
Abstract
This study investigated perceived support received by partners and its association with quality of life (QOL) in older couples facing skin cancer. Thirty couples (n = 60; M Age = 70) in which one partner had a skin cancer diagnosis (PwSC) completed either online or paper surveys about their skin cancer diagnosis, perceived partner support, and overall QOL. Actor–partner interdependence models revealed that when PwSCs reported overprotection from their healthy partners (HPs), they were more likely to report lower QOL. Protective buffering received by HPs was negatively associated with their QOL as well as their PwSCs QOL. Active engagement support, however, was not associated with either partner’s QOL. While couples may use all three styles of relationship-focused support, protective buffering and overprotection affected each partner’s QOL. Implications of the study findings for interventions for couples facing illnesses like skin cancer are discussed.
Skin cancer has obvious physical bearings on patients, which are often ignored; however, they are the consequences of skin cancer on the patient’s and their partner’s quality of life (QOL). Previous research has indicated that skin cancer has a negative impact on persons with skin cancer, for both those with nonmelanoma (Gaulin et al., 2015; Radiotis et al., 2014) and melanoma (Beutel et al., 2015; Trask et al., 2001). For example, skin cancer treatment can contribute to fatigue (Albrecht et al., 2013), changes to sexuality (Kasparian, 2013), and poorer body image (Atkinson et al., 2013), which further contribute to psychological distress (Beesley et al., 2015; Kasparian et al., 2009; Trask et al., 2001). Additionally, anxiety or fear over the diagnosis, treatment, or long-term prognosis has also been found to be associated with lower QOL (Stark et al., 2002).
While the past research presents a strong case for the effect of skin cancer on QOL for the partner with skin cancer (PwSC) and how poor QOL can be associated with other underlying concerns, most research has been conducted as though patients cope on their own. Few studies have examined the role of spouses and partners in the disease process. Distress or fears resulting from partners’ skin cancer diagnosis altered social roles and limited social activities which may affect healthy partners (HPs) such that they too may experience poorer QOL. HPs may feel anger toward skin cancer, medical professionals, or even themselves if they feel they should have noticed skin concerns earlier (Woźniak & Iżycki, 2014). Previous research on couples coping with various cancer diagnoses, including skin cancer, found that HPs report negative impacts on family relationships and less social support to them compared to the partners with cancer (Northouse et al., 2000). HPs have also found that family communication was an important factor that impacted HP’s anxiety and depression (Edwards & Clarke, 2004) and perhaps their QOL. Thus, additional knowledge about both partners’ QOL when facing skin cancer can inform psychoeducational services or guide services from other human services professionals.
The main objective of this study was to address gaps in the literature on QOL of both PwSCs and their HPs to highlight the role of relationship-focused support as a mechanism of change that promotes positive QOL in couples experiencing skin cancer. An understanding of how both partners support one another and what associations such support have with QOL of both can inform support groups and couple’s therapy sessions, providing opportunities to help couples understand how they can best support one another.
Literature Review
Worldwide, skin cancers account for more cases than all other types of cancer combined (Roberts et al., 2013). An estimated 3–4 million people in the United States are diagnosed with nonmelanoma skin cancers each year (American Society of Clinical Oncology [ASCO], 2017), and 87,000 new cases of melanoma are diagnosed annually (American Cancer Society, 2017). The average age for diagnosis of melanoma in the United States is about 63 years (American Cancer Society, 2017). The increase in the incidence of melanoma begins around the age of 60 and continues to increase after age 60 (Cancer Research, UK, 2016). This is primarily due to the well-documented link between cumulative sun exposure and skin cancers (Fartasch et al., 2012).
Further, incidence rates for melanoma have recently been increasing at a rate roughly ten times higher for individuals over the age of 65 compared to those under the age of 40 (Lasithiotakis et al., 2010). Researchers have postulated other reasons why older adults face more risk from skin cancer than younger individuals (Yuce et al., 2014). One contributing factor to the increased skin cancer risk as individuals age is a normative weakening of the immune system, which lowers an individual’s ability to fight disease, including skin cancer (Lasithiotakis et al., 2010). Also contributing to this potential increased risk is that older adults may be less observant of changes to their skin and pay less attention to early symptoms compared to younger adults. Thus, older adults may be less likely to participate in skin cancer screening programs. Skin cancer is an area of concern for many older adults, and as such, is an area of opportunity for researchers, including examination of how skin cancer affects older adults and how those in couple relationships support one another.
Stressors and Experiences of Skin Cancer
Experiencing a skin cancer diagnosis can be stressful for both individuals with the diagnosis and others, including romantic partners, other family members, or friends. Persons with skin cancer may experience uncertainty when the diagnosis is first made (Stamataki et al., 2015) or stress about making treatment decisions (French-Rosas et al., 2011). Individuals may experience heightened depression or anxiety if cancer reoccurs (Kasparian et al., 2009), or worry about physical changes resulting from the skin cancer, especially concerns about actual or potential scarring due to surgical procedures (Stamataki et al., 2015). Additionally, families may have financial concerns due to unexpected medical expenses. In more advanced stages of skin cancer, individuals may have to take time away from work for treatment or for recovery following treatment, which may contribute to additional financial stress (Morris et al., 2009).
As evidenced by research on other types of cancer, skin cancer can also cause stress for HPs. The stress experienced by HPs can be the result of multiple stressors that accompany the skin cancer diagnosis, including becoming an advocate for the PwSC, changes in relationship dynamics, or concerns over financial and insurance needs. For example, the uncertainty and waiting during the initial diagnosis process can be a source of stress for HPs. They may feel helpless or frightened of the future. HPs often experience as much emotional distress as, if not more than, the partners with the cancer diagnosis (Northouse et al., 2000). Couples may also experience negative impacts on communication, which can be an additional challenge for HPs (Hawes et al., 2006). Partners may avoid communication to protect one another from fears or other negative emotions (Boehmer & Clark, 2001). During treatment, HPs may experience role shifts, such as taking over additional family responsibilities (Manne & Badr, 2010). Additional stressors for HPs may come from changes to physical intimacy during or after treatment (Lindau et al., 2011), especially if the PwSC experiences negative changes to his or her body image and self-confidence (Fingeret et al., 2014). Similar to PwSCs, HPs may also experience concerns over the financial implications of treatment (Morgan et al., 2011).
