
Abstract
Behavioral and psychological symptoms of dementia are a major reason for institutionalization, and high demanding for staff in Residential Care Facilities. This article reports the design, implementation, and evaluation of a Validation Therapy pilot-training program (VALIDA) for staff members of a residential care facility in Aveiro, Portugal. This pilot study involved 22 members of the staff, including qualified professionals and nonqualified direct care workers, who were involved in the design. The pilot-training program comprises two components: training sessions in group and individual monitoring between those sessions. The evaluation indicates that the structure of the pilot-program was well accepted, and participants reported positive impacts in professional (better skilled to deal with residents with dementia) and personal (better trained to deal with elderly relatives) lives. This pilot-training program shows potential to be used in residential care facilities and needs to be replicated.
Behavioral and psychological symptoms of dementia (BPSD) are linked to superior stress and diminished quality of life among patients, family, and formal caregivers; consequently, these symptoms are amongst the main reasons for institutionalization (Afram et al., 2014; Cerejeira et al., 2012). The most frequent BPSD are depression, anxiety, irritability, apathy, agitation, aggression, psychosis, and sleep changes (Finkel, 2000; Savva et al., 2009). It is estimated that at least 80% of the institutionalized old adults have dementia, and show some BPSD (Quince, 2013).
In Portugal, the family plays a major role in care. However, in high challenging situations, such as dementia, families often resort to formal care services, namely a Residential Care Facility (RCF; Ministry of Labour, Solidarity and Social Security, 2015). In our country, RCFs accommodate a wide range of seniors, since specialized services are limited (Barbosa et al., 2015). The size of these facilities varies substantially, but the average number of available beds is 40. Typically, the RCF has a care-home manager, a qualified professional (usually a social worker) who supervises direct care workers (DCWs; usually nonqualified staff). The DCWs are the core of the care since residents spend most of their time with them. Yet, the majority are middle-aged women and the educational level is typically low, not being required any kind of training in gerontology or in dementia (Barbosa et al., 2015). Therefore, training staff to understand and manage BPSD seems essential for the quality of life of residents with dementia, as well as of the staff (Barbosa et al., 2015; Stone, 2012).
Nonpharmacological interventions (NPI) in BPSD have shown promising efficacy in maintaining and/or promoting function and participation in people with dementia, by managing symptoms and retarding the disease progress (Wang et al., 2018; Zucchella et al., 2018). In Portuguese RCFs, reality orientation (RO) is the most widely strategy used for dealing with people with dementia (Marques et al., 2013). Not so much due to its effectiveness, but because it is the most obvious and known strategy. Still, RO is often associated with a misunderstanding of dementia, at least in the early stages that combine moments of orientation and disorientation (Barbosa et al., 2015). RO frequently makes caregivers experience extra frustration, since they repeatedly try to orient the person, with little noticeable long-term effect (Hitch, 1994).
In this study, we adopt validation therapy (VT) to train staff in an RCF, because it consists of communication strategy that can be used in a daily routine basis, and accessible to all persons (Touzinsky, 1998). Naomi Feil developed VT, which is rooted in the Rogerian humanistic approach (Livingston et al., 2005). VT training aims to help caregivers develop communication skills in their interactions with residents with dementia, by accepting the residents’ reality and by validating their feelings with the use of multiple verbal and nonverbal communication techniques (Feil, 1992). It stands on some main principles (Feil & Altman, 2004; Feil & Klerk-Rubin, 2012): all people should be accepted as they are; there is a reason that underlies every behavior; when feelings are suppressed, these feelings will gain strength; and, people can live on several levels of awareness at the same time. According to VT, many people with dementia enter a final life struggle called “resolution” of unfinished issues to die in peace, which goes through four phases (Feil, 1992). In the first phase, malorientation, the person is mostly oriented to time and place, and starts expressing past conflicts in disguised forms. In the second, time confusion (TC), the person is not oriented to time and place, and is no longer holding onto reality. In the third, repetitive motion (RM), the person uses movements instead of speech to express human needs and/or to work through unresolved conflicts. In the fourth, vegetation, the person gives up trying to resolve living, has minimal movement, blank expression, and no speech. VT techniques may be delivered one-to-one, in a group setting, or used in the daily routine by caregivers to communicate with people with dementia. VT considers that when people express emotions that have often been suppressed for many years, the intensity of the feelings diminish, people communicate more and are less likely to withdraw into further stages of disorientation (Feil & Klerk-Rubin, 2012). The evidence for VT is still small and shows mixed findings. A case-control study (Tondi et al., 2007) suggests that VT is able to reduce the frequency and severity of BPSD. However, other reviews found insufficient evidence (Livingston et al., 2005; O’Neil et al., 2011; Olazarán et al., 2010; O’Connor et al., 2009). Studies on VT effects are challenging due to ethical, practical, and methodological problems, mostly because more than the techniques, what is effective in VT is the affirmation of the person’s value, the greater attention to their needs, and the emotional support (Deponte & Missan, 2007; Finnema et al., 1998).
