
Abstract
Persons with dementia (PWD) benefit from participating in meaningful activities. This study’s objective was to learn the characteristics of successful meaningful activities from community-based service providers who work with PWD. Six group interviews were performed with 15 unique professionals from an adult day service or community-based coordinated care program. These were supplemented by 100 hr of researcher immersion through weekly volunteering. Data were analyzed by a team, using qualitative content analysis. Participants reported successful activity content incorporated personalization; continuity and incremental challenges; and social engagement. Successful delivery of activities required managing necessary resources; involving informal (family/friend) caregivers; having a backup plan; monitoring time of day and energy levels; facilitating a domino effect; and ensuring safety. Outcomes of successful activities were experiencing fulfillment and purpose; overcoming challenges; and unexpected triggers. Research and practice recommendations include testing innovative, dynamic, and technology-enabled approaches to providing such activities.
Keywords
Introduction
Due to global population aging, the number of persons with age-related health conditions, including dementia, is expected to double by 2030 (Alzheimer’s Association, 2019; Borson et al., 2016; Prince et al., 2016), with accompanying increases in social, medical, and financial demands (Alzheimer’s Association, 2015; Borson et al., 2016; Hebert et al., 2013). A significant need for persons with dementia (PWD) is participating in stimulating and meaningful activities (Miranda-Castillo et al., 2013; Nyman & Szymczynska, 2016). Studies show fulfilling the need for such activities for PWD can improve quality of life (Gitlin et al., 2016; Nyman & Szymczynska, 2016; Phinney et al., 2007), reduce anxiety and agitated behaviors (Cohen-Mansfield et al., 2015, 2017; Han et al., 2016), improve clinical and social outcomes (Kolanowski et al., 2006; Nyman & Szymczynska, 2016), stimulate feelings of individuality and autonomy (Kolanowski et al., 2006; Phinney et al., 2007), and improve relationships with others (Gitlin et al., 2016; Kolanowski et al., 2006; Vernooij-Dassen, 2007). In contrast, a lack of activity opportunities or not being able to engage in them effectively is associated with neuropsychiatric symptoms such as withdrawal, inactivity, passivity, agitation, depression, and worse quality of life and health (Harmer & Orrell, 2008; Miranda-Castillo et al., 2013; Nyman & Szymczynska, 2016; Phinney et al., 2007). Consequently, milestones for the United States (US) National Plan to Address Alzheimer’s Disease include funding to “develop and scale-up innovative and low-cost evidence-based purposeful living activities for individuals with cognitive impairment that will also provide respite for key family and friend caregivers” (Borson et al., 2016, p. 362).
Despite the recognized importance of activities for PWD and accumulating knowledge of PWD and family caregiver perceptions of activities (e.g., Harmer & Orrell, 2008; Menne et al., 2012), there is additional value to understanding what makes for a successful activity (Cohen-Mansfield et al., 2015; Kolanowski et al., 2008; Lu et al., 2016). Service providers who recommend, deliver, or otherwise support activities may have unique and important insights into the elements of activity content, delivery, and outcomes that make them successful or not.
Activity content refers to the type of activity and its difficulty and complexity, relative to the abilities of the PWD (Lu et al., 2016; Regier et al., 2017). One way to evaluate content is to assess how well it matches PWDs’ interests and preferences (Gitlin et al., 2016; Menne et al., 2012; Regier et al., 2017) or self-identity (Harmer & Orrell, 2008). Successful delivery of activities refers to the approach or strategies used to present the activity and engage participants. For example, one popular strategy in the literature is tailoring the activity to the individual to accommodate not only limitations but also their abilities and preferences (Gitlin et al., 2016). A tailored activity for someone who likes physical activity but cannot remember multiple steps might be washing windows or winding yarn (Gitlin et al., 2009). Tailoring to what a person can and wants to do is a hallmark of the strengths-based approach used in psychology, social work, occupational therapy, and other fields (McGovern, 2015). Another delivery strategy described in the literature is inserting periodic check-ins and adjusting activities over time to address emergent barriers to engagement (Gitlin et al., 2008; Lu et al., 2016). Lastly, successful activities might be defined as ones achieving positive outcomes such as clinical improvement, social engagement, sense of autonomy, or belonging, and preventing undesirable outcomes such as withdrawal, disengagement, or various neuropsychiatric symptoms associated with dementia (Han et al., 2016; Miranda-Castillo et al., 2013; Phinney et al., 2007; Volicer et al., 2006).