Relationship-Focused Support
Social support, including support from romantic partners, is beneficial in helping individuals adjust to stressful situations, including cancer diagnoses. For example, in their study of individuals with melanoma and nonmelanoma, Pereira et al. (2017) found that less perceived social support was associated with poorer QOL. Similarly, Devine et al. (2003) found lower social support to be associated with greater intrusive thoughts and poorer QOL in individuals with metastatic melanoma. Findings from studies with nonskin cancer diagnoses have also highlighted the importance of support. For example, women with breast cancer who were socially isolated from both family and friends before their diagnosis were at an elevated risk of mortality compared to women who had strong social support (Kroenke et al., 2006). As these studies show, receiving social support has an important impacts on individuals with skin cancer, but not all support is helpful.
As couples work together to cope with skin cancer, certain supportive styles may be more effective than others. For example, active support, which encompasses efforts aimed at facing the problem directly and working to come up with possible solutions to reduce any stress, has been found to contribute to better outcomes compared to passive support or strategies used to escape the stressor without confronting it, including lower depression and better QOL (Kershaw et al., 2004; Kim et al., 2010). Passive support is linked to a higher level of stress in women at risk of developing breast cancer (Pieterse et al., 2007). Emotional support from family and friends, characterized by reassurance, comfort, and assistance with problem solving, is associated with viewing a cancer experience through a positive lens following the completion of treatment (Schroevers et al., 2010). As these findings suggest, actively engaging with stressors stemming from a skin cancer diagnosis should be more effective than avoiding or denying stressors.
Although there are numerous ways that researchers have conceptualized and operationalized support, the current study uses Buunk et al.’s (1996) view of relationship-focused support. From this lens, the three styles of support that partners provide are active engagement, protective buffering, and overprotection (Kuijer et al., 2000). Active engagement support involves discussing thoughts and feelings and using joint problem solving to cope with a stressor (Hagedoorn et al., 2011; Schokker et al., 2010). Protective buffering support includes partners hiding or suppressing worries or fears about a stressor, or actively avoiding discussions about the stressor. Finally, overprotection encompasses an underestimation of the person with the chronic illness abilities, which results in help that is unnecessary and damaging, excessive praise for accomplishments, and attempts to restrict activities of the partner (Kuijer et al., 2000).
While research focused specifically on the use of relationship-focused support by couples facing skin cancer is limited, researchers have studied this style of support in couples coping with other cancer diagnoses, including breast, colon, and colorectal cancers. A review of these studies illustrates an examination of a variety of physical and psychosocial outcomes, such as relationship improvement when partners use more active engagement support behaviors and a positive association between overprotection and partner distress (Hagedoorn et al., 2011; Kuijer et al., 2000). However, not all findings of potential benefits of relationship-focused support are clear-cut; for example, the use of active engagement support by a partner may be associated with increased psychological distress in partners with cancer (Kuijer et al., 2000) or higher levels of stress (Coyne & Smith, 1991). Relationship-focused support may have a positive impact for couples coping with some types of cancer, but these styles may be less effective for couples facing other types of cancer-related stressors. For example, focusing on symptoms has been found to be a maladaptive approach in women who are receiving treatment for early-stage breast cancer (Ransom et al., 2005); on the other hand, spotting suspicious-looking skin spots by one’s partner is critical for early detection of skin cancer. While the nuances of relationship-focused support in the context of skin cancer may align with studies of other types of cancer, it is important to acknowledge that studies on relationship-focused support in couples facing other types of cancer may not capture the nuances of the lived experience of facing skin cancer. The current study helps fill this gap in the literature. If the previous findings hold true in the examination of relationship-focused support use when facing skin cancer, active engagement support—a style that involves facing the stressor directly and working together to solve problems—should be more beneficial than protective buffering and overprotection, which include avoidance and denial.
Quality of Life
Several studies have examined psychological distress and QOL after being diagnosed with skin cancer. These studies have found contradictory findings. For example, in a study of 178 individuals with stage 0–III melanoma, individuals who reported high levels of distress over the melanoma were likely to experience poor QOL (Trask et al., 2001). Other studies have found that QOL of the individual with skin cancer may not be negatively impacted. For example, Schlesinger-Raab et al. (2010) found that 2 years posttreatment for malignant melanoma, participant QOL scores were similar to scores from the general population. About half of the study participants reported that their attitudes toward life had changed for the better since the melanoma diagnosis. One explanation may be that QOL had returned to normal levels in 2 years between the treatment ending and the study beginning. Beutel et al. (2015) also did not find poorer QOL in their study of 683 individuals with melanoma, but it had been an average of 8.41 years since participants had been diagnosed, so they too may have recovered from any negative QOL impacts from the melanoma.
The current study addresses some of the limitations of past research on QOL and skin cancer. Rather than focusing only on the QOL of the person with skin cancer, which neglects half of a two-person equation, this study examines QOL of both partners. As cancer affects many people in the surrounding network, especially romantic partners, it is important for researchers to examine the QOL of both members of a couple, emphasizing how partners may affect one another. There may be implications for both HPs and couples if QOL of the HPs is also impacted by skin cancer. For example, poor QOL of HPs may be associated with other negative outcomes such as higher HP anxiety. Additionally, poorer QOL may be linked to lower relationship satisfaction, which can individually affect each partner. The current study addresses the gap in understanding about HPs’ QOL, setting a foundation for future work that could examine personal and couple implications.
Purpose
The primary aim of this study was to examine the role of relationship-focused support to promote the QOL in partners coping with skin cancer. We hypothesized that support received by each partner would affect their QOL (“actor effects”) as well as their partner’s QOL (“partner effects”), controlling for the characteristics of skin cancer, namely, type of diagnosed skin cancer, stage of the skin cancer, and sex of the partner with the diagnosis. The specific research question and hypotheses for each of the three types of relationship-focused support were as follows:
Methods
Participants
Thirty couples in which one partner had received a skin cancer diagnosis in the previous 2 years participated in this study. Couples were recruited between July and December 2017. Inclusion criteria were (a) diagnosis of skin cancer (melanoma, basal cell carcinoma [BCC], squamous cell carcinoma [SCC], or other) in stages 0–III; (b) age 60 or older; (c) ability to read and write in English; (d) married or in a committed romantic relationship for a minimum of 5 years and living together with the partner; and (e) both partners willing to participate in the study. The exclusion criteria were (a) either partner was currently receiving treatment for any other form of cancer that was not skin cancer; (b) skin cancer in stage IV; (c) couples where the skin cancer diagnosis had occurred more than 2 years prior; (d) couples who had been partnered fewer than 5 years; and (e) another chronic health condition besides the skin cancer in either partner that was not successfully controlled by medication or another form of treatment. Twenty-two couples completed surveys on paper, while eight couples completed the surveys online via Qualtrics.