To our best knowledge, seven intervention programs using VT and targeting formal caregivers have been published (from 1995 to 2014). Three studies (Finnema et al., 2005; Schrijnemaekers et al., 2002; van der Kooij et al., 2013) investigate the effect of EOC that included VT, and the remaining four use VT as the main intervention (Canon, 1995; Söderlund et al., 2011, 2014; Toseland et al., 1997). All studies involve supervision (except Canon, 1995) and control group (except Söderlund et al., 2014). Main results indicate that staff changed the communication strategies with the residents with dementia, and reported increased satisfaction and reduced stress symptoms; positive changes in the qualitative nature of relationships between staff and residents; reduced physically and verbally aggressive behavior by the residents; and improved work climate.
To the best of our knowledge, VT training programs were never implemented in Portugal before. The aim of this study is to design, implement, and evaluate a VT pilot-training program (VALIDA) for staff members of an RCF in Aveiro, Portugal.
Design
The program was named VALIDA, which is an acronym that brings together two Portuguese words, meaningful within the VT: “validar,” which means to validate; and “vida,” which means life. It was developed based on research and literature from the VT (Feil & Klerk-Rubin, 2012; Feil, 1985; Sunrise Senior Living, 2011). The aim of VALIDA is to improve the skills of an RCF staff on VT techniques, in order to better understand and manage BPSD, and consequently improve well-being for both residents and staff (Kuske et al., 2007). VALIDA was performed in an RCF in Aveiro with around 36 residents, with different degrees of in/dependence, and variable mental perturbations (nine diagnosed with dementia). VALIDA was approved by the direction of the institution and announced according the institution’s common procedures (a poster in the staff room with key information: topics, schedule). Informed consents were obtained from all the participants.
VALIDA design embeds the needs reported by the staff. The first author was in the RCF for 1 month (around 15 hr per week) in order to collect the needs, to observe and become familiar with the context, and to bond with the staff. The needs and difficulties, gathered during dialogs through daily work routine, comprise two main topics. First, general information on understanding dementia as a chronic disease (sometimes it is assumed that people with dementia pretend some behaviors, such as swearing). Second, dealing with specific behaviors of residents with dementia, in particular regarding resolution stages two (TC) and three (RM), the most common in the RCF. The staff reported struggling with people in TC, since they “ask questions and demand answers,” and staff often have “to lie” since they do not know another way (lying reported as a big burden). Regarding RM, the staff struggled with the bizarre and intrusive behaviors (as clap hands and/or grave others), since this promotes conflicts between residents.
Planning a training program in an institution that operates 24/7 demands adjusted arrangements. It was decided that the participation was voluntary (although highly encouraged), there was no previous registration, and participants could attend the session/s they wished (i.e., a participant could come just to session 3, or could attend all of them). In addition, it was decided to carry out each session twice, so the participants could choose the one that better adjusted to their schedule. Moreover, the RCF has 28 staff members, which would be too big for just one training group. All the sessions were scheduled for Tuesday (previously defined by the RCF as the day for training; from 10:30 to 11:30 a.m., or 3 to 4 p.m., the periods between residents’ mealtimes).
