
Abstract
There has been a documented increase in the numbers of filial and sandwiched caregivers in the United States. However, past studies have overlooked the impact of work and family overload on caregiver well-being. This study investigates the moderating influences of the quality and directionality of work and family spillover on the well-being (e.g., positive affect and negative affect, psychological well-being, and global well-being) of 180 filial and sandwiched caregivers from the second wave of the Midlife in the United States Survey. Regression and moderation analyses revealed that sandwiched caregivers with high levels of negative work-to-family spillover exhibited higher negative affect than the comparison groups. Sandwiched caregivers with high levels of negative family-to-work spillover exhibited higher level of negative affect and lower level of self-acceptance than other caregivers. These findings can help create work programs that address spillover between work and home in the effort to promote caregiver well-being.
Keywords
Introduction
There are 34.2 million family caregivers of older adults in the United States, including nonsandwiched filial (caregiving for a parent or parent-in-law) caregivers and sandwiched (caregiving for both children and a parent or parent-in-law) filial caregivers (American Association of Retired Persons & The National Alliance for Caregiving, 2015). For simplicity, nonsandwiched filial caregivers will be referred to as filial caregivers and sandwiched filial caregivers will be referred to as sandwiched caregivers. There has been a documented growth in the number of filial and sandwiched caregivers, which has been driven by the combination of increasing life expectancy and more adults needing instrumental or financial support in late adulthood (Center for Disease Control, 2016). In addition, 74% of family caregivers in the United States worked while providing care (Feinberg & Choula, 2012). Thus, it is critical to examine how the intersection of family caregiving and work responsibilities impacts the aspects of well-being in filial and sandwiched caregivers in midlife and late adulthood. Informed by the life course perspective and stress process model (Elder, Johnson, & Crosnoe, 2003; Pearlin & Skaff, 1996), this study extends the extant research by examining the association between caregiver type (filial and sandwiched) and the aspects of psychological well-being (e.g., negative affect and self-acceptance) in a sample of filial and sandwiched caregivers in the context of work and family spillover.
Filial and Sandwiched Caregivers and Psychological Well-Being
Much of the existing literature on caregiver well-being has focused on family caregivers primarily in the context of spousal caregivers or as a group without considering the specific nature of the caregiver and care–recipient relationship (Pinquart & Sorensen, 2004; Silverstein & Giarrusso, 2010). While the literature has focused on the examination of filial caregivers’ well-being as compared with other family caregivers (e.g., spousal caregivers; Kang, 2006; Ourada & Walker, 2014), less attention has been devoted to the comparison of filial and sandwiched caregivers’ well-being.
Compared with past decades in the United States, young adults are now remaining in the family home longer, with some living in their family home into their mid-20s (Arnett, 2000). Emerging adults who are living in their family homes may still depend on their parents for some aspect of financial or instrumental support (Federal Interagency Forum on Child and Family Statistics, 2014). This social change underlies the increase in the number of sandwiched caregivers. While there has been a documented growth in the number of filial and sandwiched caregivers, few studies have compared the well-being of these two groups (Rubin & White-Means, 2009). This comparison is important to consider as filial and sandwiched caregivers may be more vulnerable to lower levels of well-being (e.g., affect and self-acceptance) than other family caregivers (e.g., sibling and other kin). Compared with filial caregivers, sandwiched caregivers have the additional responsibilities of caring for children, which may result in greater caregiving distress (DePasquale et al., 2016). Also, sandwiched caregivers were found to report lower levels of psychological well-being when compared with other family caregivers (e.g., spousal caregivers and filial caregivers; Daatland, Veenstra, & Lima, 2010; Hammer & Neal, 2008; Steiner & Fletcher, 2017). Together, the findings of Daatland et al. (2010) and Steiner and Fletcher (2017) suggest that caregiver type matters in the context of well-being.