Procedures
Approval for this study was obtained from Virginia Tech’s Institutional Review Board. Survey questionnaires were available either as pen-and-paper surveys or online via Qualtrics. After giving informed consent, both partners in each couple were instructed to complete survey measures independently from one another on the appraisal of the skin cancer diagnosis, their perception of the type of support they received from their partner, and QOL. Following the completion of the survey, participants could choose to be entered into a random drawing for one of four $25 Amazon gift cards. Couples who completed the survey questionnaires as pen-and-paper surveys mailed the surveys back to the primary researcher in separate envelopes to help provide confidentiality to both partners. Twenty-two couples completed pen-and-paper surveys, and eight couples completed the online survey. There were no differences in demographics, received relationship-focused support, and QOL between couples who completed the pen-and-paper surveys and those who completed the online surveys.
Measures
All participants answered demographic questions including age, sex, race and ethnicity, length of the current partnership, and presence of common health conditions. Additionally, PwSCs answered questions that were used as control variables in the study analyses. Specifically, the control variables were PwSC sex (0 = male; 1 = female), the type of skin cancer diagnosis (melanoma = 0; nonmelanoma [BCC and SCC] = 1), and skin cancer stage (early stage [stage I] = 0; midstage [stages II–III] = 1).
Perception of Relationship-Focused Support Received From Partner
The current study utilized a questionnaire developed by Buunk et al. (1996) to measure three styles of relationship-focused support: active engagement (e.g., “When something bothers me, my partner tries to discuss the problem.”), protective buffering (e.g., “My partner tries to act as if nothing is the matter.”), and overprotection (e.g., “My partner continuously keeps an eye on me.”). The version for the PwSC diagnosis included 19 items asking to what extent they perceived their HP had adopted the three styles of providing support to them. Perceived active engagement support was measured via five items, rated on 5-point Likert-type scales (α = .70). Protective buffering support was captured by eight items (α = .74). The overprotection subscale, which was completed only by the partners with skin cancer, included six items (α = .83). PwSCs rated each of the 19 items on a 5-point Likert-type scale, with responses ranging from 1 (Never) to 5 (Very often). Items on the active engagement, protective buffering, and overprotection subscales were averaged to create three subscale scores. Higher subscale scores indicate higher perceived receipt of the particular relationship-focused support from their partner.
HPs completed an 11-item version of this scale to rate the extent to which they perceived their PwSCs provided support as active engagement (five items; α = .69) and protective buffering (six items; α = .79). Each of the 11 items was rated on a 5-point Likert-type scale. Responses ranged from 1 (Never) to 5 (Very often). To capture each style of support received by the PwSC, items on the active engagement and protective buffering subscales were averaged to create two scores. Higher average scores indicated higher perceived receipt of the particular style of support. The questionnaire completed by HPs was shorter in length because overprotection was not included as a style of support used by the PwSCs.
Quality of Life
Both partners completed the World Health Organization Quality of Life-Brief (WHOQOL-BREF) measure, which is a 26-item scale revised from the original 100-item World Health Organization Quality of Life measure (WHOQOL Group, 1998). The WHOQOL-BREF evaluates the four domains of physical health, psychological health, social relationships, and environment. Elements within the physical health domain, which is measured via seven items, include activities of daily living, energy and fatigue, pain and discomfort, and sleep and rest. The 6-item psychological domain includes items about negative and positive feelings, self-esteem, and spirituality and religion. The third domain, social relationships, focuses on personal relationships, social support, and sexual activity, and is measured through three items. Finally, the eight-item environment domain includes items about financial resources, home environment, leisure activities, and the physical environment. Participants were instructed to think about their lives over the past two weeks and respond to questions based on their thoughts and feelings during this time span, with responses ranging from 1 to 5. Response ratings varied based on wording for individual items. For example, responses for “How much do you enjoy life?” ranged from 1 (Not at all) to 5 (An extreme amount); responses for “To what extent do you have the opportunity for leisure activities?” ranged from 1 (Not at all) to 5 (Completely); responses for “How satisfied are you with the support you get from your friends?” ranged from 1 (Very dissatisfied) to 5 (Very satisfied); and “How often do you have negative feelings such as blue mood, despair, anxiety, depression?” ranged from 1 (Never) to 5 (Always). Participants also responded to two additional items: “How would you rate your quality of life?” with responses from 1 (Very poor) to 5 (Very good), and “How satisfied are you with your health?” rated with responses from 1 (Very dissatisfied) to 5 (Very satisfied).
Individual items from each domain were averaged to calculate the domain score. Next, domain scores were multiplied by four, so they were comparable to scores used in the original 100-item measure, per scoring guidelines for the WHOQOL-BREF (WHOQOL Group, 1998). The four domains were scored such that higher domain scores indicated higher QOL on the specific domain. A summed total QOL score was created using the four separate domain scores, one item on overall QOL (e.g., “How would you rate your quality of life?”) and one item on general health (e.g., “How satisfied are you with your health?”). Potential overall QOL scores could range from 6 to 100, with higher scores capturing higher QOL. Overall QOL demonstrated good reliability (PwSC QOL α = .86; HP QOL α = .84).
Analytical Plan
Statistical analyses were performed using SPSS version 24 (SPSS Inc., Chicago, IL, United States) and MPlus version 8 (Muthén & Muthén, Los Angeles, CA, United States). Multivariate actor–partner interdependence models (APIMs) examined associations between partners’ perceptions of received support and their own QOL (actor effects) and associations of perceived support with their partners’ QOL (partner effects), accounting for the nonindependence of the couple data. Three APIMs were run separately to assess the association between each type of support (i.e., active engagement, protective buffering, and overprotection) and QOL while controlling for PwSC sex, type of skin cancer, and skin cancer stage. An a priori p-value of <.05 was considered statistically significant. Fit indices (χ², Confirmatory Fit Index [CFI], and Standardized Root Mean Square Residual [SRMR]) are reported for the results of the three models.