Implementation
Globally, 22 (out of 28) staff members participated in at least one session; 15 were present in at least three sessions, and were considered the completers (Table 1). Participants’ average age is around 46 years old; mostly females, predominantly DCWs, with 5 to 9 years of experience, low education, frequently without education on gerontology and/or geriatrics. Completers’ average age is higher (around 48 years old); all female, with almost half of them having up to 4 years of schooling; with the exception of two completers, all are DCWs, have no education on gerontology and/or geriatrics, and predominantly with 5 to 9 years of experience.
VALIDA: Participants and Completers.
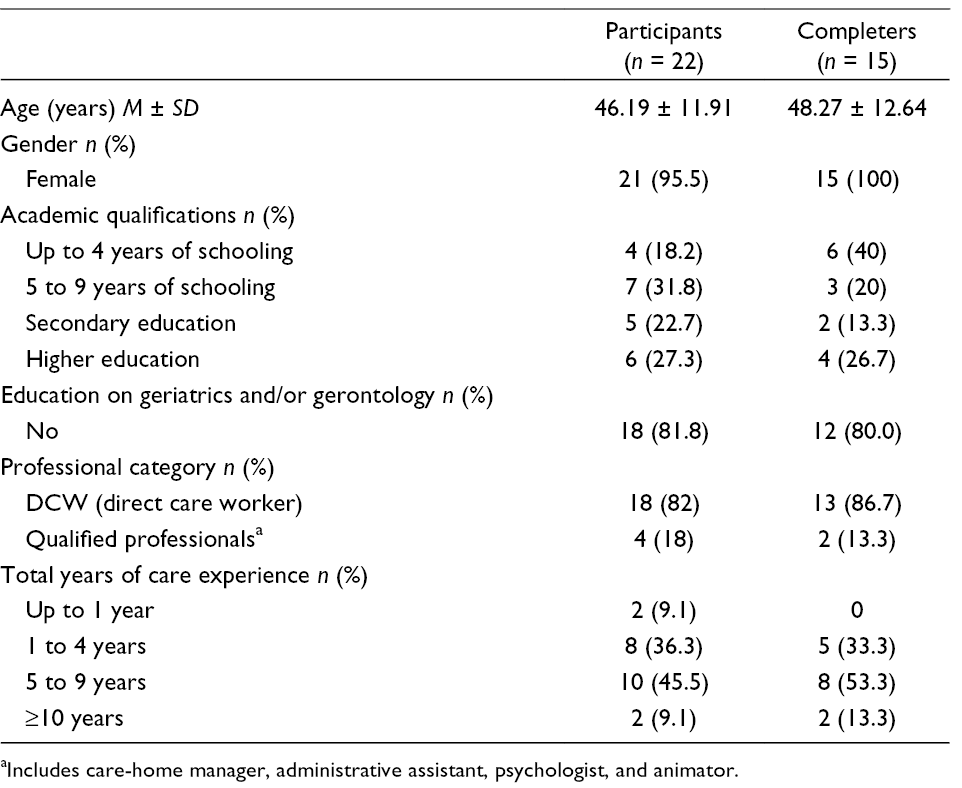
aIncludes care-home manager, administrative assistant, psychologist, and animator.
VALIDA comprises two components, carried out by a facilitator (1st author): training sessions in group and individual monitoring between sessions.