Well-being has been shown to be comprised of multiple aspects, which may not be captured solely one domain (e.g., affect). Ryff (2014) demonstrated the importance of examining well-being by assessing multiple aspects, including personal growth, autonomy, environmental mastery, self-acceptance, purpose in life, and positive relations with others. The separate aspects of psychological well-being have been studied in the context of family caregiving. Marks, Lambert, and Choi (2002) documented that filial caregivers reported less personal mastery, personal growth, and self-acceptance when compared with other types of caregivers, including spousal caregivers and other kin caregivers. The findings of Marks et al. (2002) highlighted the need to compare groups of caregivers to identify caregivers who may be vulnerable to lower levels of well-being. Of the existing studies that have examined the components of psychological well-being across caregiver type (Marino, Haley, & Roth, 2017; Marks et al., 2002), the comparison between filial and sandwiched caregivers has been overlooked. This study furthers the field of caregiving by examining the extent to which types of caregiving, specifically filial and sandwiched caregiving, impact multiple aspects of psychological well-being (e.g., self-acceptance, purpose in life, and autonomy).
Filial and Sandwiched Caregivers and Employment
In line with the life course perspective (Elder et al., 2003), caregiving does not occur in isolation and lives often are embedded in the contexts in which they reside. Individuals providing family care may find themselves navigating additional responsibilities outside of their caregiving roles (e.g., work; Feinberg & Choula, 2012). Navigating work responsibilities in the context of caregiving burden may give rise to conflicts that may be carried over between work and family life and impact caregiver well-being (England & Tripp-Reimer, 2003; Steiner & Fletcher, 2017). Complementing the life course perspective, the stress process model provides insight into how different levels of stressors (e.g., primary and secondary) may intersect and shape caregiver well-being (Pearlin & Skaff, 1996). While work and family spillover has been studied in the context of work hours, supervisor support, and demographic differences (Bianchi & Milkie, 2010), it has been understudied as a moderator of the relationship between caregiver type and well-being. This examination is important because certain caregivers may be more vulnerable to stressors carried over from work and family responsibilities and vice versa (Bianchi & Milkie, 2010).
To assess different domains within the intersection of work and family, Grzywacz (2000) offered a multidimensional conceptualization of work and family spillover that captures quality (negative or positive) and directionality (work-to-family and family-to-work; Grzywacz, 2000). The work of Grzywacz and Marks (2000) showed that both the quality and directionality of work and family spillover shaped the well-being of individuals with family responsibilities. Of the existing literature that has examined work and family spillover, negative work and family spillover was associated with lower levels of well-being in a sample of female filial caregivers as compared with noncaregivers (Stephens, Franks, & Atienza, 1997). Similar findings on negative work and family spillover have been reported for sandwiched caregivers. Hammer and Neal (2008) found that negative and positive domains of work–family spillover were associated with different levels of well-being for sandwiched caregivers in that negative work and family spillover lowered the levels of well-being and positive work and family spillover promoted the aspects of well-being. While more attention has been paid to negative work and family spillover (Michel, Kotrba, Mitchelson, Clark, & Baltes, 2011; Stephens et al., 1997), the examination of both quality and directionality of work and family spillover has been overlooked. In line with the work of Grzywacz (2000), this study examines the moderating role of four domains of work and family spillover to capture the quality and directionality of spillover experienced by filial and sandwiched caregivers, which may shape caregiver well-being.
Study Goals
The first goal of this study is to investigate the effect of caregiver type (filial vs. sandwiched caregivers) on aspects of well-being (e.g., negative affect and positive affect, self-acceptance, purpose in life, and global well-being). Consistent with the work of Daatland et al. (2010) who found sandwiched caregivers to be more vulnerable to lower levels of well-being, it is predicted that sandwiched caregivers will exhibit higher negative affect, lower positive affect, lower levels of psychological well-being, and lower global well-being when compared with filial caregivers. In addition, this effect is expected due to the multiple social responsibilities that caregivers occupy which may influence well-being.
The second goal of this study is to examine the moderating role of work and family spillover, specifically the quality (negative and positive) and directionality (work-to-family and family-to-work), on the association between caregiver type and aspects of well-being. It is hypothesized that negative work-to-family spillover would moderate the association between caregiver type and well-being. Sandwiched caregivers with high levels of negative work-to-family spillover are expected to exhibit higher negative affect, lower positive affect, lower levels of psychological well-being, and lower global well-being when compared with filial caregivers with high levels of negative work-to-family spillover as well as filial and sandwiched caregivers with low levels of negative work-to-family spillover. This hypothesis is in line with the work of Hammer and Neal (2008) who found that high levels of negative work and family spillover negatively impacted sandwiched caregiver well-being. As for the moderating influence of negative family-to-work spillover, sandwiched caregivers with high levels of negative family-to-work spillover are expected to exhibit lower positive affect, higher negative affect, lower levels of well-being, and lower global well-being when compared with filial caregivers with high levels of negative family-to-work spillover as well as filial and sandwiched caregivers with low levels of negative family-to-work spillover. In this study, a set of covariates will be accounted for in each of the regression models (see the Method section for more details).