Results
Descriptive Analyses
Descriptive characteristics of the study sample are presented in Table 1. The mean age for PwSCs was 69.97 years (SD = 7.79), with a range of 60–88 years. The mean age for HPs was 70.10 years (SD = 6.80), with a range of 60–87 years. Partners had been together for an average of 38 years (range 10–60 years). All HPs reported their race as White/Caucasian (n = 30), mostly not Hispanic or Latino, whereas 28 PwSCs reported their race as White/Caucasian, again mostly not Hispanic or Latino, one indicated race as American Indian or Alaska Native, and one as Asian. The majority of PwSCs were women (n = 20, 67%) in comparison to men (n = 10, 33%). Seven PwSCs (23%) and seven HPs (23%) completed 11–15 years of education, 17 PwSCs (57%) and 15 HPs (50%) completed 16–18 years of education, and six PwSCs (20%) and 8 HPs (27%) reported completing 19 or more years of education. Thirteen PwSCs (43%) and 14 HPs (47%) were currently employed, 12 PwSCs (40%) and 15 HPs (50%) were not currently employed, and five PwSCs (17%) and one HP (3%) had never been employed outside of the home. Fourteen PwSCs (47%) reported a melanoma diagnosis, 11 reported a BCC diagnosis (37%), and five reported a SCC diagnosis (16%). More PwSCs had stage I cancers (n = 13, 43%) and stage II cancers (n = 12, 40%) than stage III cancers (n = 5, 17%). PwSCs reported an average of 10.90 months since receiving the skin cancer diagnosis (R = 2–20 months, SD = 5.10). A significant difference (t(29) = −2.28, p = .03) was found between QOL of PwSCs (M = 97.06, SD = 11.44) and HPs QOL (M = 101.76, SD = 10.96). Correlations between study variables are provided in Appendix A.
Demographic Characteristics of PwSCs and HPs.
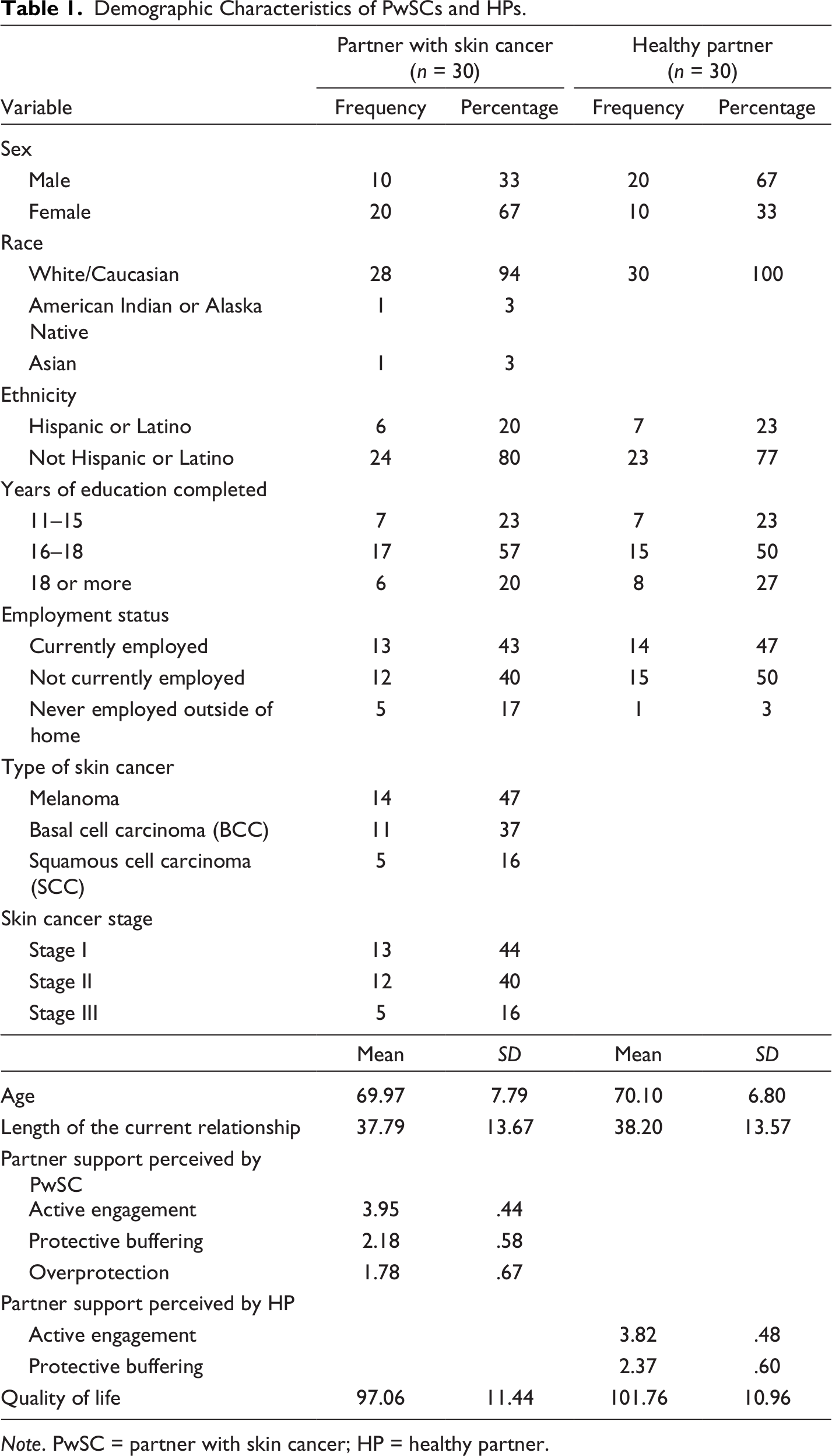
Note. PwSC = partner with skin cancer; HP = healthy partner.