Component: Group-Training Sessions
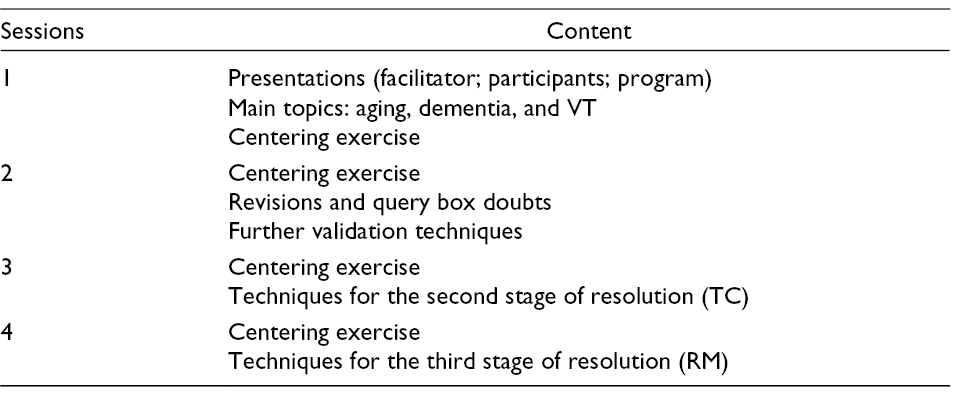
The group training includes four sessions held for a period of 6 months, each planned for 60 to 90 min duration. The four sessions had a similar structure (Table 2). In each, the participants received handouts summarizing the important information. It was planned to have a query box available during all the program for participants to expose their issues; however, they preferred to expose their doubts personally to the facilitator during the monitoring (the box was removed after the second session). The methods/activities involved theoretical exposition of contents, debate, sharing of experiences, clarifying doubts, and playing games.
VALIDA: Sessions Structure.
The first session begins with the personal presentations of each participant, including the facilitator; each one describes the colleague sitting next to them, indicating the name, main hobbies, and favorite artist. This is framed as a way to underline the importance of knowing the preferences of the residents with dementia. Then the aim of the program is stated, as well as the format; and the query box is described.
The main topics involve bringing together aging, dementia, and VT, by gathering what participants already know about the new topic on VT. This is addressed through nine interlinked cards (each comprising a word/expression and a related picture). Randomly, each participant receives one of the cards, and then reads it, to initiate the debate, share experiences, and clarify doubts. The cards are: 1, person with dementia vs person with dementia; 2, communicate; 3, barriers; 4, bridges: empathy, validation, and reminiscence; 5, past (returning to); 6, express (dumping the heavy backpack of emotions); 7, do not argue; 8, do not lie; and 9, levels of awareness. The session ended with the practice of the centering exercise. The participants state that they are always tired, since they have an exhausting job. The session lasted 70 min.
The second session is mainly supportive, aiming to respond to the participants’ questions left in the query box, and introduce further validation techniques. The first question was “what should the caregiver do when interacting with a resident with dementia?” The facilitator suggests three techniques (centering, empathy, and linking the behavior to the unmet human need). The second question was “should we enter their world? Does it mean lying to them?” For the participants, the topic of lying is relevant, since they prefer not to lie, although they lack alternatives. The facilitator explains that entering the person’s world is not lying, but accessing their world, helping him/her to revive pleasurable moments of the past. Some examples involving residents were provided. The third question was “which techniques should be applied when communicating with Mrs. Petra?” The facilitator describes the four phases of resolution, and explains that Mrs. Petra is mostly in TC. Some validation techniques are recommended and exemplified (such as the use of polarity). This session lasted 70 min.
The third session aims to characterize the TC phase and deliver validation techniques for this stage. The session begins with the centering exercise. The facilitator starts by describing the main physical and psychological characteristics of TC. Then, the participants describe features of the residents that match. The facilitator presents the 12 validation techniques recommended for this stage (each printed in A5 cards): centering; factual words; rephrasing; polarity; genuine, close eye contact; ambiguity; clear, low, and loving tone of voice; mirroring; linking the behavior with the unmet human needs; preferred sense; touching; and music. Again, participants (mostly DCWs) are exhausted, and some link the lack of time with not doing the best they should with the residents, and some dissatisfaction with their job performance. Cecília said: “there is always a need behind the behavior, but sometimes we have so much to do that we don’t even think about it. We do so many things wrong in our work!” The session lasted 60 min.