Past research has reported mixed findings in the examination of positive work-to-family and family-to-work spillover as a moderator of the relationship between family caregiver type and well-being (Hammer & Neal, 2008; Stephens et al., 1997). In the examination of positive work and family spillover on filial caregiver well-being, an association was not found (Stephens et al., 1997). In contrast, Hammer and Neal (2008) documented the positive influences of work and family interface on sandwiched caregivers’ lives. Of the few studies that have examined positive work and family spillover, the inconsistent findings underscore the imperative need to examine positive work and family spillover utilizing a population-based sample of family caregivers. As caregivers navigate work and family responsibilities, it is critical that research focuses on positive aspects alongside negative aspects of spillover. This study aims to extend the literature on work and family interface by exploring the moderating role of positive work and family spillover on the association between caregiver type and multiple aspects of well-being.
Method
Participants
Participants were selected from the Midlife in the United States Survey (MIDUS), a three-wave population-based study on the health and well-being of men and women. Data collection started in the mid-1990s with subsequent waves collected 10 years thereafter (Radler & Ryff, 2010). This study utilized the second wave of MIDUS (collected in 2004–2006), which consisted of 5,555 adults aged 28 to 85. Participants were recruited through random digit dialing and completed telephone interview and self-administered questionnaires on topics including demographics, work–family, caregiving, and well-being.
Analytic Sample
Participants were selected into the analytic sample based on a set of selection criteria. Of the 5,555 MIDUS participants in the second wave of MIDUS, 3,338 reported working for pay and were included. Next, individuals who provided care to a family member within the last 12 months were selected (n = 409). Finally, participants who met our selection criteria of filial and sandwiched caregivers (see below for more details) were identified. The analytic sample comprised of 90 filial and 90 sandwiched caregivers.
Predictors
Caregiver type
A set of items was used to identify caregiver type. First, individuals who reported that they provided care to a parent or parent-in-law (“During the last 12 months have you, yourself, given personal care for a period of 1 month or more to a family member or friend because of a physical or mental condition, illness, or disability?”) were selected. Then, a composite variable was created using household structure items to identify whether children lived in the household. Individuals who reported that they provided care to a parent or parent-in-law and did not have any children living in the household were classified as filial caregivers in this study. Respondents who provided care to a parent or parent-in-law and reported having a son or daughter, 25 years or younger, living in the household were identified as sandwiched caregivers. Caregiver type was a contrast between filial caregivers (0) and sandwiched caregivers (1).
Work and family spillover
In line with Grzywacz (2000), spillover was measured with four subscales. The first two subscales assessed spillover from work to family. The four-item negative work-to-family spillover subscale included examples such as “Stress at work makes you irritable at home” and “Job worries or problems distract you when you are home” (α = .85). Positive work-to-family spillover (α = .69) consisted of four items including “The things you do at work help you deal with personal and practical issues at home” and “Having a good day on your job makes you a better companion at home”. The remaining two subscales examined negative and positive spillover from family to work. The negative family-to-work spillover subscale (α = .81) comprised of four items (e.g., “Responsibilities at home reduce the effort you can devote to your job” and “Stress at home makes you irritable at work”). Examples from the four-item positive family-to-work spillover subscale (α = .69) included “Your home life helps you relax and feel ready for the next day’s work” and “Talking with someone at home helps you deal with problems at work”. Respondents rated the items using a 5-point scale (1 = all of the time to 5 = never). Responses were recoded such that higher values indicated higher levels of spillover. For each subscale, items were summed so that higher scores represented higher levels of spillover.
Outcomes
Negative affect and positive affect
To assess one aspect of well-being, negative and positive affect scales from Mroczek and Kolarz (1998) were utilized. Using the response options of 1 (all of the time) to 5 (none of the time), participants rated their affect in the past 30 days. Examples from the six-item negative affect scale (α = .85) included nervous, restless, and hopelessness. The six-item positive affect scale (α = .91) included cheerful, in good spirits, and satisfied. Items were recoded such that 1 reflected none of the time and 5 represented all of the time. The items were averaged within each domain with higher scores corresponding to higher levels of the respective scales.
Psychological well-being
The Ryff scale of psychological well-being consisted of six subscales measuring different dimensions of well-being (Ryff, 2014). Each of the Ryff subscales comprised of seven items and was measured from 1 (strongly agree) to 7 (strongly disagree). The autonomy subscale (α = .64) included items such as “My decisions are not influenced by what everyone else is doing” and “I tend to worry about what other people think of me”. The environmental mastery subscale (α = .73) included the items, “In general, I feel I am in charge of the situation in which I live” and “I often feel overwhelmed by my responsibilities”. The example items, “I have the sense that I have developed a lot as a person over time” and “When I think about it, I haven’t really improved much as a person over the years” were measured in the personal growth subscale (α = .75). Items from the purpose in life subscale (α = .70) included examples such as “I have a sense of direction and purpose in life” and “My daily activities often seem trivial and unimportant to me”. The positive relations with others subscale (α = .80) captured information such as “Most people see me as loving and affectionate” and “I have not experienced many warm and trusting relationships with others”. The self-acceptance subscale (α = .80) comprised of the items “In general, I feel confident and positive about myself” and “In many ways I feel disappointed about my achievements in life”. All items within each subscale were recoded with higher values corresponding to higher levels of well-being. In this study, the different subscales also were averaged for an overall psychological well-being.
Global well-being
Participants rated their overall mental or emotional health from 1 (excellent) to 5 (poor). Responses were reverse coded such that higher values reflected higher level of global well-being.
Control variables
A set of caregivers’ characteristics was examined in the analyses. Both age and education have been linked to aspects of caregiver well-being (Carmichael & Ercolani, 2016; Do, Cohen, & Brown, 2014) such that older adults and those with higher levels of education exhibited higher levels of well-being. Age in years and highest level of self-reported education (e.g., a high school degree or less, some college, a college degree or higher) were examined. This study also considered the caregivers’ sex (male vs. female) and race (White vs. other) because past findings have shown that women and racial minorities participated in a greater amount of family responsibilities than men and Whites individuals (Dilworth-Anderson, Williams, & Gibson, 2002; Morgan, Williams, Trussardi, & Gott, 2016). Marital status (married vs. other) also has been demonstrated to have differential impacts on caregiving responsibilities (Henz, 2010). Brehaut et al. (2009) found that higher levels of caregiver chronic conditions were associated with lower levels of well-being, and thus, the number of chronic conditions (e.g., diabetes and asthma) experienced in the past year was included.
Analytic Plan
First, descriptive analyses were carried out to examine the analytic sample using analysis of variance and chi-square tests. Then, a set of multiple linear regression models were conducted to examine the associations between caregiver type and aspects of well-being. The association between caregiver type (e.g., filial and sandwiched caregivers) and well-being (e.g., negative affect and positive affect, psychological well-being, and global well-being) was analyzed. To examine the moderation effect of work and family spillover on caregiver type and aspects of well-being, interaction models were tested at one standard deviation above and below the mean. Continuous variables in the analyses were centered to aid in interpretation (Hayes, 2017). Missing data were addressed using listwise deletion. Preliminary regression analyses with all of the covariates were conducted; however, age was the only significant covariate. Because the nonsignificant covariates did not significantly change any of the estimates, they were dropped from the final regression models.
Results
Descriptives
Descriptive analyses (see Table 1) showed that filial caregivers were significantly older (mean [M] = 54.56 years, standard deviation [SD] = 6.43) than sandwiched caregivers (aged 46.16 years, SD = 5.96). A majority of caregivers were female, White, and married. Filial caregivers were less likely to have a college degree when compared with sandwiched caregivers. No significant differences in sex, race, marital status, and education existed between filial and sandwiched caregivers.
Demographics of Filial and Sandwiched Caregivers.

Note. M = mean; SD = standard deviation.
*p < .01.
Caregiver type on aspects of well-being
It was hypothesized that sandwiched caregivers would exhibit higher negative affect, lower positive affect, lower psychological well-being, and lower global well-being than filial caregivers. In contrast to predictions, findings from regression analyses showed that the main effect of caregiver type did not significantly differentiate the aspects of well-being.
Caregiver type and work–family spillover on aspects of well-being
The next set of analyses examined the moderating role of work and family spillover, specifically the quality (negative or positive) and directionality (work-to-family and family-to-work), on aspects of well-being. In the examination of negative work-to-family spillover, it was hypothesized that sandwiched caregivers with high levels of negative work-to-family spillover would exhibit higher negative affect, lower positive affect, lower psychological well-being, and lower global well-being when compared with filial caregivers with high levels of negative work-to-family spillover as well as filial and sandwiched caregivers with low levels of negative work-to-family spillover. This hypothesis was partially supported in that negative work-to-family spillover moderated the association between caregiver type and negative affect (b = 0.07; standard error [SE] = 0.03; p = .02; see Table 2, Model 1b). Interactions were tested at low and high levels of work-to-family spillover defined as one standard deviation below and above the mean, respectively. As shown in Figure 1, sandwiched caregivers with high levels of negative work-to-family spillover also exhibited significantly higher levels of negative affect (work-to-family spillover estimated at high levels: b = 0.27; SE = 0.03; p = .02) when compared with filial caregivers with high levels of negative work-to-family spillover and filial and sandwiched caregivers with low levels of negative work-to-family spillover. Negative work-to-family spillover did not significantly moderate the relationships between caregiver type and positive affect, psychological well-being, and global well-being.
Interaction Models of Caregiver Type and Work and Family Spillover on Well-Being.

Note. SE = standard error.
aCareiver type was coded; 0 = filial caregivers and 1 = sandwiched caregivers.
bNegative work-to-family spillover.
cNegative family-to-work spillover.
dAge in years.
*p < .05. **p < .01.

Caregiver type and negative work-to-family spillover on negative affect.
Next, this study investigated the ways in which negative family-to-work spillover moderated the relationship between caregiver type and aspects of well-being. It was hypothesized that sandwiched caregivers with high levels of negative family-to-work spillover would exhibit higher negative affect, lower positive affect, lower levels of psychological well-being, and lower global well-being compared with other caregivers. The interaction between caregiver type and negative family-to-work spillover on negative affect was significant (b = 0.07; SE = 0.03; p = .02; see Table 2, Model 2b and Figure 2). Similar to testing the slopes for work-to-family spillover, low and high levels of negative family-to-work spillover were defined as one standard deviation below and above the mean, respectively. Sandwiched caregivers with high levels of negative family-to-work spillover exhibited significantly higher negative affect (family-to-work spillover estimated at high levels: b = 0.25; SE = 0.12; p = .02) when compared with filial caregivers with high levels of negative family-to-work spillover and filial and sandwiched caregivers with low levels of negative family-to-work spillover. In investigating psychological well-being (see Table 2, Model 3b), negative family-to-work spillover moderated the relationship between caregiver type and self-acceptance (b =–1.40; SE = 0.47; p < .01). To probe the interaction effects, the slopes were tested at low and high negative family-to-work spillover (b =–4.07; SE = 1.57; p = .01; see Table 2, Model 3b and Figure 3). The interaction was significant only at high levels of negative family-to-work spillover. The final goal, which assessed the moderating role of positive work and family spillover on the association between caregiver type and well-being, yielded no significant findings in either direction (e.g., positive work-to-family spillover and positive family-to-work spillover).
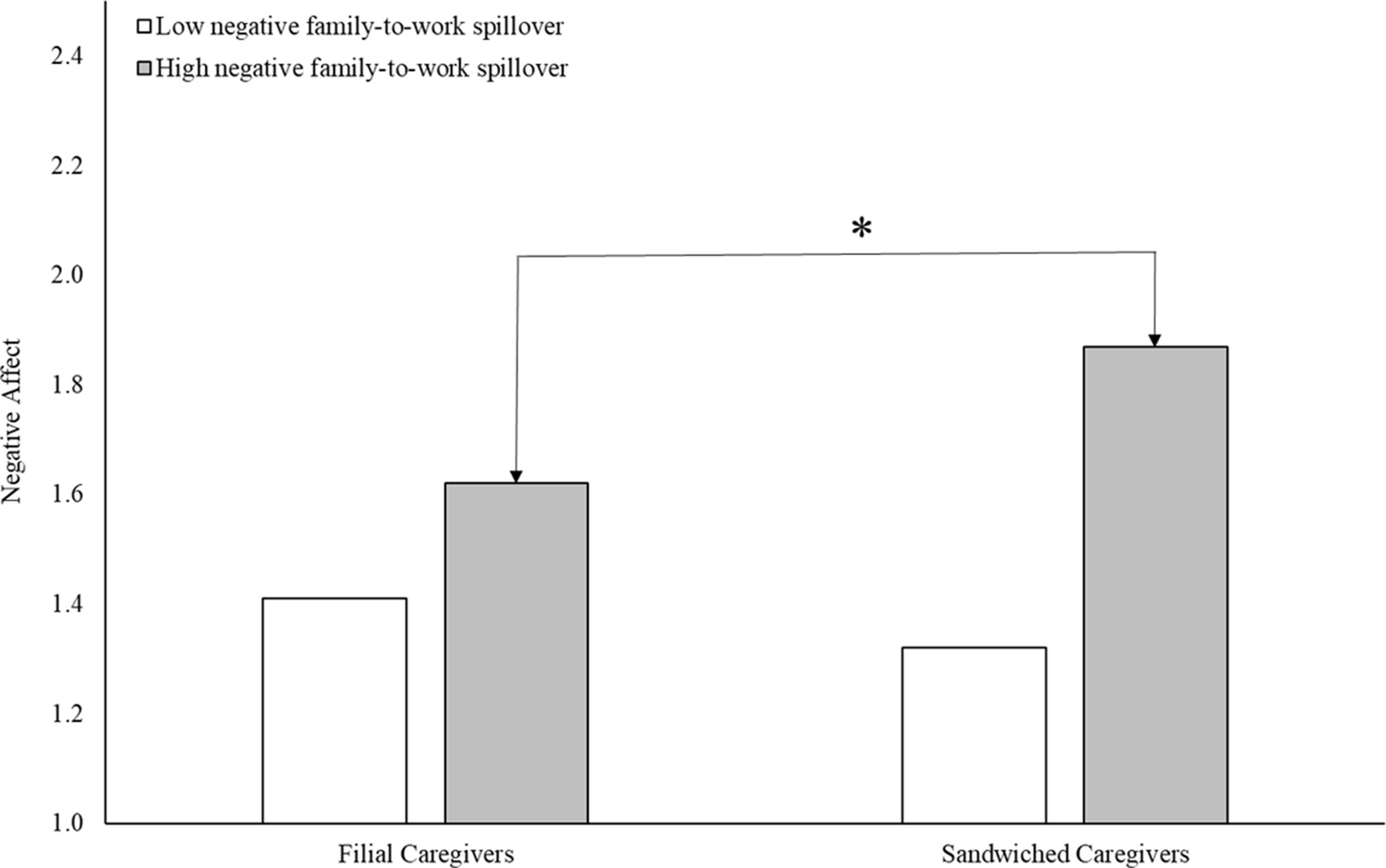
Caregiver type and negative family-to-work spillover on negative affect.

Caregiver type and negative family-to-work spillover on self-acceptance.
Discussion
This study extends and advances the caregiving literature by comparing the well-being of filial and sandwiched caregivers in midlife and late adulthood, a comparison that has been understudied in past literature in the field of aging. Informed by the life course perspective and stress process model, this study also examined contextual factors, specifically work and family spillover, that shape caregiver well-being. Findings highlight the need to examine caregiving in the context of work responsibilities given that the number of working family caregivers continues to grow (Phillips & O’Laughlin, 2017).
Leveraging the population-based MIDUS dataset, this study first sought to compare the levels of well-being between filial and sandwiched caregivers. Contrary to the prediction that sandwiched caregivers would be more susceptible to lower levels of well-being due to multiple caregiving responsibilities, occupying the role of a filial or sandwiched caregiver did not differentiate the aspects of well-being in this study. One plausible explanation is that occupying the role of a caregiver is simply stressful regardless of the type of caregiver and care–recipient relationship (Pinquart & Sorensen, 2004; Silverstein & Giarrusso, 2010). These findings are reflective of the life course perspective as caregivers are not only influenced by their caregiving role but also the interconnectedness of different life domains (e.g., work and family).
While caregiver type did not differentiate the aspects of well-being, findings from this study demonstrate the importance of contextual factors (e.g., work) on the associations between caregiver type and aspects of well-being. In line with the stress process literature, the influences of secondary stressors (work and family spillover) on caregiver well-being were documented. In examining the domains of work and family spillover, sandwiched caregivers who reported negative spillover from work to home exhibited higher negative mood than other caregivers. Thus, in the context of negative events that spilled from work to home, sandwiched caregivers may not have the resources to navigate the additional stressors while managing their regular caregiving responsibilities to multiple generations. A similar pattern also was documented for the moderating role of negative family-to-work spillover. Sandwiched caregivers who experienced more challenges and less support at home also experienced higher levels of negative mood in this study. This finding is consistent with the work of Hammer and Neal (2008) who documented the impacts of negative family-to-work spillover on caregiver well-being, As evident by these findings, it is imperative to consider the context that surrounds the nature of the caregiving to better determine the aspects of caregiver well-being.
Since more attention has been directed at the impacts of negative work and family spillover on well-being, it was important to examine the role of positive spillover on caregiver well-being. In this study, positive spillover did not moderate the associations between caregiver type and well-being. This finding is in line with past literature that showed positive experiences are less salient than negative experiences (Leger, Charles, & Almeida, 2018; Marks, Franklin, & Zoellner, 2018), which highlights the greater need to identify ways to reduce the negative spillover between work and family rather than increase positive spillover.
Several considerations need to be accounted when interpreting the study findings. This study capitalized on MIDUS, which is a population-based survey of adults in the United States. MIDUS is not a caregiver focused survey, and thus, detailed characteristics about the caregivers, such as hours spent on care and burden, could not be examined. The strength of using a population-based survey such as MIDUS is that the caregivers in this study are more representative of the population. This study focused on well-being at one time point, which cannot parse out the causal effects of caregiver type and work-family spillover on aspects of well-being. Future studies could utilize the daily diary portion of MIDUS to better determine the causal linkages among caregiving, work-family, and well-being by examining the lagged effects stressors on well-being and vice versa.
The study findings have the potential to inform education programs and work policy change. With the rise in numbers of working family caregivers (Phillips & O’Loughlin, 2017), more individuals may find themselves navigating caregiving responsibilities and work obligations. Education programs adapted to work or online environments that equip caregivers with adaptive coping skills to better navigate stressors at work or home may help to reduce the carryover of negative work and family experiences (Bauer & Sousa-Poza, 2015). These programs should pay special attention to topics such as balancing time and coping with stress at work and at home. Caregivers who feel overloaded by the negative spillover between work and family domains also could benefit from support in the workforce (Shockley & Allen, 2007). Specifically, caregivers could maximize benefits from the Family and Medical Leave Act. Caregivers who take advantage of this policy may be better protected from unpaid work absences due to caregiving responsibilities. A supportive work environment may lessen the impacts of negative work events, decrease psychological distress, and increase productivity, engagement, and workforce retention (Phillips & O’Loughlin, 2017; Shockley & Allen, 2007).
Conclusion
This study contributes to the existing literature on family caregivers by addressing the overlooked comparison of filial and sandwiched caregivers’ well-being and highlighting the important consideration of the quality and directionality of work-to-family spillover. Together, findings from this study demonstrate the need to examine the context in which the caregiver is embedded to better determine the factors that shape the aspects of their well-being. Finally, the study findings have the potential to inform work policies and promote a supportive and collaborative work environment that may lessen the negative experiences of family caregivers across work and home domains.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The MIDUS II research was supported by a grant from the National Institute on Aging (P01-AG020166) to conduct a longitudinal follow-up of the MIDUS I investigation. The first author was supported by funds from the Graduate Enrichment Fellowship and the Lucile and Roland Kennedy Scholarship at The Ohio State University.