Relationship-Focused Support and Quality of Life
Active Engagement Support and Quality of Life (Hypothesis 1a)
The APIM representing the relationships between active engagement support and QOL of both partners did not demonstrate significant actor or partner effects (Figure 1; χ²(7) = 7.95, p = .33; CFI = .92; SRMR = .08). Specifically, support in the form of active engagement perceived by PwSCs was associated with neither their own QOL (actor effect; β = .26, p = .12) nor their partner’s QOL (partner effects; β = .18, p = .33). Similarly, active engagement support perceived by the HPs was not associated with their own QOL (actor effect; β = .11, p = .53) or with the PwSC QOL (partner effect; β = .00, p = .99). HPs reported lower active engagement from female PwSCs (β = −.09, p = .05).
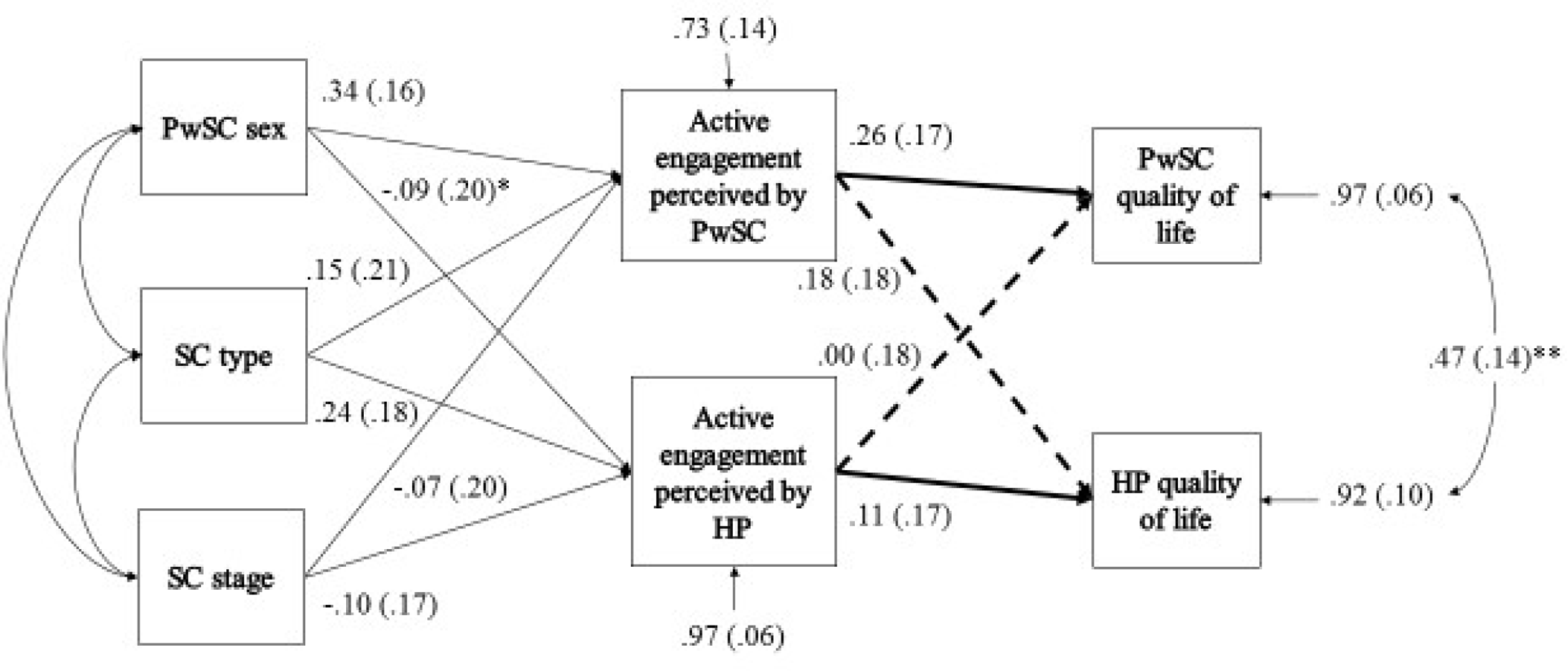
APIM of the associations between active engagement and QOL. Note. PwSC = partner with skin cancer; HP = healthy partner. APIM = actor–partner interdependence model.
Protective Buffering Support and Quality of Life (Hypothesis 1b)
The APIM representing the relationships between protective buffering support perceived by both partners and QOL of PwSCs and HPs demonstrated significant actor and partner effects (Figure 2). The fit of this model was less optimal, but adequate (χ²(7) = 10.83, p = .15; CFI = .92; SRMR = .09). Specifically, protective buffering support perceived by PwSCs was not associated with their own QOL (actor effect; β = −.30, p = .09) or with their partners’ QOL (partner effect; β = −.05, p = .79). In contrast, protective buffering perceived by HPs was associated with their own QOL (actor effect; β = −.37, p = .05) and associated with their partner’s QOL (partner effect; β = −.43, p = .01). With regard to the control variables, HPs reported perceiving greater protective buffering when their PwSCs was female and when the skin cancer was in midstage. PwSCs also reported perceiving more protective buffering from their HPs when they had melanoma skin cancer.