The fourth session aims to characterize RM stage and provide techniques that prevent the withdrawal to vegetation. The session starts with the centering exercise and then playing a board game inspired by Monopoly®, designed for this session: Repetopoly (named to underline the RM phase). Beyond spaces to move on, to move back, or to play again, the game comprises questions, and information spaces, planned to explain the RM phase and techniques. Information spaces contain sentences such as “Memories of early and consolidated movements are revived in order to people in RM survive the painful present.” “Use the ambiguity to respond to the person. If he/she speaks unknown words, use a vague pronoun to answer him/her (“he,” “she,” “it,” “someone.” and “something”).”
Examples of the questions are “True or false? People in RM use body parts or objects to symbolize significant people or events from the past” [Answer: true]. “True or false? It is common at this stage for people to repeat sounds they have learned in childhood, including cackling, groaning and chanting” [Answer: true]. At the end of the session, the participants share their perspectives about the benefits of VALIDA, thank the institution for providing quality training, and congratulate the facilitator for her performance. Camila said: “validation is indeed a therapy to relieve the burden, to die in peace; it works with our emotions.” This session lasted 80 min.
During the sessions, participants were often asked to share examples or events related to the interaction with the residents with dementia and the use of validation techniques. This was an approach used to understand if the participants comprehended the concepts and techniques. Participants shared events both from their professional and personal lives, which suggested their understanding.
Component: Individual Monitoring
Between sessions, the facilitator accompanied each participant (both DCWs and qualified staff) weekly. This component aims to give individual and private attention to each member of the staff and to support them by adopting the VT techniques in daily practice. The facilitator embodies the empathic principle of VT, and in these periods the staff gain support for professional and personal issues. Regarding DCWs, the monitoring occurred mostly at the night shift (6 pm to 11 pm), because it is a quieter moment. In addition, night and in particular bedtime is a moment where “all comes about.” This monitoring was planned to be individual, but in some occasions, it involved two staff members, because they were delivering care together. Often it occurred in the bedrooms, while residents were helped to go to bed. It was mainly a moment to talk about their own life, both personal and professional; doubts about use of the techniques were clarified. This bound the facilitator and the staff, creating a close and affectionate relationship.
In addition, the individual monitoring was a component where the facilitator could observe and discuss with the participants the use of techniques. Overall, the most used techniques were rephrasing, use of factual words, polarity, touch, and genuine eye contact. The staff reported that the most useful technique was touch, since they found it easy to use and that it produced calmness and/or affectionate reactions from residents rapidly. The most difficult technique was mirroring behaviors and emotions, mostly because they were afraid of mimicking. The areas of further guidance were related to the difficulty of the staff in using VT consistently; previously the staff used RO, and still have the tendency to go that way, mainly when they use a validation technique and do not obtain the desirable behavior quickly. For example, the staff tended to lie instead of rephrasing, particularly when the residents did not calm down rapidly after the use of rephrasing.
Evaluation
This pilot-training program was evaluated in order to collect suggestions from the participants to better adjust it to their needs; and to capture the program clinical significance (Fraenkel, 2006; Sousa & Rodrigues, 2008) for the participants (positive and negative impacts, at both personal and professional levels). It involves two moments: after each training session through a questionnaire, to gather participants’ suggestions, since this would allow for immediate improvements; and, 6 months after that, to gather further suggestions to improve the program, to capture the clinical significance and understand what techniques the staff were still using.