Prior studies to establish the characteristics of activities have been based on trials of intervention efficacy, showing, for example, that tailoring results in better outcomes compared to nontailored programs (Trahan et al., 2014). In addition, studies have interviewed PWD and informal caregivers of PWD to understand their perspectives on what makes activities meaningful or enjoyable (Han et al., 2016; Harmer & Orrell, 2008; Menne et al., 2012; Phinney et al., 2007). In the present study, we add to the literature on “what makes activities for PWD successful” by investigating the experiences and perceptions of community-based service providers.
The present study’s objective was to learn the content, delivery, and outcome characteristics of successful activities from the perspectives of individuals who work with PWD in community-based service settings. As part of a larger project to develop a new activity intervention, we performed six group interviews with nine individuals working or volunteering at an adult day service and six nursing and social work staff from a community-based coordinated care program.
Methods
Design
From October to November 2016, the researchers performed six group interviews with 15 unique professionals working with PWD, many of whom participated in multiple interviews. In parallel, during a 3-month period, the researchers performed 100 hr of immersion as activity volunteers at an adult day service facility. Interview data were analyzed qualitatively for themes regarding the content, delivery, and outcomes of successful activities, as defined by the service providers. Interview data were collected with verbal informed consent, as approved by the Indiana University Institutional Review Board. Human subjects data were not collected during immersion activities; instead, researchers documented their personal reflections in research memos.
Settings and Participants
Participants were paid staff and volunteers from two organizations providing services to PWD: Joy’s House adult day service and the Aging Brain Care (ABC) clinical program. Joy’s House is an Indianapolis-based not-for-profit organization providing weekday adult day services including activity programming to individuals with life-altering conditions. Approximately 70% of individuals attending Joy’s House are diagnosed with dementia. Services cost $75/day, with financial assistance available based on need. The ABC program is a combination ambulatory memory clinic and community-based coordinated care program for older adults with cognitive impairment. The care coordinators and their assistants in this program work with PWD and their informal caregivers to manage the physical and mental health of both. This includes making recommendations for engagement in social and meaningful activities as well as helping secure resources to facilitate activity engagement. This community-based program is embedded in a large Indianapolis-based safety net community health system, Eskenazi Health, and serves a vulnerable population, comprised of 60% Black/African American PWD and 30% with <12 years of education. Both organizations serve a racially and socioeconomically diverse clientele.
Of the 15 total participants, nine were employees (n = 8) or long-time activity volunteers (n = 1) at Joy’s House . These participants’ roles spanned activity development, activity facilitation, and management. All had experience directly engaging PWD in various planned activities. The other six participants were employees at the ABC program, representing a mix of registered nurses, social workers or social work trainees, and community health workers who routinely worked with community-dwelling PWD. They recommended and monitored, but did not directly facilitate, participation in planned and unplanned activities.
For both participant groups, individuals self-enrolled in the study with support from organizational leadership. A mean of 4 ± 1.4 individuals participated in each group interview session. Group interviews took place during work hours in a conference room in the participants’ respective facilities. Participants received no incentives or compensation for study participation.
Procedures
Group Interviews
The group interviews consisted of three interview sessions with each group of participants (for a total of six), each session focusing on one aspect of activities for PWD: activity content; delivering activities, including strategies and challenges; and outcomes of PWD participating in activities (see Appendix for the session guide). In the second session, participants also marked which activities they would give a “High” or “Low” recommendation on a list of activities generated from the first session. At the end of the third interview, participants engaged in whole-group brainstorming about specific new activity interventions, as the ultimate goal of the project was to create a new intervention. The group interviews followed a semistructured protocol using prepared topics and scripted probes to initiate discussion, with facilitation and encouragement to participants to contribute openly and build on each other’s comments. Slight variations to topics and probes were made to accommodate differences between participants in the two settings, for example, asking the clinician group to discuss how cost played a role in PWDs’ ability to engage in activities. Participants were asked to answer the questions and share their own experiences, focusing on activities for older adults with mild or moderate dementia.
Group interview sessions were deliberately planned such that on each interview day, one participant group was interviewed in the morning and the other was interviewed about the same topic in the afternoon, with counterbalancing of groups. This allowed the team to develop additional probes or discussion topics based on interviews earlier in the day. Researchers also prepared for each subsequent topic session by reviewing notes from prior sessions.
Two researchers, a human factors engineer/psychologist (RJH) and a human-centered computing doctoral student (LC), facilitated the sessions with the aid of one observer and one note taker. The facilitators used a whiteboard, drawings, and printouts as visual aids to stimulate conversation and confirm understanding. Group interviews lasted 60–90 min and were audio- and video-recorded.