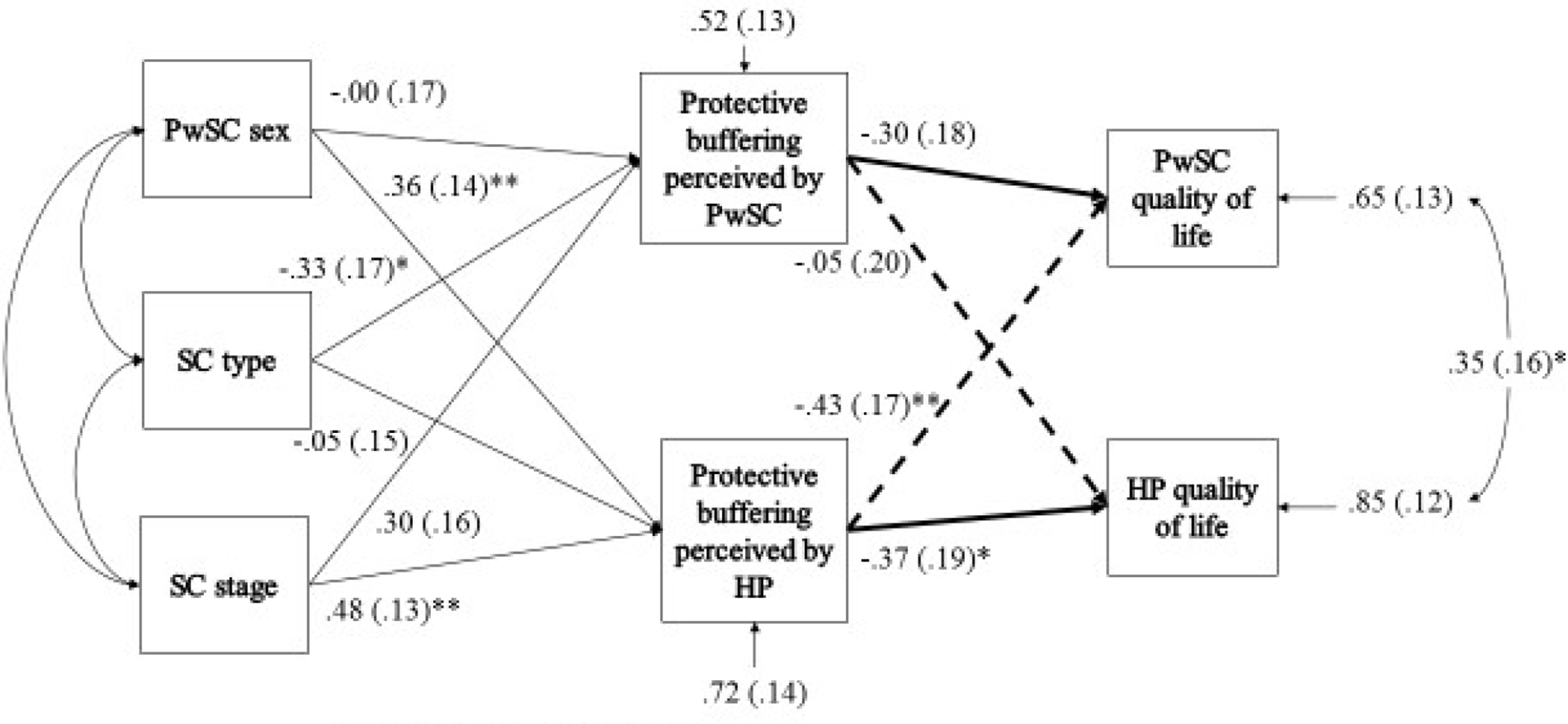
APIM of the associations between protective buffering and QOL. Note. PwSC = partner with skin cancer; HP = healthy partner. APIM = actor–partner interdependence model.
Overprotection Support and Quality of Life (Hypothesis 1c)
The APIM representing the relationships between overprotection perceived by the PwSCs and QOL of both partners demonstrated a significant actor effect, but no partner effect (Figure 3; χ²(6) = 3.04, p = .08; CFI = 1.00; SRMR = .05). Specifically, overprotection perceived by the PwSCs was significantly associated with their own QOL (actor effect; β = −.63, p < .001). However, overprotection was not associated with HPs’ QOL (partner effect; β = −.25, p = .14).
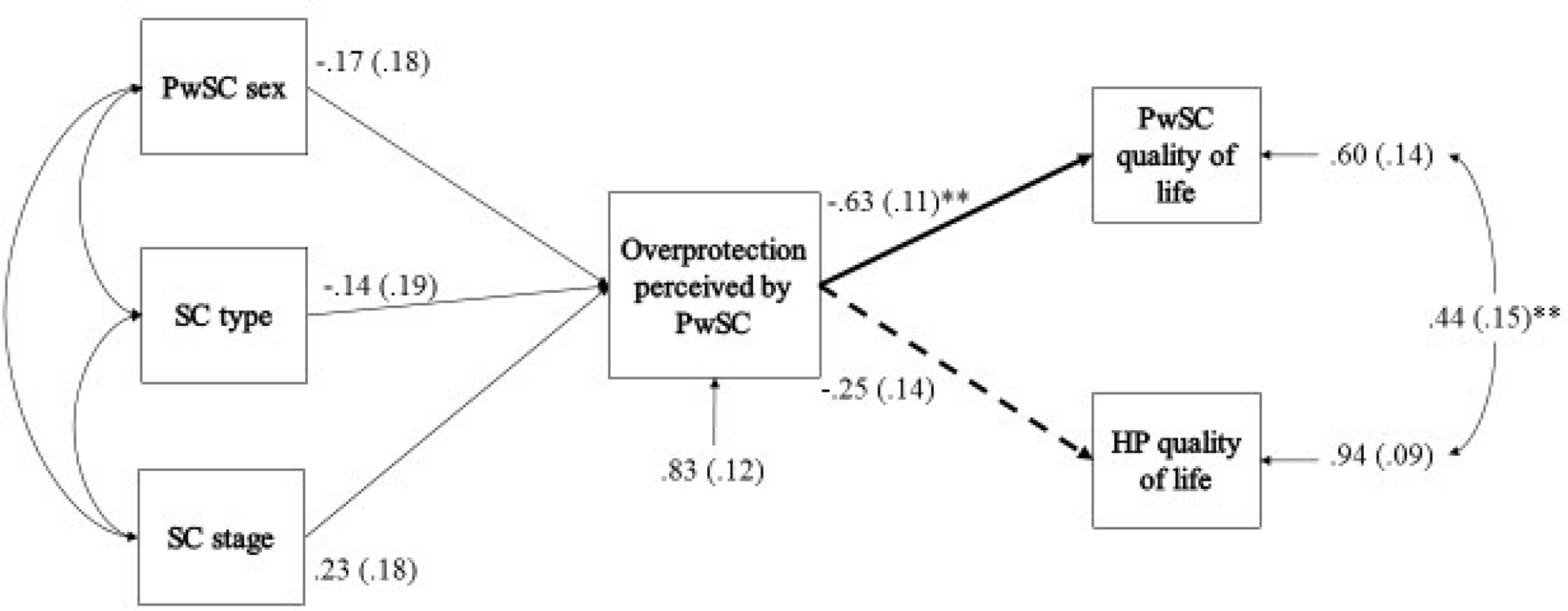
APIM of the association between overprotection and QOL. Note. PwSC = partner with skin cancer; HP = healthy partner. APIM = actor–partner interdependence model.
Discussion
The current study examined both partners’ use of relationship-focused support and its associations with their own QOL and their partners’ QOL. Overall, this study found that protective buffering support provided by PwSCs was associated with lower QOL of both partners. HPs’ overprotection also was associated with lower QOL for PwSCs. However, contrary to the previous research (Banovcinova & Baskova, 2016; Leung et al., 2014), in this study, active engagement support provided by either partner was not associated with QOL.
