of participant characteristics (i.e., predisposing, enabling, and need factors), as put forth in the behavioral models of health behaviors and healthcare services use (Andersen, 1995; Andersen et al., 2013). Aligned with our hypotheses and consistent with results from the extant scientific literature examining other populations, predisposing factors (i.e., older, women, married, and higher mastery) were strongly associated with healthier patterns of health behavior (Lachman et al., 2011; Olson et al., 2017). With respect to mastery, higher levels may act as a motivator to initiate or maintain positive behavioral changes among Korean baby boomers as the Western scientific literature suggests (Bandura, 1997; Lachman et al., 2011).
Higher socioeconomic status (i.e., education and income), categorized as an enabling factor, was associated with belonging to healthier behavior profiles. Higher socioeconomic status is linked to more resources for engaging in preventive behaviors and for having access to more information about health behaviors, which enable participants to engage in healthier behaviors. Interestingly, however, participants who were currently working were less likely to belong to the healthier health profiles. Participants may have been working to compensate for their lack of resources, which may lead to lower engagement of preventive health behaviors. Also, another contributing factor may be after-work social gatherings that often involve heavy alcohol consumption and is a social norm in the Korean culture (Park & Lee, 2011).
Need factors were associated with belonging to the healthier profile, as well. Participants with higher need, such those with higher health concerns, were more likely to engage in healthier patterns. Findings regarding health concerns indicated that being attentive to one’s own health may serve as a motivator among Korean baby boomers to engage in fewer risky behaviors and more preventive health behaviors. Our findings about participants’ health concerns did not support previous research (Skidmore et al., 2014) that suggested health concerns are linked to more risky health behaviors. This discrepancy may be due to differences in sample characteristics; our sample is a general sample of Korean middle-aged adults who may have had fewer health issues, while previous research was mostly based on clinical samples (Anttila et al., 2006; Skidmore et al., 2014).
Despite the novelty of the study population and the large sample size, along with the development of distinct, latent health behavior profiles, this study had limitations. First, the study was based on a cross-sectional research design. Although our analyses provided evidence for associations between individual characteristics and health behavior profiles, the direction of the causal relationships cannot be determined with this type of research design. Second, some of health behaviors were coded as dichotomous variables. Readers should interpret the results cautiously, as dichotomous variables may not fully capture the complexity (e.g., volume, intensity) of certain behaviors. Finally, measures of risky and preventive behaviors are based on self-report, and this may lead to responses influenced by social desirability and recall bias.
This study contributed to the field by identifying specific latent profiles of health behaviors based on observed self-report data about risky and preventive health behaviors. Previous literature has examined the association between health behavior profiles and health outcomes, but few studies investigated individual predisposing, enabling, and need characteristics associated with these profiles (Reedy, Haines, & Campbell, 2005). Co-occurrence of health behaviors varies across population subgroups (Olson et al., 2017), and the associated factors need to be explored in greater depth. Work status and health concerns, for example, may have different meanings in other cultures.
In sum, Korean baby boomers engaged in distinct patterns of health behaviors that were related to a set of individual characteristics, including predisposing, enabling, and need factors. Considering multiple preventive and risk behaviors that yield distinct health behavior profiles allows researchers, program developers, and policy makers to identify gaps and barriers among the current Korean middle-aged population, with the possibility of targeting program participation for those with higher risk and those with less preventive health profiles. For example, education programs for behavioral change should also make an effort to increase sense of mastery, which could be more effective in not only initiating a positive change but also maintaining the change. Policy interventions targeting Korean middle-aged adults who are working may contribute to healthier lives for Korean baby boomers as they move into the later stages of the life course. In addition, given the association between health concerns and health behavior profiles, future intervention strategies should work to increase awareness of the value of engaging in healthy lifestyles.
Supplemental Material
Supplemental material for Health Behavior Profiles of Korean Baby Boomers
Supplemental Material for Health Behavior Profiles of Korean Baby Boomers by Bon Kim, Kyungmin Kim, Jeffrey A. Burr and Gyounghae Han in The International Journal of Aging and Human Development
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grant, Korean Baby Boomer Panel Study (Gyounghae Han, principal investigator) from the Institute on Aging at the Seoul National University and MetLife Korea Foundation.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.