Immersion
The research team participated in 100 hr (average of 25 hr per person) of immersion in the form of weekly volunteering at Joy’s House adult day service facility. Immersion included participating in activities organized by Joy’s House staff as well as planning and leading new activities. Example activities were mask painting, Halloween decorations, group reading, social conversations, group exercise, table games, and crafting musical instruments. Researchers recorded self-reflective memos and discussed their experiences with one another to gain and share personal insights into activities for PWD. These immersive experiences helped provide context for understanding interview findings and contributed to the development of interview probes.
Analysis
We adopted a direct content analysis approach (Hsieh & Shannon, 2005) in a team-based qualitative data analysis framework (Guest & MacQueen, 2008). A team of three primary analysts (LC, TP, SV), all involved in data collection, performed the analysis with a senior researcher (RJH) intermittently examining the analysis and providing supervisory feedback. The analysis process was done in three phases. In phase 1, members of the analysis team independently assigned multi-paragraph sections from group interview transcripts to three predetermined major categories (Content, Delivery, Outcomes). When the content of a section pertained to multiple categories, the section was coded in each. In phase 2, the team met regularly for in-person whole-team analysis sessions, during which they suggested and agreed upon an initial set of nonoverlapping subcategories developed inductively from the data. Prior to these group analysis meetings, all analysts prepared by reading transcripts and reviewing audio or video recordings. All analysts thus suggested coding subcategories, gave examples from the interviews to illustrate subcategories, and audited each other’s suggested subcategories, to develop a team-generated code book (MacQueen et al., 2008). These meetings provided not only analytic convergence among the team but also what Barry et al. (1999, p. 33) called “a training ground for the mindset” of the primary analyst, who performed the actual coding of data into subcategories between group meetings. Over time, the coding discussions produced a final set of 47 subcategories. In phase 3, the primary analyst reviewed the subcategories and coded data in themes, or cohesive “patterns in the data” describing the most salient aspects of the phenomenon in question (Braun & Clarke, 2006). This resulted in 12 themes, each presented in the results within the broader categories of Content, Delivery, and Outcomes.
Results
Most participants were female (14, 93%) and ages varied: 25–34 years (3, 22%), 35–44 years (5, 34%), 45–54 years (3, 22%), 55–64 years (3, 22%). Their experience working with PWD ranged from 6 months to 12 years, with seven (43%) reporting having 3–10 years’ experience. They spent a mean of 88 hr per month working with PWD (range, 12–150).
Content
In the first group interview session, participants mentioned 54 unique activities, listed by category in Table 1. Nine participants marked activities they would “highly” recommend. The activities most likely to be highly recommended were those that could be performed individually and with low-cost equipment, such as listening to music, painting and drawing, walking, stretching, and reading. There were several highly recommended social activities, ranging in amount of planning and organizing required, but often placing little burden on the participant, for example, playing bingo, talking to others, pet therapy, or attending meeting and events. Several activities were pro-social and more complex, such as volunteering, coaching sports, teaching, caregiving for others, and neighborhood watch, but these tended to not be highly recommended.
Fifty-Four Group and Individual Meaningful Activities Suggested by Participants, by Category, and Frequency With Which They Were Highly Recommended for Persons With Mild or Moderate Dementia.

Across the participant groups, three major themes emerged about the characteristics of successful activity content: personalizing activities; establishing continuity and incremental challenges; and incorporating social engagement.
Personalizing Activities to Individual Identities, Interests, and Abilities
Among all the factors mentioned that make an activity successful, the capacity to help PWDs relate to their past was the most prevalent. Participants reinforced the need to tailor activities to the identity and history of the PWD:
“Because they [the PWD] don’t feel forgotten… this is the question I ask the caregiver a lot, what did they do for a living? What was their role in the family?” Anna, Joy’s House
“One of my patients loved cars so I suggested him to help his son when he works on his car. He is only holding a lamp sometimes, [but that is still] something” John, ABC program
According to participants, choosing activities aligned with one’s identity can increase interest, engagement, and a sense of “ownership” of the activity. For instance, in a demonstration of taking ownership, an activity coordinator described how a group of women interested in cooking kept her accountable for a meal-related activity they were promised, even after several weeks had passed:
“I said I would buy some greens to prepare for lunch but totally forgot. Weeks later the three ladies … saw me and were saying ‘when are we preparing the greens? We should have those greens.’ I just ran out to buy some … [it] was a great activity helping to clean and prepare the food.” Tereza, Joy’s House
Participants stated that preferences for activities naturally varied and could be influenced by both interest and ability, requiring attention to both. For example, among a group of individuals, one subgroup might be personally interested in exercise, and a group exercise activity might permit standing and chair exercise as well as full-body and arms-only variants. Another subgroup might prefer reading and a reading activity could be developed with a variety of reading materials ranging in difficulty or topic.