Protective buffering perceived by HPs (and provided by PwSCs) was associated with poorer QOL of both partners. This finding extends the previous research that has documented the negative associations between protective buffering and couple outcomes such as relationship satisfaction (Schokker et al., 2010). When PwSCs hides cancer-related thoughts and concerns to protect their partner, it may affect how they cope with their illness. When HPs knows that their PwSCs are avoiding discussions about cancer, they may experience emotional distance. Similarly, HPs may want to have more conversations about the diagnosis but feel hesitant to engage with the PwSCs (Venetis et al., 2014). There may also be instances where HPs express their worries, but the PwSC have trouble handling those concerns, so they act as if they do not notice (Badr & Taylor, 2006). As a result, HPs may be even more hesitant to talk about cancer in the future. PwSCs may perceive distance or apprehension in the HPs, potentially without being aware that the avoidance of skin cancer is the driving force behind the discord. In these instances, the QOL of both partners may be negatively affected.
HPs may provide less support because they are unaware of the stress or worries that the PwSCs is hiding, which could contribute to hurt feelings within the relationship (Manne et al., 1999). PwSCs may also hide information about the skin cancer, such as treatment concerns or prognosis details received from doctors (Porter et al., 2005) if they feel their HPs are not concerned about the skin cancer. Additionally, if HPs appear to be disengaged with the skin cancer-related stress because they are unaware of the PwSCs’ support needs, PwSC may try to cope by themselves (Burri et al., 2017) or they may experience feelings of resentment or loneliness. Similarly, hiding thoughts and concerns may also affect how the HP copes with skin cancer. HPs may ruminate over their concerns but not find relief from sharing these with their partners (Badr & Taylor, 2006). Hiding concerns could also lead to bitterness and hostility within the couple relationship (Langer et al., 2009). In summary, our study suggests that when the PwSC does not want to talk about skin cancer, the QOL of both partners is affected.
It is also possible that avoidance of the topic of skin cancer may be a beneficial coping mechanism for some. Perhaps the use of protective buffering support can offer some stress relief to the PwSC; not talking about skin cancer-related stressors may allow the partners to focus on positive thinking (Badr & Taylor, 2006). Also, efforts made to prevent the HP from thinking about the diagnosis may be helpful in keeping him or her from becoming overwhelmed or may reduce anxiety or depressive thoughts and feelings. In these instances, the use of protective buffering support may be a constructive coping strategy for the HP, and therefore, not associated with poorer QOL.
Overprotection perceived by PwSCs was associated with lower QOL for PwSCs. Perceiving support such as unnecessary praise or being constantly monitored is likely to impact the PwSC’s self-confidence and sense of autonomy (Buunk et al., 1996) or undermine his or her sense of control (Coyne & Smith, 1994), which may then negatively impact his or her QOL. Similarly, when HPs unnecessarily take over chores from PwSCs, they may lose previously held roles or responsibilities within the family, which can cause an upset in the family homeostasis. The heightened level of monitoring and control exhibited by overprotective support (i.e., constant monitoring to ensure the PwSC follows doctor’s instructions) has the potential to change the dynamics of the partner relationship to one of unequal power, such that the PwSC feels a sense of loss over what the partnership used to be. These findings are novel in skin cancer literature, as they contribute deeper understanding than an examination of either partner in isolation would provide, showing how using a dyadic focus can move the literature on skin cancer in older adults forward.
Contrary to the previous studies (Hagedoorn et al., 2011; Schokker et al., 2010), we did not find a significant association between active engagement support perceived by PwSCs and HPs and the QOL of either partner. One possibility is that active engagement may be more important for couples facing late-stage skin cancer. As couples face more advanced stages of skin cancer, which requires more invasive treatment and has poorer prognoses, open discussions about the prognosis may be beneficial for both partners. As no couples in this study were facing late-stage skin cancer, future studies could evaluate these associations by focusing on stage IV. Additionally, it is important to highlight the relevance of the broader context in which couples in this study enacted their support. While the current study directed couples to focus on relationship-focused support within the context of the skin cancer diagnosis, couples would have still been facing other daily secondary stressors which would necessitate support (e.g., financial difficulties, issues with other family members, and work-related incidents; Savla et al., 2011). It may be that significant associations between active engagement and QOL may be dependent on an examination of the variety of other secondary stressors that couples were concurrently experiencing.
Overall, findings from this study emphasize that support provided by both PwSCs and HPs appears to be important for couples, confirming that skin cancer is a couple’s stressor. Health care providers and mental health professionals can use these findings to inform work with couples facing skin cancer. Providers can help increase couples’ awareness of the associations between the support they provide and their QOL, while also engaging in discussions about how partners can improve the support they give. Psychoeducational programs and support groups could focus on helping partners learn about the benefits of using different types of support when their needs are different. While partners could work on increasing active engagement support, they could also learn to identify when protective buffering support might be beneficial. Additionally, as protective buffering intrinsically involves avoiding discussions about skin cancer, partners could work on openly discussing their support needs to help one another, including discussions when support needs change or when the previously used support is no longer beneficial. Providers could also help HPs learn to identify instances when they use overprotection that may not be appreciated or welcomed by the partner with skin cancer. These findings of our study also have implications for couples facing a variety of other diagnoses or stressful life events; understanding the impact that protective buffering and overprotection support have on QOL can inform work with couples facing other stressors, who may experience similar challenges.
Limitations
The findings of this study must be considered in light of their limitations. First, the relatively small sample size limits the complexity of potential analyses, as well as the generalizability of the findings. Thus, although the study findings should be interpreted with caution, they provide an important first step in examining a complex life experience that many older couples may face. Second, as a cross-sectional study, causal effects between the study variables cannot be implied. Nevertheless, by establishing that some types of support are associated with partners’ QOL, the current study creates a foundation for future longitudinal work to examine whether and how the effects of support change over time. There is also room for a deeper understanding of the relationships between characteristics of the skin cancer diagnosis, support perceived by each partner, and QOL. Other variables, such as relationship satisfaction, were not included in this study. Future research should consider such variables that provide relationship context and history from which interpretations about the current quality of support can be judged. Finally, relationship-focused support does not capture all the support that couples receive. For example, partners may have also been receiving support from adult children, friends, or other family members, which likely is associated with their QOL but not examined in the current study. Despite these limitations, the current study demonstrates that relationship-focused support partners perceive is associated with their own QOL and their partners’ QOL.