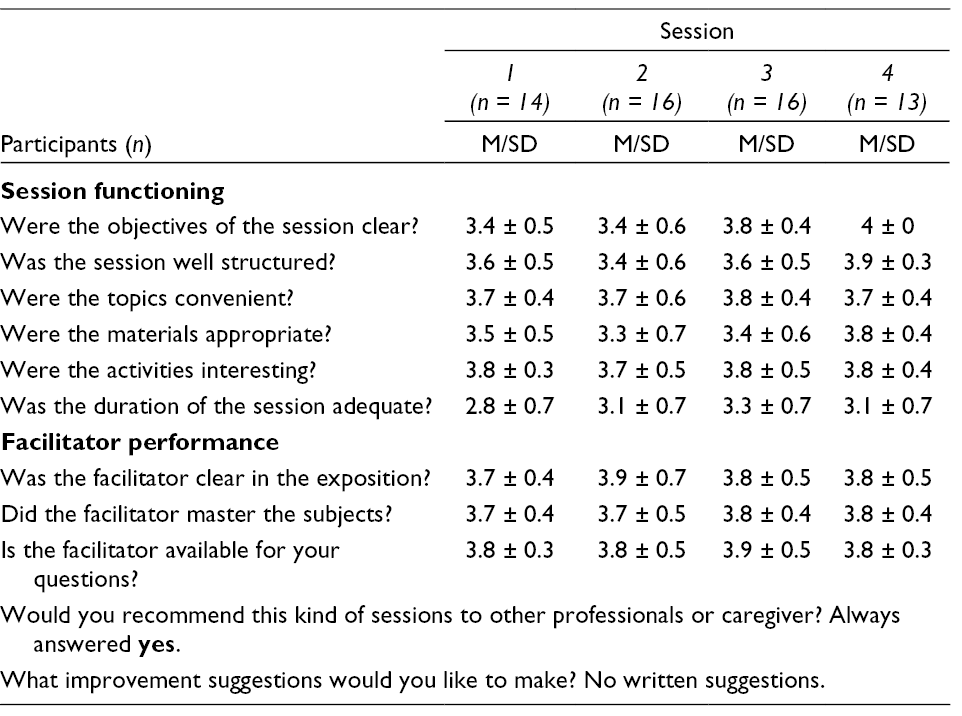
Two instruments were used. A postsession individual questionnaire designed to evaluate the functioning of each session, based on a four-point Likert scale (1: insufficient, 2: sufficient, 3: good, and 4: very good), comprising nine items; six of them evaluate session functioning, and three assess facilitator performance. There were also two open questions (Table 3).
Postsession Questionnaire Means.
For the second moment, a focus group was performed through a semistructured interview, consisting of three questions: (1) What is your opinion concerning the functional aspects of the VALIDA? (2) What is your opinion concerning the contents and activities used in the sessions? and (3) What are the personal and professional impacts, both positive and negative? The interviews were carried out in groups (5–8 elements) with the completers (e.g., Table 2). The participants listened to other participants’ responses and made additional comments as they went along, knowing that they did not have to reach any kind of consensus or disagreement. The interviews were performed by the facilitator at the participants’ workplace with an average duration of 60 min; they were transcribed and submitted to narrative analysis (Riessman, 2008).
Results
Regarding the questionnaire, results indicate that means are all around the value 4 (very good); except for the item relating to the duration of the first session that was scored at a lower value, since the participants considered the sessions should be longer. Concerning the open questions, all participants responded that they would recommend VALIDA to other professionals or caregivers, and no written suggestion was made.
In the focus group, with regard to the spacing between training sessions, participants would like to have them twice a month (rather than one a month); however, they recognize that "logistically it’s difficult" (Cândida). They consider that the duration of each session from 60 to 90 min is enough, because “if sessions were longer, we would fall asleep” (Claúdia). About the composition of the training groups, all participants agree that it was good to "mix everyone" (Clara), "regardless of their level of education" (Celeste) and function, because "we are a team; we participate in everything together all year long. (...) It doesn’t make sense to be selective here" (Carmen), and "it is the importance of multidisciplinary" (Cândida). They point out that "we also get to know each other better" (Clara), because in the work routine it is not always possible. For the number of participants in each session, participants consider that "it has never affected us, as long as we respect each other. It is important to listen to our colleagues, not interrupting the other person" (Clara). Regarding the adequacy of the themes, participants consider that "it was good, because they were about our day-to-day work and clarified our doubts" (Clarinda), and "sometimes were about our life, which is also important" (Clara). They emphasize that the themes were appropriate since "all the things we talked about here, we actually do it in practice" (Cármen). However, they point out that "sometimes it is difficult not to lie" (Cármen), and "sometimes lying is the way" (Carolina), otherwise "we lose control of the situation and consequently they [residents] become more disoriented" (Cecília). Concerning the methodologies, which combined expositive and active method, they consider that "both are essential, the most theoretical part first, and then the practical part to apply the new concepts" (Cristina). The group context is also valued, since it allows normalization ("I did like sharing experiences with the group, and knowing that my colleagues also have similar situations in their interactions with residents," Carolina) and cooperation ("to help each other how to deal with residents’ behavior. If it worked well in this way, and the resident was quieter, I can share my technique with the group," Claúdia). Participants emphasize the fun and learning playing Repetopoly.
Participants Did Not Report Negative Impacts
The positive impacts were felt on both personal and professional level. On a personal level, participants said that it was useful for their lives (Celeste: "we learned not only to apply the techniques to the residents, but also to ourselves. We learned to release what is going on inside us, to dump the heavy backpack of emotions"), and to deal with their relatives (Clara: "it helped me to better understand my mother, who was diagnosed with Alzheimer... It also helped me to accept her the way she is right now"). Participants state that VALIDA has helped them to separate the professional life from the personal life (Celeste: "we separate work from home affairs; sometimes we took work issues home with us, and vice versa. Now I can separate things a lot better because it was not being good to me"). On a professional level, they felt that VALIDA has helped them: (1) feeling more empowered and skillful, and less stressed (Clara: "I’m more satisfied with what I am doing. I feel more secure in performing everyday care and satisfied to be able to do a little more for the residents”). (2) To better understand dementia, and accept the person with dementia (Carla: "gave me another sensitivity with residents with dementia and dementia itself"). (3) Understanding and supporting colleagues, releasing emotions, and improving communication skills (Celeste: “we learned to (…) dump the heavy backpack of emotions and to express more what we think and feel"). (4) Dealing with conflict situations with residents (Cristina: "it helped me to better solve tricky situations with residents").
During the focus group some participants’ commented some alterations they made in the interaction with the residents after the VT training, that were also observed by the facilitator, namely: (1) more eye contact (for instance, go down to the same eye level of the seated resident to talk to him/her). (2) More understanding toward the person, following the VT principles (for instance, when they were moving the wheelchair, they start by telling the resident they were going to do it). (3) Recognizing the resident’s needs (for instance, if a resident was agitated, they care for understanding the need behind). Participants state that before the VT training they did not try to understand the residents with dementia, because they are “demented”; now they understand that these residents are reporting a need from their own reality. Therefore, when they hear a resident with dementia saying something they try to understand the need he/she is trying to report.
Discussion
VALIDA was well accepted by all the participants, with reported personal and professional impacts on their well-being. This pilot-training program was designed and implemented according to VT principles (Feil & Klerk-Rubin, 2012; Feil, 1985). It is our perspective that a VT training program should be congruent by using validation in all its aspects. The design was developed respecting (validating) the setting, the staff, and the residents. The setting, an RCF, is a facility where a number of old persons inhabit (with different ages, degrees of in/dependence, and variable mental perturbations), cared by a limited number of staff 24/7. Therefore, the training sessions need to be limited to a small number for a medium-term period (four sessions in 6 months), and be supported by monitoring during daily routines. The staff were involved in a voluntary basis, without previous registration, and could attend the session/s they wished/could. This is a way to validate the emotional and physical demands of the job, where staff have to deal in a daily basis with suffering, mental perturbation, and mostly working shifts. The residents were not directly involved, but sessions were designed considering the main resolution phases of dementia in the RCF, and monitoring was performed also in direct care.