Participants were in consensus that personalization unfolded as a dynamic process, as those who facilitate activities over time would: (a) learn about an individual’s background, interests, capabilities, and available resources; and (b) monitor for changes, such as reduced capabilities or new interests.
During immersion sessions, the research team observed the impact of matching the activity to a PWD’s identity. During a mask-painting activity, two individuals were highly interested and engaged, painting multiple masks and being present during the entire activity period, while others disengaged after their first mask. After the session, an activity coordinator explained one of the highly engaged individuals had been an arts and crafts teacher and the other came from a family of artists.
Establishing Continuity and Incremental Challenges
Participants reported successful activities were ones that over time could be performed continually and increased in complexity. Repetition was reported to both improve skills and establish routines and expectations:
“There’s good days and bad days, but the activity will come easier for them with repetition.” Meredith, ABC program
“They know that Friday we have Bingo and they prepare themselves for that.” Martha, Joy’s House
Participants noted the importance of gradually presenting “new challenges,” adopting activities with multiple levels of complexity, and allowing the activity leader to increase complexity according to the PWD’s progress and tolerance for additional challenge. For instance, after reading short texts from a newspaper for a week or two, the PWD may be ready to read a short book or book chapter. Participants differentiated this approach from using low-effort, passive activities that offered little challenge or growth, such as watching television. Participants also described situations where PWD abandoned an activity because it was no longer challenging:
“It is important to see if they [the patient] get something from the activity; can’t be too hard, but can’t be too easy either.” John, ABC program
On the other hand, participants cautioned about excessive difficulty or introducing a challenge too soon, thus bringing about perceived failure on the part of the PWD and resultant loss of self-confidence. They discussed the need for monitoring PWD for signs of dissatisfaction with the level of challenge.
Incorporating Social Engagement
Participants stated the ideal activity should provide the PWD an opportunity to engage and identify with both self and others. For example, participants described how a typically individual activity such as reading afforded social engagement when the reading was done in a communal circle; even being read to in this setting allowed a PWD to express themselves to others by commenting on the book. Similarly, reading to a grandchild could make an otherwise disinteresting reading activity more pleasant. Participants universally noted that certain activities can be among the most engaging and memorable precisely because of their social components:
“They love Bingo, it is like a party. We make sure everybody wins something, and they just play with each other, make jokes. It’s a good time for the group.” Helena, Joy’s House
The research team observed the value of social engagement during immersion sessions. In addition to the liveliness of social activities (e.g., community reading or exercise), PWD were described as particularly excited about individual arts and crafts activities when they were making objects meant for others’ enjoyment, such as Valentine’s Day cards.
Delivery
According to participants, successful delivery of meaningful activities required overcoming a number of barriers by implementing strategies related to activity planning and facilitation, namely: managing necessary resources; involving informal caregivers; having a backup plan; monitoring time of day and energy levels; facilitating a domino effect; and ensuring safety.
Managing Necessary Resources
Before an activity can be performed, necessary resources must be available or else provided, including both materials needed for the activity and the broader resources needed to access or engage in an activity, such as transportation or money:
“Some activities can be expensive. Sometimes I go to the patient’s house and they don’t even have a TV or even sound system.” John, ABC program
“If you tell them to go to the church but they can’t leave the house, they will only get frustrated.” Janet, ABC program
Some activity-related barriers were only barriers to a subset of PWD, for example those who are homebound or have difficulty reading. Thus, activities that some could perform unaided require additional resources for others, for example having a person provide physical assistance or read instructions. Other barriers were more situational, with everyone requiring additional resources, such as transportation during inclement weather.
Participants described both taking resource disparities into consideration when planning or recommending activities as well as preferring those activities that required minimal resources:
“I try to plan according [to] what they have. If they don’t have a camera, you can’t ask them to take pictures, but ask them to draw.” John, ABC program
“Exercising is always a good idea because they don’t need anything else, just themselves.” Mary, ABC program
The research team found during immersion that anticipating needed resources was not straightforward. For example, in organizing a crafts activity involving water, researchers brought all the necessary crafting materials but did not anticipate needing materials to absorb and clean up water spillage. This experience highlighted the difficulty of anticipating needed resources.
Involving Informal Caregivers
From participants’ perspectives, involving unpaid informal caregivers, often family members but sometimes friends, is vital for the successful delivery of certain activities. Even when the PWD is the only one performing the activity itself, it is important for caregivers to understand the importance of the activity and believe in its benefits:
“The caregiver can help even [without] participating, recognizing the work shows that they care and makes the patient happier.” Carol, Joy’s House
At the same time, participants were realistic about the difficulty of involving informal caregivers who were busy or tired, particularly when the activity was designed to offer respite to the caregiver. This was one reason for their suggestion to at the very least inform caregivers and secure their buy-in, so they could encourage PWD to perform the activity even without being involved in it themselves.
Having a Backup Plan
During our interviews, participants described that a PWD may disengage from an activity for known and unknown reasons:
“The [PWD] may not want to participate in the planned activity for ‘N’ reasons, and you won’t know exactly why in some cases.” Janet, ABC program
Reasons mentioned for disengagement included those related to the person (e.g., losing interest), the design of the activity (e.g., group size), and situational factors (e.g., bad weather). Because of the risk for disengagement, participants described using backup plans. Backup activities could either replace the initial activity or serve as a second activity to which a PWD could transition once they disengaged from the initial one, illustrated respectively:
“If they can’t do the [outdoors physical] activity, because it is raining, we tell them to just do something else, play some music and dance or sing. Just keep moving.” Janet, ABC program
“We have the activities running in the main room, but the guest can go to another space if they feel like taking a nap or if there is another group just to chat.” Tereza, Joy’s House
Monitoring Time of Day and Energy Levels
Another important aspect of activity delivery described by participants was the timing of the activity and associated variation in PWD energy levels:
“They are more energetic in the morning, so it is easier to have physical activities, then they have lunch and their energy goes down a little.” Carol, Joy’s House
Participants mentioned that energy levels were also affected by environmental factors, such as daytime darkness due to storms signaling bedtime or being influenced by the energy of others during a social activity:
“We need to take care of the energy in the room for an activity. One person can make them too excited or put them down and the activity won’t happen.” Mary, Joy’s House
Service provider participants reported carefully monitoring energy levels during the day. They also described planning dynamic or challenging activities during high-energy times of the day and less challenging or individual activities in the early morning or toward the end of the day:
“The morning we start with calm conversation when they [guests] arrive. They have coffee and we start the stretching when they start to get more active. After, we do some other activity, whatever is planned, but stop it at least a half hour before lunch to let them calm down.” Helena, Joy’s House
Facilitating a Domino Effect
Participants discussed planning for what they called the “domino effect,” or the engagement in future activities as a result of a single initial activity. Participants saw the initiating activity as one that was short or easier to perform, which could lead to performing related but more varied or challenging activities:
“If he goes to pick up the mail, he can talk to a neighbor outside, go to church on Sunday, discover a voluntary group and keep going. It’s like a snowball.” John, ABC program
Participants described envisioning the sequence of future activities when planning. However, when planning sequential activities, they also were cautious to prevent “overdoing it” or starting a PWD down a path that would lead to fatigue or unattainable goals. Participants acknowledged that the circumstantial and probabilistic nature of the domino effect meant it was not something that one could easily predict or control.
Ensuring Safety, First and Foremost
Ensuring safety was viewed as paramount to activity delivery and an overriding goal. This included general safety monitoring and identifying person-specific risks:
“We need to know what they can do and how much supervision they need before recommending an activity.” Meredith, ABC program
Certain activities were perceived to have inherent and unmanageable risks, for example unsupervised meal preparation:
“I’m not sure about cooking. I think that the risks are too high. What if they forget the oven is on? [Or] they can cut themselves.” Carol, Joy’s House
Risk mitigation techniques mentioned included preparing safe physical space and supervision:
“Before anything it needs to be safe …. they can always surprise you, either you have someone with them or do an activity that you know is not dangerous.” Janet, ABC program
Outcomes
Participants described, based on their own experiences, the most common desirable or undesirable outcomes of meaningful activities: feeling fulfilled and having a purpose; overcoming personal challenges; and unexpected triggers. Participants also acknowledged evidence of clinical outcomes such as changes in neuropsychiatric symptoms related to activity engagement.
Feeling Fulfilled and Having a Purpose
A common outcome of PWD engaging in activities, according to participants, is the perception of value and reward, leading to a sense of personal fulfillment and purpose. Some activities produced a clear tangible outcome, such as the meal resulting from a cooking activity. Even when the PWD did not value the product, they sometimes appreciated that the product would have value to someone else, for example, a family member who would receive a painting or pottery:
“When I ask them to paint or to do something I suggest to do [it] for their family, wife, grandkids, someone they love.” Marissa, Joy’s House
Other activities, such as participating in a performance or reading, did not yield a tangible or lasting product. These activities instead resulted in personal satisfaction or feeling useful and recognized by others, for example by family or staff. In immersion sessions, the research team noticed higher engagement in activities that resulted in physical products.
Overcoming Personal Challenges
In interview and immersion sessions, it became apparent that another possible outcome was the satisfaction of overcoming a personal challenge or gaining a sense of mastery:
“… you need to make it [the activity] challenging, see how well they can do and make the activity just right to push them a little more.” John, ABC program
During immersion sessions, the research team saw that PWD liked to try new activities, suggesting they may enjoy the challenge of something new. During one activity, PWD were asked to paint and write messages on pictures for Halloween decorations. Participants with higher skill and energy levels were not satisfied. They took on additional challenges such as drawing their own illustrations and deciding where to place the decorations in the facility.
Unexpected Triggers
Participants discussed how problematic behaviors such as frustration or anger were triggered by some aspect of the activity. They described some triggers as unpredictable or producing unexpected responses:
“You never know what is coming, any small thing can make them react.” Janet, ABC program
“You should always expect the unexpected.” Carol, Joy’s House
During the immersion sessions, unexpected triggers were observed multiple times. During an activity to craft a musical instrument to play together, one PWD became angry because the activity was taking longer than scheduled. This individual confiscated some of the crafting materials, refusing to return them until the activity was stopped.
Discussion
The success factors for activities for PWD are important to establish from multiple perspectives, especially as healthcare professionals, informal caregivers, and PWD appear to differ in their opinions of what makes meaningful activities meaningful (Harmer & Orrell, 2008). This study reported community-based providers’ experiences and perceptions of the content, delivery, and outcome characteristics of successful activities for PWD. Several study findings were especially notable and are discussed below.
With respect to activity content, we found that activities resonating with the PWD’s past were perceived as more successful. This corresponds with the frequent finding that tailored activities reduce behavioral symptoms of dementia (Gitlin et al., 2008). The personalization of activities furthers the personhood of the PWD: it recognizes the presence of the PWD as an active agent, not merely a consumer of activities, and acknowledges the present or past identity of the PWD as vital to making decisions (Hughes, 2014; Jenkins & Price, 1996; O’Connor & Purves, 2009). In addition, study participants echoed the prevailing recommendations for strengths-based approaches to recreation therapy for PWD, which entail attention to participant preferences, interests, and abilities, not merely their deficits or limitations (Buettner & Kolanowski, 2003; Öhman & Nygård, 2005). Social activities were described as a desirable opportunity to engage with others and social activities may improve multiple outcomes for PWD and their informal caregivers (Särkämö et al., 2014). It was unclear, from our study, whether all individuals and informal caregivers equally enjoy social activities, especially when the purpose of the activity is to provide respite to the caregiver. Participants’ responses indicated that meaningful activities are not static and, when possible, should present novel challenges or increasing levels of challenge, in line with PWD’s progress and tolerance. Phinney et al. (2007) similarly observed that PWD can accomplish challenging activities and may find the challenge rewarding. At the same time, others note the need to design activities to not exceed physical or cognitive capacity of PWD (Kolanowski et al., 2008), although cognitive capacity may be misperceived in PWD (Burns et al., 2006). The implication for practice is to strive for balance in activity difficulty, with neither too much nor too little, along with appropriate monitoring to adjust the level of challenge over time.
Study participants noted several strategies to ensure successful delivery of activities, including monitoring PWD energy levels, involving informal caregivers, managing resources, and ensuring safety. The need for such delivery strategies stems in part from the known influence of situational factors such as time, sound levels, and group size on activity engagement (Cohen-Mansfield et al., 2009). Community service provider participants sometimes faced difficulties monitoring, accounting for, or controlling these factors, especially when the PWD was performing activities at home. Furthermore, it was clear from interviews that not all delivery strategies were equally effective for different individuals, activities, or points in time. Another notable finding about activity delivery was what we call the domino effect, in which engaging in one activity can lead to engagement in another, and so forth. Additional research is warranted on strategies used to deliver meaningful activities, the relative advantage of each under differing conditions, and especially strategies that promote the domino effect, and PWD resilience in general (Harris, 2008). Work should be done to also adapt known strategies to settings outside formal care or day service facilities, for example, activities that can be delivered in the home or performed autonomously by the PWD, with or without an informal caregiver’s assistance. Activities that can be performed safely and successfully in the home or at least independent of specific settings and their human and material resources, are much more scalable, especially across demographic and geographic groups. Furthermore, we see an opportunity for interventions such as staff training or technology to help professionals deliver activities. In addition to activities that are presented via technology, for example, videos or games on a surface tablet, technologies offer functionality to support activity delivery. This includes monitoring the behavior, engagement, or performance of a PWD as they complete an activity, or offering help and assistance using built-in tutorials or live video conferencing with a human or digital assistant.