In summary, older couples use a variety of styles of support when facing a skin cancer diagnosis of one partner. Partners’ support does appear to have some associations with QOL of both partners, but not uniformly. Active engagement support does not appear to be associated with QOL. Protective buffering and overprotection support, on the other hand, may contribute to low QOL for partners in some instances. As longevity continues to increase, older couples will face chronic health conditions together. How partners support one another and how they cope with an illness has implications for partners’ relationship satisfaction, emotional well-being, QOL, and overall health. Overall, the current study demonstrates the importance of paying attention to how partners face skin cancer together.
Footnotes
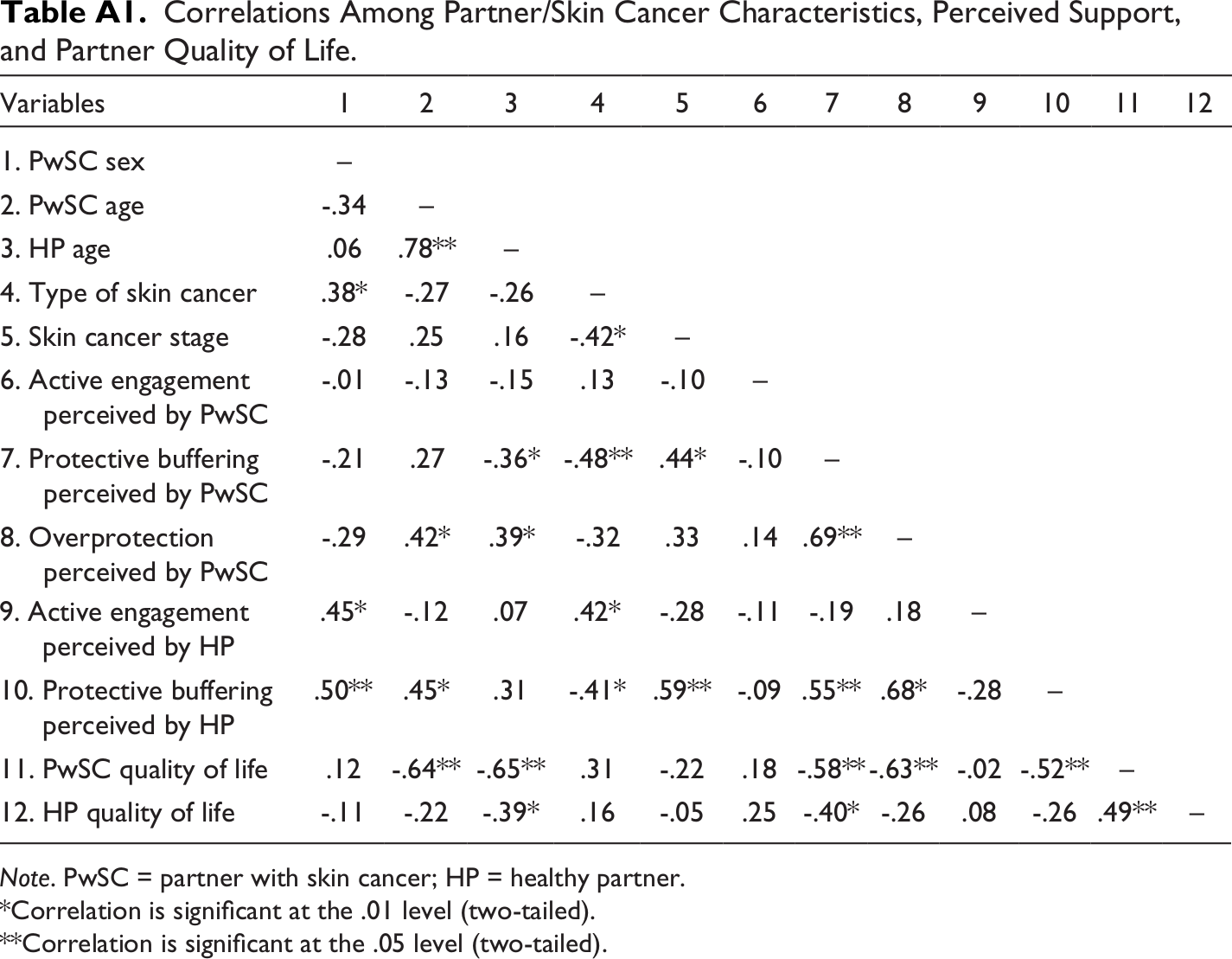
Appendix A
Correlations Among Partner/Skin Cancer Characteristics, Perceived Support, and Partner Quality of Life.
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. PwSC sex | – | |||||||||||
| 2. PwSC age | -.34 | – | ||||||||||
| 3. HP age | .06 | .78** | – | |||||||||
| 4. Type of skin cancer | .38* | -.27 | -.26 | – | ||||||||
| 5. Skin cancer stage | -.28 | .25 | .16 | -.42* | – | |||||||
| 6. Active engagement perceived by PwSC | -.01 | -.13 | -.15 | .13 | -.10 | – | ||||||
| 7. Protective buffering perceived by PwSC | -.21 | .27 | -.36* | -.48** | .44* | -.10 | – | |||||
| 8. Overprotection perceived by PwSC | -.29 | .42* | .39* | -.32 | .33 | .14 | .69** | – | ||||
| 9. Active engagement perceived by HP | .45* | -.12 | .07 | .42* | -.28 | -.11 | -.19 | .18 | – | |||
| 10. Protective buffering perceived by HP | .50** | .45* | .31 | -.41* | .59** | -.09 | .55** | .68* | -.28 | – | ||
| 11. PwSC quality of life | .12 | -.64** | -.65** | .31 | -.22 | .18 | -.58** | -.63** | -.02 | -.52** | – | |
| 12. HP quality of life | -.11 | -.22 | -.39* | .16 | -.05 | .25 | -.40* | -.26 | .08 | -.26 | .49** | – |
Note. PwSC = partner with skin cancer; HP = healthy partner.
*Correlation is significant at the .01 level (two-tailed).
**Correlation is significant at the .05 level (two-tailed).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies