
Abstract
The study examined gender differences in the impact of living alone and intergenerational support on depressive symptoms among Mexican American older adults. The sample included 335 parent–adult child pairs which are nested within 92 Mexican American respondents, because each respondent reported their specific relationships with each child. Clustered regression analysis showed gender differences in the impact of living alone and intergenerational support on depressive symptoms among Mexican American older adults. In general, older men provided and received less intergenerational support than older women, but their depressive symptoms were more susceptible to living alone and different types of intergenerational support. Factors such as living alone, receiving instrumental support were associated with more depressive symptoms in older men than inolder women, whereas older men benefited more from the emotional closeness with children than older women. The findings highlight the need for a gender-specific approach to future research on this topic.
The number of Mexican American older adults aged 65 years and older is growing rapidly because of the high immigration volume from Mexico, persistent high fertility rates, low mortality rates, and the natural aging process (Angel & Angel, 1998; Federal Interagency Forum on Aging-Related Statistics, 2012; Pew Hispanic Center, 2016). Many older Mexican immigrants face mental health challenges, of which, depressive symptoms are the most common one (Black & Markides, 1999; Salinas, Gonzalez, & Al Snih, 2018). The Hispanic Established Population for the Epidemiologic Study of the Elderly reported that the prevalence of depression (16 or more Center for Epidemiologic Studies-Depression score) was 21.2% among older Mexican Americans (Salinas et al., 2018). Elevated levels of depressive symptoms concomitant with chronic conditions such as diabetes, heart disease, hypertension, cancer, and stroke increase the risk of mortality and disability among Mexican American older adults (Black & Markides, 1999; Salinas et al., 2018). However, the impact of living alone and intergenerational support on the depressive symptoms in older Mexican Americans has not been sufficiently studied.
Because of strong familism and economic disadvantages, older parents in Mexican American families tend to live with and depend on their children for various forms of support (Angel, Angel, McClellan, & Markides, 1996; Glick, 1999; Griffith, 1984; Himes, Hogan, & Eggebeen, 1996; Keefe, Padilla, & Carlos, 1979; Radina, 2007). But the gaps in acculturation levels between two successive generations in immigrant Mexican families and the erosion of familism over time may challenge their traditional living arrangements and family support systems (Bacallao & Smokowski, 2007; Silverstein & Chen, 1999). In addition, research shows that older men and women may experience different mental health outcomes in the face of similar risk factors such as living alone, being unmarried, and lower socioeconomic status, because of their different biological risks, socialization experiences, and social roles (Hill, Uchino, Eckhardt, & Angel, 2016; Jeon, Jang, Rhee, Kawachi, & Cho, 2007; Li, Song, & Feldman, 2009). Therefore, we expect that the impact of living alone and social support on depressive symptoms to be different among older Mexican American women and men. This study could provide important empirical evidence and policy guidance for interventions to improve older Mexican American’s mental health based on their unique cultures and interactions with adult children.
Background: Familism and Gender Roles in Mexican American Families
Family support is a relatively important source of social support to Mexican American older adults due to the strong familism (Chiriboga, Black, Aranda, & Mrkides, 2002; Hill et al., 2016; Peek, Howrey, Ternent, Ray, & Ottenbacher, 2012; Rothman, Gant, & Hnat, 1985). Previous studies suggest that children play a vital role in the health and well-being in older Mexican Americans (Angel, Douglas, & Angel, 2003; Griffith, 1984; Johnson, Schwiebert, Alvarado-Rosenmann, Pecka, & Shirk, 1997; Keefe et al., 1979; Markides & Krause, 1985; Radina, 2007). Historically, Mexican American families maintained a traditional culture described as patriarchal and authoritarian (Hill et al., 2016; Radina, 2007). Strong familism and interdependence embedded in patriarchy may translate into gendered social roles among Mexican American families. For example, men are expected to bear the responsibility for their families’ material well-being, whereas women are expected to be family and child-care providers (Radina, 2007). It is also expected that Mexican American older women have greater cohesive informal networks and social ties than older men (Angel et al., 2003; Hill et al., 2016).
Gender Differences in Living Alone and Depressive Symptoms
Mexican American older adults show preference to coreside with their children due to their cultural endorsement for closer family ties and a heavier dependence on children for support (Angel et al., 1996; Himes et al., 1996; Johnson et al., 1997). However, their preference for living with family may not always be possible. Several factors, such as intergenerational differences in lifestyle and the feeling of being a burden to their family members, may motivate older Mexican Americans toward self-reliance (Johnson et al., 1997).
Older men who are unmarried, including those who are separated, widowed, divorced, or single, are more likely to live on their own rather than with their children because men are socialized to be independent (Hill et al., 2016; Klinenberg, 2012; Varley & Blasco, 2003). Another possible reason for this trend is that older men are less likely to be taken in by their adult children and relatives, because the family provider role over the life course makes men have less interactions with children. In comparison to their female counterparts, older men are more likely to be estranged from adult children and other relatives (Klinenberg, 2012; Varley & Blasco, 2000). Moreover, men are more likely to be viewed as less resourceful because of their loss of the breadwinning role and less experiences in performing household chores (Varley & Blasco, 2000).
Some studies have demonstrated that the influences of living alone on depressive symptoms are stronger in older men than older women in Korean families and Hispanic American families (Jeon et al., 2007; Russell & Taylor, 2009). It is important to examine the association between living alone and depressive symptoms in subgroup of Hispanics (e.g., Mexican Americans) because of the heterogeneity within the Hispanic population (Losada et al., 2006).
The following factors have been proposed to account for the varying influence that living alone has on depressive symptoms for older men and older women. First, women are more likely to be the expected caregivers to their husbands and families, and therefore relative to women, older men are more emotionally dependent on their spouses. This, in turn, results in older men’s higher risks of mental health problems when they are living alone (Jeon et al., 2007). Second, although older adults who live alone generally are more likely to be socially isolated because of estrangement from their social networks (Klinenberg, 2001), older women who live alone maintain more active social ties and a greater engagement in social activities than older men (James, Wilson, Barnes, & Bennett, 2011; Park, Jang, Lee, Haley, & Chiriboga, 2013; Russell & Taylor, 2009). Thus, we hypothesize that: Hypothesis 1 (H1): Living alone has a different impact on depressive symptoms among older Mexican American males and females, with males more averse to living alone.
Gender Differences in Intergenerational Support and Depressive Symptoms
Social support is widely acknowledged as an important contributing factor that helps to decrease depression, because social support could respond to stressful situations and change individuals’ interpretations of the situations and emotional reactions (Major, Zubek, Cooper, Cozzarelli, & Richards, 1997; Pearlin, 1989). Intergenerational support, the major source of social support for older Mexican Americans, is a multidimensional concept that typically includes financial, instrumental, and emotional assistance, which are being influenced by the theory of intergenerational solidarity (Cong & Silverstein, 2011; Silverstein, Gans, & Yang, 2006; Wolff & Agree, 2004). The psychological impact of different dimensions of support could vary according to contexts (Cong & Silverstein, 2008a).
It has been well recorded that Mexican American culture endorses strong familism and exchanges of support (Peek et al., 2012; Sarkisian, Gerena, & Gerstel, 2006, 2007). Previous research showed that there are gender differences in the association between the sources of social support (e.g., whether it is from the marital or partner relationship) and depressive symptoms among adult Mexican Americans (Aranda, Castenada, Lee, & Sobel, 2001). Yet, relative few studies have examined gender differences in the association between intergenerational support and depressive symptoms in the older Mexican American population.
It is suggested that women and men have different behavioral responses to stress because of oxytocin, estrogen, and endogenous opioid mechanisms (Taylor et al., 2000). That is, the female response to stress is more marked by a pattern called “tend-and-befriend” due to natural selection and different parental investment. “Tending involves nurturant activities designed to protect the self and offspring that promote and reduce distress, befriending is the creation and maintenance of social networks that may aid in this process” (Taylor et al., 2000, p. 411). Older women tend to the needs of other people within her network, including family members and friends, and maintain the strengths of webs and support to manage the stressors (Shearer & Fleury, 2006). The pattern of “tend-and-befriend” might be maintained not only through sex-linked endocrine stress responses but also by social roles (Zunzunegui, Alvarado, Del Ser, & Otero, 2003). Girls are typically socialized to be more expressive and interpersonal, whereas boys are typically socialized to be more stoic and independent. Consequently, females could provide and receive more social support than males in adulthood (Hill et al., 2016; Li et al., 2009; Shumaker & Hill, 1991; Shye, Mullooly, Freeborn, & Pope, 1995). Studies have suggested that there are significant gender differences in the association between social support and well-being (e.g., mortality and subjective health) among the older population because of gender difference in socialization and social roles (Hill et al., 2016; Okamoto & Tanaka, 2004).
Given the gender differences in socialization, social roles in Mexican American families (Hill et al., 2016; Pei & Cong, 2016), intergenerational support may have different effects on depressive symptoms among Mexican American men and women. The “tend-and-befriend” pattern might be maintained through Mexican American older women’s social roles. Women are the traditional kin-keepers and caregivers in families (Li et al., 2009). They may protect their children and themselves by exchanging resources with their children for stress reduction. Since women are more highly embedded in social relationships and are more likely to provide and receive social support than men throughout their lifetime, women may be more likely to take both the provided and received social support for granted. Thus, women may only be influenced by higher levels of social support, and consequently, social support might have neither beneficial nor adverse effects on depression (Durden, Hill, & Angel, 2007; Shumaker & Hill, 1991; Shye et al., 1995). For example, Hill et al. (2016) found that the trajectories of perceived social support are not related to the mortality risk of older Mexican American women. Thus, intergenerational support may not be associated with depressive symptoms among older Mexican American women.
In contrast, Machismo emphasizes the family provider role of men (Radina, 2007). To be a good man should be a good provider (Villereal & Cavazos 2005). For Mexican American men, most of whom with low socioeconomic status, it has been difficult to live up to this role and thus have trouble with the provider role due to structural reasons (Villegas, de Oca Zavala, & Guillén, 2014). Their “deposit’ into a support bank manipulated by reciprocity across the life course—the bases on which adult children may motivate to provide upstream support—might be therefore too low. In urban Mexico, older men admitted that their “moral authority” often relies on their being providers (Varley & Blasco, 2000). Receiving financial support from children, even to meet necessary needs, may contradict Mexican American men’s role as traditional family providers in families (Radina, 2007). Thus, we hypothesize: Hypothesis 2 (H2): Receiving financial support from adult children has different impact on depressive symptoms among older Mexican American males and females, with males more averse to financial support from children. Hypothesis 3 (H3): Providing financial support to children has different impact on depressive symptoms among older Mexican American males and females, with males less averse to financial support to children. Hypothesis 4 (H4): Receiving instrumental support from adult children has different impact on depressive symptoms among older Mexican American males and females, with males more averse to instrumental support from children. Hypothesis 5 (H5): Providing instrumental support to adult children has different impact on depressive symptoms among older Mexican American males and females, with males more averse to instrumental support to children. Hypothesis 6 (H6): Emotional closeness with adult children has different impact on depressive symptoms among older Mexican American males and among females, with males benefiting more from emotional closeness with children.
Methods
Data
Sample
The sample for this investigation was derived from a city in West Texas, whose overall population is 285, 760, of which 32.9% are Hispanic or Latino, and 11.4% of the residents are aged 65 years and above (U.S. Census Bureau, 2012). Data were collected from a sample of adults aged 55 years and older who self-identified as Mexican American with at least one living child. Using convenience sampling, in 2010, we recruited elders in two senior centers that served predominantly Mexican American elders, as well as from community events that are popular among Mexican Americans. The survey included 99 older parents who reported information and their interactions with 394 adult children. After deleting missing values, the resulting analytic file constituted 335 observations which were nested within 92 older parents.
Measures
Dependent variable
The dependent variable was the severity of depressive symptoms of older adults. The measure was adapted from the CES-D scale (Radloff, 1977). The 20 items include negative mood, positive mood, somatic symptoms, and feelings of interpersonal conditions. We coded the frequency with which the respondent had experienced each symptom during the past week as 0 (rarely or none of the time or less than 1 day), 1 (some or a little of the time or 1–2 days), 2 (occasionally of a moderate amount of time or 3 to 4 days), or 3 (most or all of the time or 5 to 7 days). Summing all items of this scale yields one score of depression ranging from 0 to 60. A higher score indicated more depressive symptoms after reverse coding four positive feeling items. The CES-D had adequate validity as well as reliability in a number of previous studies with older populations including Hispanic (Aguilar-Gaxiola & Gullotta, 2008; Roberts, 1980). The Cronbach’s alpha of this measure was .82 in this study.
Independent variables
Our key independent variables were older parents’ gender, living arrangements, and intergenerational support, including financial support, instrumental support, and parent–child emotional closeness. Gender of older parents was coded as 0 (male) and 1 (female). Living alone and marital status are usually intertwined because those married usually live with spouses. To disentangle the effect of marital status and living arrangements, we categorized respondents into three categories, namely unmarried and living with others (reference), married and living with others (as 1), and unmarried and living alone (as 2). The group who were unmarried and living with others were used as a reference so that its comparisons with other two groups reflected the effect of being married when living with others and that of living alone when unmarried.
Financial support was the total amount of money and in-kind gifts that elders received from, or provided, to each child during the previous 12 months. If the exact amount was not available, respondents were asked to choose among the following nine categories: (0 = none, 1 = less than 100, 2 = 100 to 199, 3 = 200 to 499, 4 = 500 to 999, 5 = 1000 to 2999, 6 = 3000 to 4999, 7 = 5000 to 9999, and 8 = more than 10000 of US dollars). Then the median value of the chosen category was used to interpolate the amount of financial support. Because high percentages of receiving no financial support from children or providing no financial support to children, we used 0 (no financial support) and 1 (some financial support) to present financial support from or to children.
Instrumental support was based on household chores or personal care received from and provided to any children or children’s family (including children-in-law) during the last year. Instrumental support received was coded as 0 = didn't receive instrumental support from any children and 1 = received some instrumental support from any children. Similarly, instrument support provided was coded as 0 = didn't provide any instrumental support to any children and 1 = provided instrumental support to any children.
Emotional closeness between a respondent and each child was measured with six questions adapted from the Affectual Solidarity inventory (Mangen, 1988): (a) Taking everything into consideration, how close do you feel to this child? (b) Overall, how well do you and (this child) get along together? (c) How is the communication between you and this child, exchanging ideas and talking about things that really concern you at this point in life? (d) How well do you feel that you understand this child? (e) How well do you feel that this child understand you? (f) How much do you feel that this child would be willing to listen when you need to talk about your worries and problems? The answers were coded as: 0 (not all close, not at all well, not at all good, or not at all willing), 1 (not too close or not too good), 2 (somewhat close, somewhat well, somewhat good, or somewhat willing), 3 (very close, very well, very good, or very willing), or 4 (extremely close, extremely well, extremely good, or extremely willing). Summing all items of this scale yields one score of emotional closeness ranging from 0 to 24. The reliability coefficient of this measure was .90.
Control variables
We controlled for characteristics of older parents and their children as well. Older parents’ characteristics included factors known to be related to depressive symptoms (AlegrÃa et al., 2008; Chiriboga, Black, Aranda, & Markides, 2002; Cong & Silverstein, 2008b; Rote, Chen, & Markides, 2015; Schulz et al., 2006). Age was measured in chronological years. Years of education were coded by continuous variables (0–17). Immigrant status was determined by asking the respondents which country he or she was born and was coded as 0 (born in USA) and 1 (born in Mexico). Functional limitations were measured as the sum of seven items (α = .83) reflecting difficulties in performing daily living activities (0 = no difficulty, 1 = some difficulty, 2 = cannot do at all) from a modified version of the Katz ADL scale (Al Snih et al., 2009), including walking, bathing, grooming, dressing, eating, removing continence, and toileting. Because older adult’s functional limitations were nonnormallly distributed with high percentages having no functional limitations, we used dummy coding to present the functional limitations of older parents as 0 = have no functional limitation and 1 = have some functional limitations. Respondents’ finance strain was based on the question: How much difficulties do you have in meeting monthly payments on your bills, and the variable was coded as 0 = none and 1 = some. The number of children was measured as the number of living children. Parent–child geographic proximity was dummy coded as 0 = not living in the same city and 1 = living in the same city. The level of acculturation was assessed by the 12 items of the Brief Acculturation Rating Scale for Mexican American-II (Cuellar, Arnold, & Maldonado, 1995). It includes the Mexican Orientation Subscale (MOS, e.g., “I enjoy speaking Spanish,” “I enjoy reading books in Spanish,” α = .69) and Anglo Orientation Subscale (AOS, e.g., “My thinking is done in English language,” “My friends are of Anglo origin,” α = .80). Older respondents were asked to rate these statements on a 5-point Likert scale ranging from 0 (not at all) to 4 (almost always or extremely often). Acculturation scores were calculated as the difference between the mean of AOS and that of mean MOS (AOS-MOS): 0 (>−1.33, very Mexican oriented), 1 (≥−1.33 and ≤−0.07, Mexican oriented or balanced bicultural), 2 (>−0.07 and <1.19, slightly Anglo oriented bicultural), 3 (≥1.19 and <2.45, very Anglo oriented bicultural), and 4 (>2.45, assimilated or Anglicized), with higher scores representing more acculturated. Finally, because the level of acculturation was nonnormally distributed, we used dummy coding to present the level of acculturation (0 = low level of acculturation and 1 = high level of acculturation (Pei & Cong, 2016). Children’s characteristic included age in years, gender (0 = son, 1 = daughter), years of education achieved (0–17), marital status (0 = unmarried, 1= married), and the number of their own children (0 = 0–2 children, 1 = more than 2 children).
Analytic Strategy
We used multiple regression analysis to estimate the impact of parents’ living alone and intergenerational support on depressive symptoms among older Mexican Americans. Because the 335 parent–child dyads were nested within 92 families, we generated robust standard errors to account for the family clustering (Cong & Silverstein, 2008b; Silverstein et al., 2006; Statacorp, 2001). We did the analysis for males and for females separately, and then for all respondents combined. For the all-parent sample, we included two-way interactions between parents’ gender, parents’ living arrangement, and intergenerational support to examine if there are greater associations with depressive symptoms in older men than in older women. To compensate for the low power related to multiplicative variables (i.e., higher than desired Type II error), we used p < .10 to identify statistically significant effects for interactions (Cong & Silverstein, 2008a).
Results
As shown in Table 1, the average depressive symptoms were 7.83 (SD = 8.32) for males and 9.88 (SD = 7.20) for females. T tests showed no significant differences between males and females concerning age (averaged 70 and 69 years, respectively), but males had significantly lower education levels (6.50 vs. 8.88). χ2 tests showed no significant differences between males and females concerning immigrant status (20% and 11.5% were born in Mexico, respectively), health status (45% and 28.9% have some functional limitation, respectively), the number of children (averaged 4), and financial strain (37.5% and 55.8% experienced financial strain, respectively). Whereas males and females had significant gender difference in the level of acculturation (the percentage of high level of acculturation was 40% and 61.5%, respectively).
Characteristics of Older Parents, Adult Children, and Intergenerational Support.
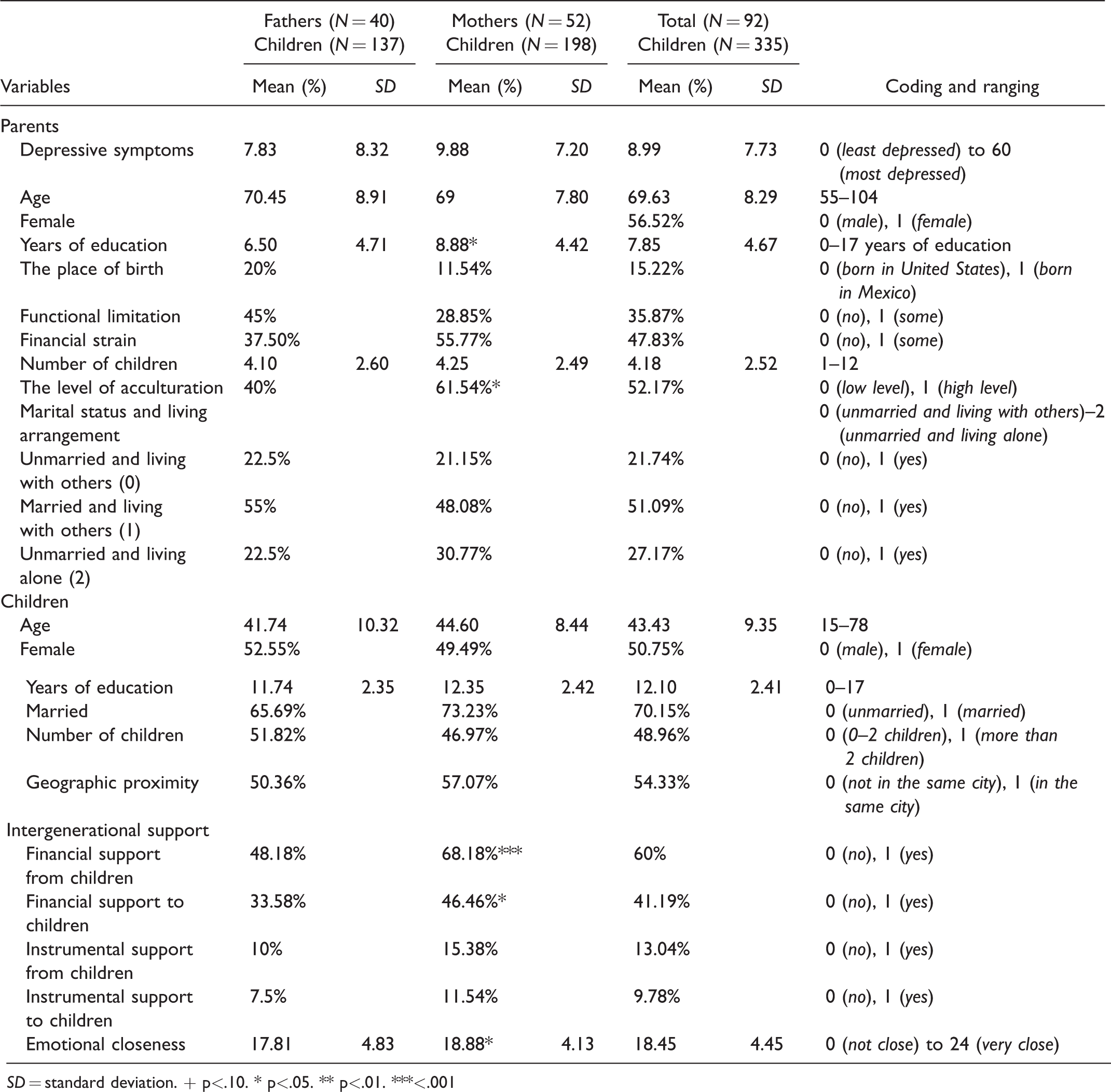
SD = standard deviation. + p<.10. * p<.05. ** p<.01. ***<.001
T tests or χ2 tests were also used to examine whether there were gender differences in parents’ depressive symptoms, living arrangement, and intergenerational support. Males and females were not significantly different from each other in respect to depressive symptoms (averaged 7.83 and 9.88, respectively) and living alone (22.5% and 30.8% were unmarried and living alone, respectively). Mothers were more likely to receive and provide financial support from or to children than fathers (48.2% vs. 68.2%, 33.6% vs. 46.5%, respectively). Mothers had significantly higher emotional closeness to their children than fathers (17.81 vs. 18.88, respectively). There were no gender difference in instrumental support received and provided between mothers and their children and between fathers and their children.
Table 2 provides results of the two models estimating depressive symptoms for males and females separately. Both in Models 1 and 2, before and after controlling for the characteristics of respondents and adult children, being unmarried and living alone, receiving and providing instrumental support increased risks for depressive symptoms, and emotional closeness with children was a protective factor for reducing depressive symptoms in fathers. Neither living arrangements nor intergenerational support were significantly associated with depressive symptoms among mothers in both Models 1 and 2.
Regression Estimates Predicting Depression With Robust Standard Errors (Separate by Gender).
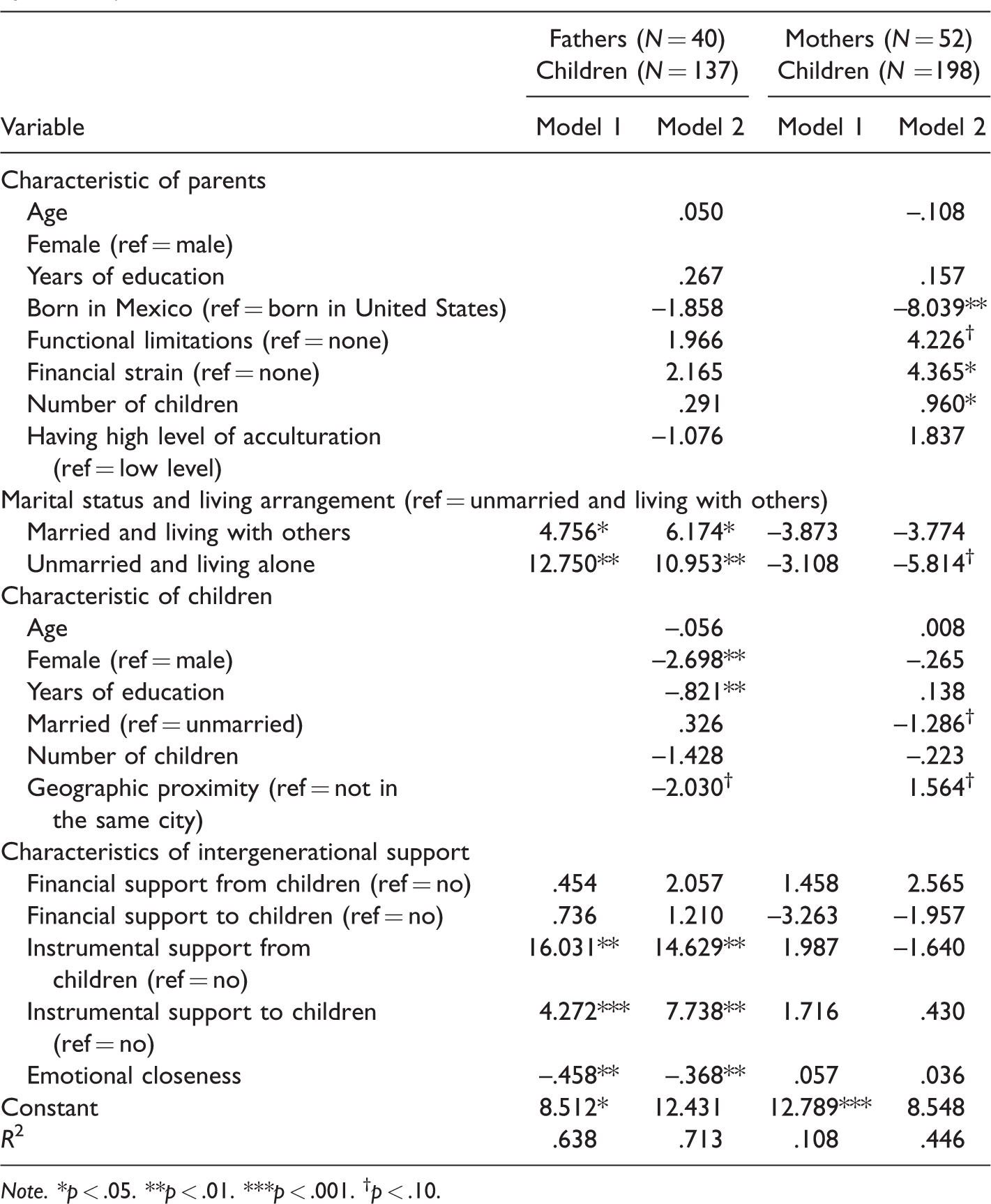
Note. *p < .05. **p < .01. ***p < .001. †p < .10.
In respect to control variables, females who were born in Mexico had less depressive symptoms than those born in United States, whereas females who had financial strain had more depressive symptoms than those who had no financial strain. The number of adult children was positively related to depressive symptoms among females. Adult children’s characteristics, including gender and education, were associated with depressive symptoms in males.
In Table 3, we did the analysis for the whole sample. In Model 1, we found a significantly negative interaction between being female and being unmarried and living alone, indicating that relative to those who were unmarried and living with others, those who were unmarried and living alone presented higher risks of depressive symptoms in males than in females. In Model 4, we found a significantly negative interaction between being female and receiving instrumental support from children, suggesting that receiving instrumental support from any child increased the risk of depression to a greater extent in males than in females. In Model 6, we found a significantly positive interaction between being female and emotional closeness, showing that emotional closeness with children decreased the risk of depression to a greater degree in males than in females.
Regression Estimates Predicting Depression With Robust Standard Errors (Total Sample N = 335). a
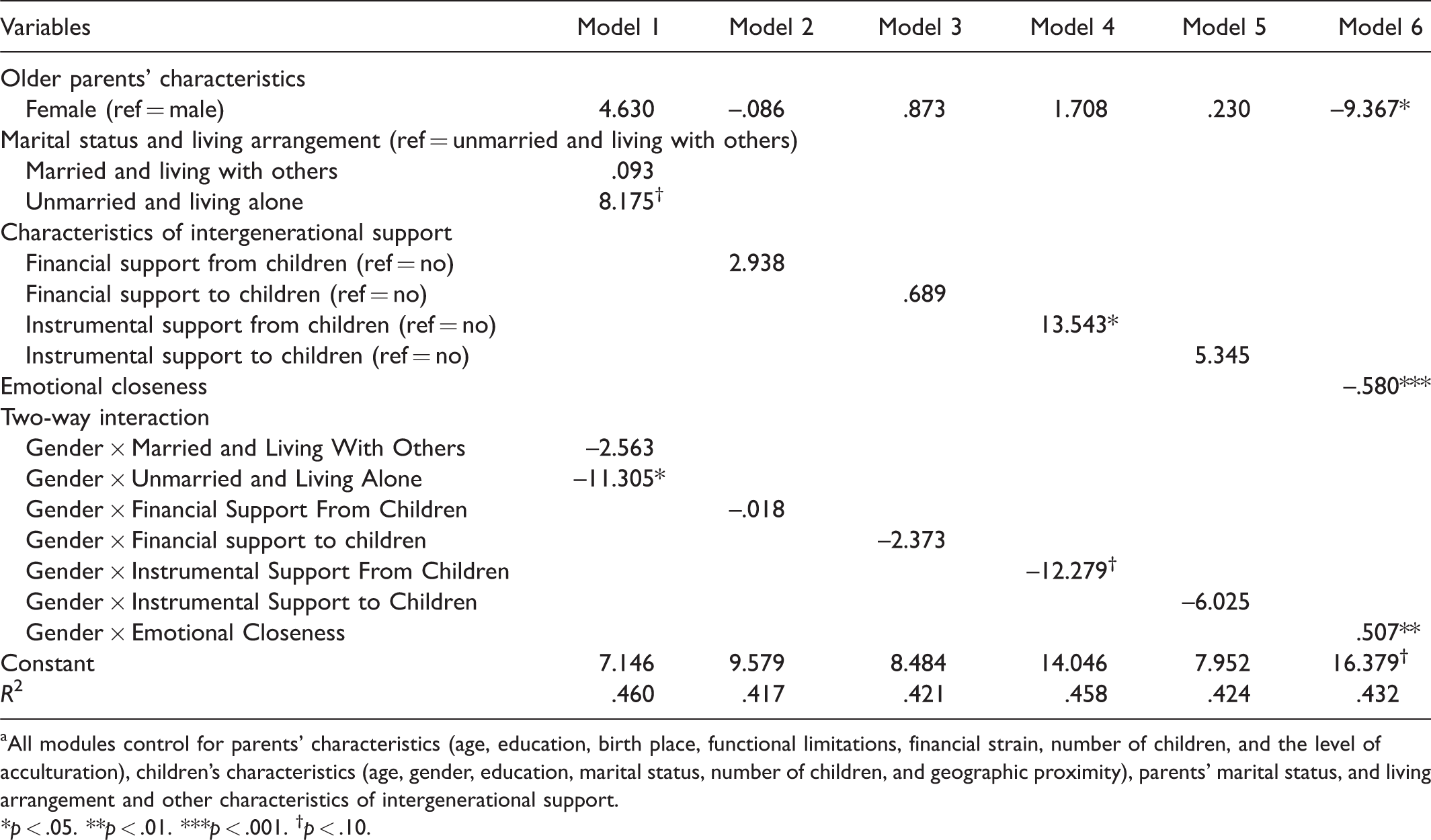
aAll modules control for parents’ characteristics (age, education, birth place, functional limitations, financial strain, number of children, and the level of acculturation), children’s characteristics (age, gender, education, marital status, number of children, and geographic proximity), parents’ marital status, and living arrangement and other characteristics of intergenerational support.
*p < .05. **p < .01. ***p < .001. †p < .10.
Discussion
This study extends previous work on gender differences in the impact of living alone and different types of intergenerational support on depressive symptoms among Mexican American older adults. The hypothesis that living alone had different impact on depressive symptoms among older Mexican American males and females, with males more averse to living alone (H1), was supported. We found that older males who were unmarried and living alone had more depressive symptoms than those who were unmarried and living with others, whereas living alone was not significantly associated with depressive symptoms among unmarried mothers. Moreover, being unmarried and living alone presented higher risks of depressive symptoms in males than in females. Our findings are consistent with previous research in Korean and Hispanic families and add new weight to the conclusion that the influences of living alone on depressive symptoms are stronger among older men than older women (Jeon et al., 2007; Russell & Taylor, 2009). This could be a result of older men’s emotional dependence on their wives due to females’ traditional caregiving role in Mexican American families (Jeon et al., 2007; Radina, 2007), and older women’s larger social networks, which protect them against the risk of social isolation (Angel et al., 2003; Hill et al., 2016). The findings highlighted the vulnerability of the older Mexican American men who are unmarried and living alone.
Our hypothesis that receiving financial support from adult children has different impact on depressive symptoms among older Mexican American males and females, with males more averse to financial support from children (H2), was not supported. We found that receiving financial support from children was not associated with depressive symptoms in both males and females, and that the interaction between receiving financial support from children and being female was not significant. Previous research on intergenerational support found that the majority of older Mexican Americans did not receive financial transfers from their adult children (Dietz, 1995; Eggebeen & Hogan, 1990). Presumably that the relatively small amount of financial support from adult children may not have a big impact on male’s role as a family provider and thus would not risk the psychological well-being of older Mexican men.
The hypothesis that providing financial support to children has different impact on depressive symptoms among older Mexican American males and females, with males less averse to financial support to children (H3), was not supported. We found that providing financial support to children was not associated with depressive symptoms in both males and females, and that the interaction between providing financial support to children and being female was not significant. Our findings were not consistent with the previous research that financial support provided to adult children is positively related to the increase of self-rated health in older men (Li et al., 2009). This may be because Mexican American older adults are not very likely to provide financial support to their children as a result of economic disadvantages (Sarkisian et al., 2006, 2007). Thus, the limited amount of financial support provided to children in Mexican American families may not have a sufficient effect size on the depressive symptoms to be detected in this sample of older Mexican American adults.
Our hypothesis that receiving instrumental support from adult children has different impact on depressive symptoms among older Mexican American males and females, with males more averse to instrumental support from children (H4), was supported. We found that older males who received instrumental support from children reported a higher level of depressive symptoms than others, but this pattern was not found among older women. Moreover, the interaction between receiving instrumental support from children and being female was significant. A similar finding that instrumental support received from children was negatively related to improved subjective health of older men was reported in a study on rural Chinese older adults, who share similar familism and gender norms (Li et al., 2009). Even in families which are characterized by familism, such as those in rural China and Mexico, it is common for older men to have a feeling of burden when received instrumental support from children or living with children (Li et al., 2009; Varley & Blasco, 2000). Our findings suggest that older Mexican American men value independence and do not want to be a burden to their children. These results highlight the role of social expectations in shaping gender difference of the association between receiving instrumental support from adult children and depressive symptoms.
The hypothesis that providing instrumental support to adult children has a different impact on depressive symptoms among Mexican American males and females, with males more averse to instrumental support to children (H5), was partially supported. We found that older fathers who provided instrumental support to children reported a higher level of depressive symptoms than others. Nevertheless, providing instrumental support to adult children was not associated with a higher level of depressive symptoms among females. To some extent, the finding is consistent with Fragoso and Kashubeck’s (2000) finding that gender role conflict was associated with higher levels of depressive symptoms among Mexican American men. Because of separation in the early migration and the loss of providing role in later life, older Mexican American men tend to have more experiences in the household (Hondagneu-Sotelo, 1992; Villereal & Cavazos, 2005). The strong gender role expectations may lag behind context changes that have increased older men’s involvement in household labor, and thus would be associated with the psychological well-being of the older males. Our findings highlight the necessity of interventions for the older Mexican American men who provided instrumental support to children.
Our hypothesis that emotional closeness with adult children has different impact on depressive symptoms among older Mexican American males and among females, with males benefiting more from the emotional closeness with children (H6), was supported. We found a beneficial impact of emotional support on reducing depressive symptoms among older men, but not in women. Moreover, Mexican American males received more psychological benefits from being close to their children than their female counterparts. Although older Mexican American men are less emotional close with their children than older women, the emotional closeness with children was negatively associated with depressive symptoms in older men. Our result is consistent with previous findings that older men are more likely to gain benefits from the perceived social support, such as emotional support, than older women with a lower threshold (Hill et al., 2016; Okamoto & Tanaka, 2004; Patrick et al., 2001). Given that emotional closeness with children was more likely to decrease levels of depressive symptoms among older males than females, it is particularly important to build quality intergenerational relationships for the elderly men among Mexican American older adults.
Although older women were more likely to provide or receive intergenerational support than older men, which is consistent with previous studies (Hill et al., 2016; Jang & Tang, 2016; Li et al., 2009), none of these intergenerational support dimensions was associated with depressive symptoms in older women. Because of their traditional kin-keeper and caregiver roles in Mexican American families, older women may protect themselves and their adult children from being stressed out through providing to and receiving from adult children. Over the life course, older women may take the frequent intergenerational exchanges for granted. Consequently, intergenerational support is less likely to be associated with the psychological well-being in older women than older men. Some scholars further pointed out that older women are more likely to be influenced by high levels of social support because of their traditional social roles (Durden et al., 2007; Shumaker & Hill, 1991; Shye et al., 1995). Thus, another possibility is that the support received by our older Mexican American females was not high enough to make a difference, because few older Mexican American females in our sample had adult children with enough resources to maintain high levels of intergenerational exchanges.
Overall, the finding regarding the gender differences in the association between intergenerational support and depressive symptoms are consistent with previous findings among older Mexican American, Japanese, and rural U.S. population that older women’ well-being (i.e., morality, subjective health, and psychological well-being) is less likely to be influenced by social support than older men (Hill et al., 2016; Okamoto & Tanaka, 2004; Patrick et al., 2001). To some extent, this gender difference may reflect a “tend-and-befriend” pattern in women’s response to stress which are proposed by Taylor et al. (2000). But our study confirmed that social role may be an important social factor that maintains the pattern of “tend-and-befriend” pattern in older women (Zunzunegui et al., 2003).
Our findings highlight the gender differences in the impact of living alone and intergenerational support on depressive symptoms in the Mexican American population. Living alone was associated with higher levels of depressive symptoms in older men, but not older women. Receiving and providing instrumental support from or to children was associated with higher levels of depressive symptoms, and emotional closeness with children was negatively associated with depressive symptoms in older men. Nevertheless, none of these intergenerational support dimensions was associated with depressive symptoms in older women. Moreover, the impact of living alone, receiving instrumental support, and the emotional closeness with children were stronger in fathers than in mothers. It is noted that when controlling for the same variables, our models explained more variance in the level of depressive symptoms among older men than older women (R2 = .713 vs. .446). Although it is also possible that other factors, not studied here, may matter more among older women, these results suggest that living alone and intergenerational support are more important for depressive symptoms in older men than older women.
The study also had some limitations that need to be addressed. First, due to older Mexican Americans’ potential fear and distrust of institutions, language barriers, schedule conflicts, and cultural differences (Areán & Gallagher-Thompson, 1996; Loue & Sajatovic, 2008), we used a geographically restricted small sample with convenience sampling strategy, which is common in social science research, especially when used with ethnic minority populations (Knight, Roosa, & Umana-Taylor, 2009). Therefore, the sampling strategy may limit the generalizability of our findings. It would be of significant interest to replicate the present analysis in a representative sample to observe how consistently and strongly the gender differences in the impact of living alone, and intergenerational support on the psychological well-being of the Mexican American older adults.
Second, the cross-sectional design of this study makes it difficult to draw conclusions regarding the directions of these relationships. Moreover, there may be over-time changes in living arrangements, intergenerational support, and depressive symptoms. Further longitudinal analyses should be conducted to establish causal relationships and explore gender differences in the links between changes in living arrangements, the amount of intergenerational support, and psychological well-being among Mexican American older adults.
Third, informational support, as an important aspect of social support was not addressed in this study. Being influenced by the theory of intergenerational solidarity, as in other studies on intergenerational support, intergenerational support in our study includes financial, instrumental, and emotional support (Cong & Silverstein, 2011; Wolff & Agree, 2004). Manifest solidarity, as an important domain of intergenerational cohesion, refers functional aspect in family life, including financial, instrumental, and emotional support (Silverstein et al., 2006). However, based on the performed functions, social support has also been divided into emotional, informational, and instrumental support (Niska, 1999; Thoits, 2011). Instrumental assistance includes offering or supplying behavioral or economic help (Thoits, 2011). Thus, informational support is not included in our study. Given the important role of informational support, future studies need to examine the impact of informational support on mental health outcomes (Thoits, 2011).
Despite those limitations, the findings of the study have implications for understanding the gender differences in the impact of living alone and intergenerational support on depressive symptoms among Mexican American older adults. The most important finding of this study is the gender differences in the impacts of living alone and intergenerational support on depressive symptoms in Mexican American older population. This suggests that the influences of living alone and intergenerational support on depressive symptoms are stronger in older men than older women, and older men are more likely to be influenced by lower levels of intergenerational support than older women. Thus, interventions should take those findings into consideration and adopt different strategies for older Mexican men and women.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the grant “Intergenerational Relations in Mexican American Families” awarded to Zhen Cong, funded by College of Human Sciences, Texas Tech University.