Participants described a key outcome of successful activities was the PWD’s sense of personal fulfillment and purpose, which others have reported as a principal unmet need of PWD addressable with meaningful activities (Miranda-Castillo et al., 2013). Less explored are the outcomes of feeling mastery and the satisfaction of overcoming a challenge, which is related to the above concept of providing PWD with activities that are sufficiently challenging. Research is needed to demonstrate this outcome and to link it to other outcomes such as PWD quality of life or willingness to engage with future activity offerings. A final noteworthy outcome described is the unintended consequence of activities triggering undesirable reactions, including emotional distress. This finding suggests that meaningful activities are not risk-free and require the management of physical and emotional safety. Together, the findings from this study offer several recommendations for research and practice, presented in Table 2.
Research and Practice Recommendations.

Abbreviation: PWD = persons with dementia.
Our study had methodological strengths and weaknesses. We were able to capture the perspectives of individuals who work with PWD in two types of community-based care organizations, one providing formal biopsychosocial care delivery (ABC program) and the other an adult day service (Joy’s House). The adult day service had a strong orientation toward enrichment activities, potentially distinguishing it from similar settings that prioritize respite goals (Abramson, 2009). Other settings for activity delivery, such as assisted living or long-term care facilities were not included, nor did we involve PWD or informal caregivers in this study. In total, 15 individuals participated across the six group interviews, but some participated in multiple interviews, with a mode of four per interview. This resulted in a large corpus of data compared to similar group interview or focus group studies. Although the sampling strategy and sample size in this study were insufficient to generalize results to the population, this was not the purpose of this qualitative study. Future work seeking to create generalizable knowledge regarding meaningful activity content, delivery, and outcomes should be carried out with larger and more heterogeneous samples across multiple geographic and organizational sites, with random or stratified sampling and using multiple, mixed methods including semistructured interview, observation, and standardized surveys. Further research is also needed to translate findings into interventions to test whether these activities are “successful” (e.g., acceptable, engaging) and “meaningful,” using validated measures (Eakman et al., 2010; Gitlin et al., 2009). A final strength of this study was that interviews were supplemented by researcher immersion as activity volunteers at one of the research sites, allowing researchers to gain personal experiences with the phenomenon of interest. The use of immersion was time-consuming but facilitated data collection and analysis.
Conclusion
While there is no singular way to create or deliver successful meaningful activities, there are several factors that may promote their success. Importantly, success is not only a matter of “what” the activity is, but also how it is delivered and what outcomes it produces. Drawing on their unique experiences and perspectives, professionals readily described the strategies they use to achieve success with meaningful activities, many of which can be replicated across settings and potentially supported with interventions such as training and technology. On the whole, the principal gap seen in professionals’ experiences with activities is the lack of support to monitor and adjust activities over time; this gap is especially salient because activities are clearly part of a dynamic process involving change over time in the PWD and their environments. By implication, activities must be dynamic as well, involving incremental challenge, a sense of mastery and accomplishment, and domino effects. Given agreement in the literature of the value of meaningful activities for PWD, the next steps for research and development in this area should be to create and test innovative dynamic approaches to providing activities to PWD, using emerging technologies where applicable.
Footnotes
Appendix: Group Interview Session Procedure and Example Probes.