In terms of implementation, the participants state that VALIDA was well structured regarding the spacing, duration, contents, methodologies, composition of the groups, and number of participants. The themes addressed the daily care and life issues, which are both considered important and appropriate. Concerning the methodologies, its order is emphasized (the lecture before the practical), and the Repetopoly is highlighted for its educational and fun purposes. Therefore, for a staff with a high demanding job, it is relevant to adopt a mix of methods. The groups in the training sessions involved members of the staff, despite their education and function; the participants consider this a good option, because they are a team. The participants state that a group context is important, since it allowed for the normalization of experiences and promoted cooperation between staff’ members (Barbosa et al., 2015). In addition, they also valued the individual monitoring, because it allowed for the possibility of clarifying doubts and building a close relationship with the facilitator. The facilitator’ role in VT training needs to be emphasized. The communication incongruence, that is, when verbal and nonverbal information are inconsistent, diminishes trustworthiness (Morioka et al., 2016). Therefore, the facilitator needs to embody the validation methods and be empathic. It is also relevant that the facilitator spent time in the RCF (beyond training) to know the RCF dynamics, the staff, the residents’ characteristics (and have examples from the residents in the training).
The participants underline two main difficulties: lying, and conflicts. Lying was the way staff was dealing with the residents in the TC stage, reported as burden they were carrying and needed to release. During the sessions, the principle of not lying was pointed out as difficult; the main uncertainty is whether entering the person’s world and lying are the same (Zeltzer, 2003). This topic requires more attention in future trainings, probably integrated into practical exercises, such as role-playing. Conflicts between residents with and without dementia are common (Ferreira et al., 2019), mainly when residents with dementia are in RM stage, the staff struggle with their own inability to break conflicts. Beyond the techniques shared within the program, future training could involve a VT component for the oriented residents.
The clinical significance of the pilot-training program revealed that participants felt well-being on both personal and professional levels, and the improved capacity to separate personal life and work. On a personal level, the participants state that they were offered techniques, which allowed them to deal with their elderly parents and to work internally on themselves. Professionally, staff state empowerment, self-efficacy, and less stress. Mostly DCWs underlined that this was the first time they had someone to also care for them, which make them feel more valued and supported, and consequently more confident about their skills. In-between sessions monitoring establishes a close relationship between the staff and the facilitator, maintaining the adherence to the training. Additionally, the participants report that the training helped them to support each other; and they are still using the techniques they learned, both personally and professionally.
Although validation techniques require training, they are also intuitive/natural, since “validation respects the intuitive wisdom” (Feil, 1982); most of the staff involved in the training had plenty of experience of working with people with dementia, and they reported understanding the adequacy of VT. In addition, our perspective is that the understanding of the VT principles are the basis for acquiring validation techniques, since participants often made that link during monitoring.
RCF in Portugal struggle with balancing the budget, since it is a high cost service that serves the older population, who usually receive low pensions. Therefore, costs are an important issue. VALIDA demands a professional with training in VT, working part-time for about 6 months. However, it may have high benefits, such as diminishing stress levels of residents and staff; lessening doubts related to dementia and consequently improving care quality; and promoting a good work climate where staff members support each other and show more support for each other.
Limitations and Research Perspectives
The main limitation of this pilot-training program is the small number of participants. Further studies should involve the replication of this program in other RCFs, in order to increase the participants; this would also allow to combine qualitative and quantitative measures, and to carry out randomized control trials. It would be relevant to assess staff well-being, job satisfaction, work climate, and perceived stress levels (Söderlund et al., 2014). The individual monitoring component could be enhanced by using supervision (Söderlund et al., 2011) including a video recording of one conversation with the same resident once a month, plus feedback from the supervisor. This would also allow us to assess the changes in the staff-residents interactions, and get a better understanding of the validation techniques more/less used by the staff, as well as those they had more/less difficulties using.
In terms of further improvements, it would be relevant to add two other components to the program: VT training with the oriented residents to increase understanding to diminish conflicts; and VT training with family members, for a better understanding, and reinforce the approach by the staff.
Footnotes
Acknowledgments
The authors gratefully acknowledge the RCF and its staff members for their participation in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by grants from the National Funds through FCT - Fundação para a Ciência e Tecnologia within CINTESIS, R&D Unit (reference UID/IC/4255/2019).
Author Biographies