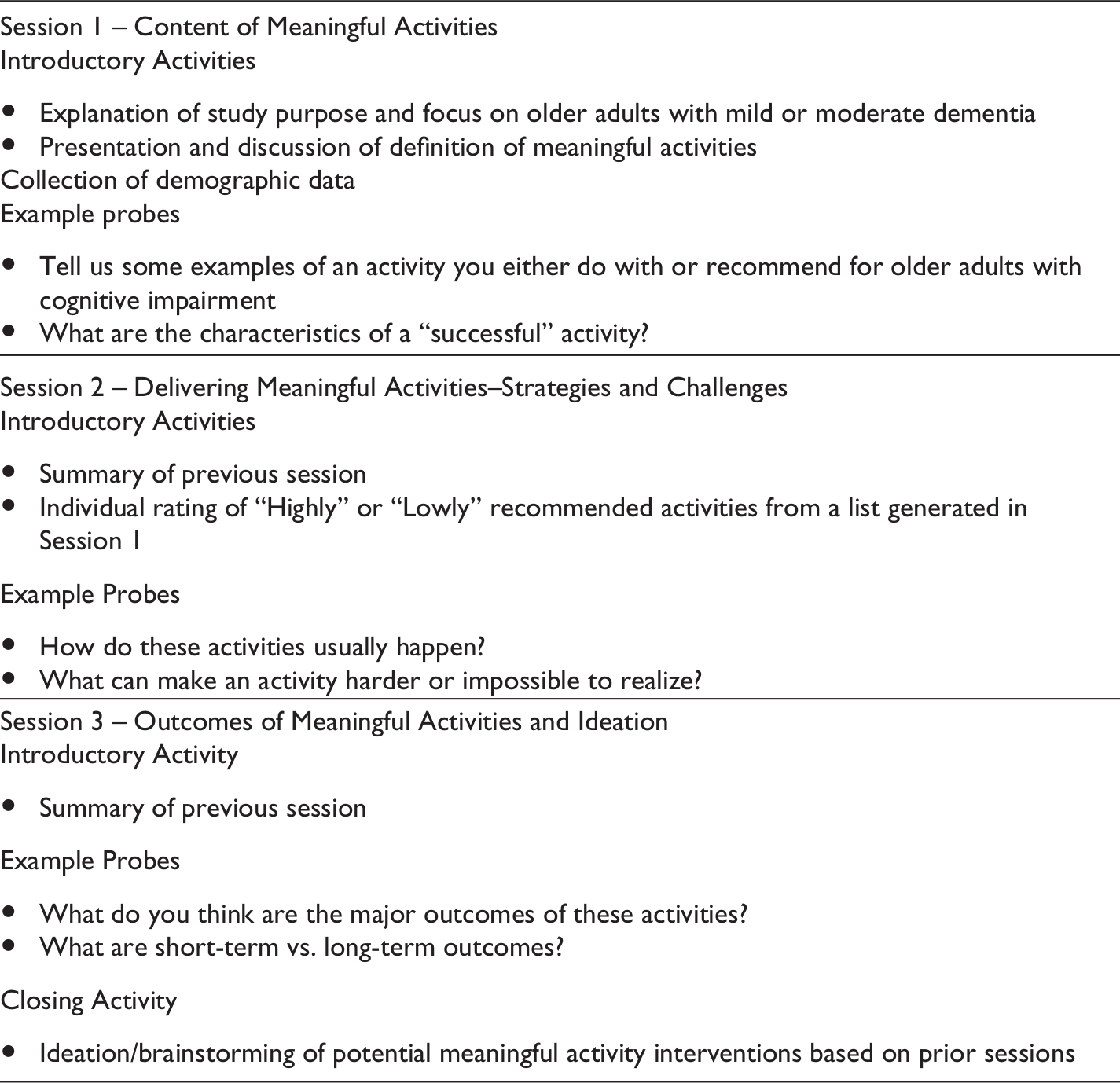
| Session 1 – Content of Meaningful Activities Explanation of study purpose and focus on older adults with mild or moderate dementia Presentation and discussion of definition of meaningful activities Collection of demographic data Tell us some examples of an activity you either do with or recommend for older adults with cognitive impairment What are the characteristics of a “successful” activity? |
|---|
| Session 2 – Delivering Meaningful Activities–Strategies and Challenges Introductory Activities Summary of previous session Individual rating of “Highly” or “Lowly” recommended activities from a list generated in Session 1 Example Probes How do these activities usually happen? What can make an activity harder or impossible to realize? |
| Session 3 – Outcomes of Meaningful Activities and Ideation Introductory Activity Summary of previous session Example Probes What do you think are the major outcomes of these activities? What are short-term vs. long-term outcomes? Closing Activity Ideation/brainstorming of potential meaningful activity interventions based on prior sessions |
Acknowledgments
We thank study participants and colleagues at Joy’s House and the Aging Brain Care program at the Sandra Eskenazi Center for Brain Care Innovation. Other contributing members of the project team were Jessica Blackburn, Prasanthi Kodthala, and Amy Miller.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Sheetz was employed by Joy’s House at the time the study was performed. Dr. Holden was a member of the Board of Advisors for Joy’s House. Drs. Holden and Fowler have served as members of the Board of Advisors for Joy’s House. Dr. Bateman is a physician provider in the Aging Brain Care (ABC) program.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Charles R. Bantz Community Scholar Award from the Indiana University Purdue University–Indianapolis (IUPUI) Office of the Vice Chancellor for Research to author RJH for the Brain-Protective Health Information Technology initiative, a.k.a., B-PHIT Indy.
Author Biographies
At the time of the study, Mr.
At the time of the study, Ms.
Dr.
At the time of the study, Dr.
Dr.
At the time of the study, Mr.
At the time of the study, Ms.