
Abstract
Research suggests that clinical management of cognitive impairment can occur through interventions targeting lifestyle factors, such as physical exercise and sleep quality. The present study examined the associations among lifestyle factors (exercise and sleep quality), cognition, and functional capacity in older adults (ages 56–94) who completed an outpatient neuropsychological evaluation (N = 356). Exercise habits and sleep quality were accessed using a self-report questionnaire and a clinical interview. Cognitive functioning was assessed using the Dementia Rating Scale-2 (DRS-2). Functional capacity was measured by the Texas Functional Living Scale (TFLS). Results indicated that physical exercise and sleep quality were positively associated with better cognitive functioning and functional capacity. Further research is needed to elucidate the relationship between lifestyle factors, cognition, and functional capacity in older adults.
By 2050, the United States is expected to experience a significant growth in its older population, with approximately 84 million adults over the age of 65, which will almost double the estimated population of 43 million in this age range in 2012 (Ortman et al., 2014). Concurrent with this increase, the projected number of individuals with various forms of cognitive impairment is also expected to grow; it has been estimated that by 2050 the number of individuals living with dementia worldwide would triple compared to 2010 (Prince et al., 2013). Although pharmacological treatments aimed at slowing down the progression of cognitive decline have been investigated in the recent years, no disease-modifying treatments have been discovered to date. Consequently, lifestyle interventions aimed at prevention or attenuation of cognitive decline have received increasing attention in the published literature in the recent decades. Specifically, physical exercise and sleep quality have been examined in relation to cognitive functioning, among other modifiable factors (Baumgart et al., 2015).
Exercise
Published research has consistently shown a positive relationship between physical activity and cognitive functioning across the lifespan (Baumgart et al., 2015; Donnelly et al., 2016; Ludyga et al., 2020; Sofi et al., 2011), and these findings have been specifically demonstrated in older adults (Chu et al., 2015; Hogan, 2005; Northey et al., 2018; Öhman et al., 2014). Some studies suggest that exercise performed in midlife is associated with reduced risk of having a cognitive impairment later in life (Ahlskog et al., 2011; Geda et al., 2010). Although some studies have suggested that exercise may affect specific domains of cognitive functioning, such as executive functioning, attention, delayed recall, and verbal fluency (e.g., Barha et al., 2017; Öhman et al., 2014), other studies have revealed global rather than domain-specific effects of exercise on cognition (Ludyga et al., 2020).
Evidence supporting specific types of physical activity is mixed, but exercise that elevates heart rate appears to garner the most support (e.g., Geda et al., 2010; Hoffmann et al., 2016). Some investigators have suggested that aerobic training may lead to greater benefits than resistance training in older adults (Barha et al., 2017), but both aerobic and anaerobic exercise have been related to cognitive health in older adulthood (Ahlskog et al., 2011; Northey et al., 2018; Voss et al., 2011). Additionally, balance exercises have also been recommended for older adults with mild cognitive impairment, along with aerobic physical activity and progressive resistance training (Chong et al., 2020).
Exact mechanisms for the beneficial effects of exercise on cognition are still being investigated, but it has been posited that physical exercise may mitigate cognitive decline through attenuation of cerebrovascular risk (Ahlskog et al., 2011). It has also been hypothesized that exercise may have a neuroprotective effect, as aerobic exercise has been associated with a larger hippocampal volume and decreased gray matter loss(Ahlskog et al., 2011). Physical activity has also been associated with a favorable biomarker profile for Alzheimer’s disease (Law et al., 2018). Finally, exercise has been implicated in neurogenesis at least in the hippocampus (Churchill et al., 2002), which may explain improved outcomes in memory and learning. Overall, reviews of both animal and human studies have consistently identified the importance of exercise for maintaining cognitive function (Voss et al., 2011).
Sleep
Sleep is another lifestyle factor that has been associated with cognitive functioning (Dzierzewski et al., 2018). Considering that sleep concerns are prevalent in older adults (Blay et al., 2008), and that individuals with cognitive impairment may experience more severe sleep disturbances than cognitively intact older adults (Cochen et al., 2009), examining the relationship between sleep concerns and cognitive function has high clinical relevance. Notably, a bidirectional relationship may exist between sleep quality and cognitive disorders (Ju et al., 2014). Sleep-wake cycle may affect the levels of amyloid-β (Aβ) peptide in the brain, which has been linked to the pathogenesis of Alzheimer’s disease. This accumulation in turn may increase wakefulness and alter sleep patterns. Therefore, sleep and neurodegenerative disease may affect one another bidirectionally (Ju et al., 2014), and it is not clear which process or disruption begins first.
Various sleep factors have been examined in relation to cognition, including sleep duration, subjective feelings of tiredness, sleep quality, and sleep disorders. Studies investigating the effects of sleep duration on cognition have revealed contradictory findings. Some studies indicate that long sleep duration may be related to worse cognitive functioning (Faubel et al., 2009), while others demonstrate a U-shaped relationship between sleep duration and cognitive functioning, in which both short and long sleep duration are association with worse neurocognitive performance (Kronholm et al., 2009). Subjective fatigue and poor sleep quality have also been linked with worse cognition (Kronholm et al., 2009; Potvin et al., 2012). A number of sleep disorders (e.g., insomnia and sleep apnea) have also been correlated with poorer cognitive functioning and with a higher incidence of cognitive impairment (Chang et al., 2013; Chen et al., 2012; Sterniczuk et al., 2013; Yaffe et al., 2011). For example, Chen et al. (2012) reported that individuals with long-term insomnia had significantly higher risk of dementia. In a similar vein, Chang et al. (2013) demonstrated that patients with sleep apnea had a 1.7-times greater risk of developing dementia. Likewise, Sterniczuk et al. (2013) reported that sleep disturbance was associated with an increased risk of developing Alzheimer’s disease.
Overall, published research indicates that sleep disturbances significantly affect the progression of brain aging and cognitive impairment (Yaffe et al., 2014). Furthermore, poor sleep quality has been associated with widespread atrophy in the frontal, temporal, and parietal regions of the brain (Sexton et al., 2014), but it is unclear if sleep quality is the cause or a consequence of this cortical atrophy. It is also unknown whether sleep disturbance causes cognitive decline or is an associated precursor for dementia (Baumgart et al., 2015). However, it appears that treatments for at least some sleep disorders (such as sleep-disordered breathing) may delay progression of cognitive impairment (Osorio et al., 2015). This suggests that addressing sleep concerns in older adults may be one of the avenues of preserving cognitive functioning and mitigating cognitive decline.
Lifestyle Factors and Functional Capacity
Functional capacity and cognitive functioning are related in that individuals with cognitive dysfunction are likely to demonstrate functional impairment that exceeds the level of age-related functional decline demonstrated by their cognitively normal peers (De Vriendt et al., 2012; Vermeersch et al., 2015). Lifestyle factors associated with cognitive impairment demonstrate similar directionality in the relationships with functional impairment. For example, exercise frequency and sleep duration have been associated with decreased functional disability incidence in the elderly (Liao et al., 2011). Specifically, older adults who regularly engage in healthy behaviors (such as physical exercise, sleeping 6–8 hr per day, non-smoking, etc.) may be 15%–75% less likely to be functionally disabled than those who do not.
In terms of physical activity, extant research consistently suggests that exercise correlates with better functional capacity, as measured by performance on assessments of activities of daily living (ADLs) and instrumental activities of daily living (IADLs). For instance, a systematic review of over 100 studies examining the relationship between physical activity and functional independence (as well as cognitive functioning) demonstrated that exercise interventions may enhance both physiological and functional status in older age (Paterson & Warburton, 2010). Another recent study revealed that a 12-week physical exercise program has been shown to improve some physical functional capabilities in older adults (Scarabottolo et al., 2017). Moreover, exercise has been shown to improve both cognition and functional ability in individuals with dementia (Vreugdenhil et al., 2012). Physical exercise may be directly related not only to the ability to function independently, but also to personal satisfaction with functional capacity (Crevenna & Dorner, 2019), and it has been shown that exercise helps maintain functional ability. After controlling for health-related factors (such as the presence of disease and health deterioration with age), frequency of exercise has been shown to correlate with ease in performing tasks related to functional capacity over time (Stessman et al., 2002).
Sleep quality and sleep duration have also been associated with functional capacity in older adults. However, it remains unclear which facets of sleep disturbance (poor sleep quality or sleep duration) have the strongest correlation with functional impairment. Some studies have demonstrated a relationship between functional impairment and sleep duration, while others have identified sleep quality as more salient. To illustrate, both excess sleep (>8 hr) and insufficient sleep (<6 hr) have been shown to predict diminished functional capacity (Brimah et al., 2013). Similarly, poor sleep quality has been significantly associated with physical disability (Chien & Chen, 2015), but sleep duration has been linked with more global functional impairment in older adults (Vincent et al., 2021). In another study, sleep quality but not duration was associated with the development of physical impairment (Campanini et al., 2019). The directionality of the relationship between sleep and functioning is also not well understood, as some studies have demonstrated that functional impairment may in fact predict poor sleep quality in older adults (Li et al., 2013).
In addition, published studies suggest that lifestyle interventions may have a multidirectional and synergistic relationship with other lifestyle variables as well as markers of functioning. For example, a combination of moderate aerobic exercise, resistance training, and activities focused on balance and motor coordination has been shown to improve both sleep quality and complex functional capacity (Nascimento et al., 2014). Furthermore, recent research has demonstrated that both physical inactivity and poor sleep habits (e.g., short or prolonged sleep duration) are among important lifestyle risk factors for ADL/IADL disability in older adults (Storeng et al., 2018).
Overall, it is important to note that research investigating various physical aspects of functional capacity in older adulthood has been emerging in the recent years. However, the number of studies focusing specifically on cognitive aspects of functional abilities (e.g., ability to manage one’s medications, keep up with medical appointments and treatments, effectively manage finances, etc.) is still rather small. Thus, further exploration of lifestyle factors and their association with functioning (both physical and cognitive) in older adults is necessary.
Rationale for the Present Study
Published research has investigated individual lifestyle factors, but studies exploring the combined effects of several health-promoting behaviors continue to be quite limited. Findings of the few rare studies in this area point to the synergistic effects of combining health-promoting behaviors. For example, Kesse-Guyot et al. (2014) examined associations between individual and combined lifestyle factors in middle age and cognitive functioning later in life. They found that global cognitive function and verbal memory were negatively associated with the number of unhealthy behaviors midlife (Kesse-Guyot et al., 2014). Additionally, although the interplay between lifestyle factors and cognition has received burgeoning attention in the recent decades, less is known about the effects of exercise and sleep on adaptive functioning in older adults. Because lower scores on measures of cognitive functioning have been correlated with decreased functional capacity in older adults (Aretouli & Brandt, 2010; Baird, 2006; Burton et al., 2009; Fong et al., 2015; Mcalister et al., 2016; Ord et al., 2019), it may be reasonable to question whether lifestyle factors have beneficial effects on functional abilities as well. For example, Karssemeijer et al. (2017) reported positive effects of combined cognitive-physical interventions on activities of daily living in older adults with mild cognitive impairment (MCI) or dementia. However, the body of research examining the associations between lifestyle factors and adaptive functioning remains limited, warranting further examination.
In summary, previously published research has demonstrated that physical exercise and sleep quality are independently linked with cognitive functioning. However, less is known about compounding effects of multiple lifestyle factors on cognition. Additionally, the association between these lifestyle factors and functional abilities remains under-researched. The current study sought to fill these gaps in published literature. The primary aim was to further elucidate the nature of the relationships among modifiable lifestyle factors (both individually and in combination), cognitive function, and functional abilities in older adults. It was hypothesized that participants who report regularly engaging in physical activity and having good sleep quality (independently or in combination) would have better scores on measures of cognitive functioning and functional abilities, as compared to those reporting no health-promoting behaviors.
Method
Procedure
The study was reviewed and received approval by the Human Subjects Review Committee (HSRC) at Regent University. The study involved retrospective chart review of 356 older adults evaluated at a private outpatient neuropsychology practice. Consecutive referrals were utilized, but if participants were not administered the measures utilized in the present study or if their data were incomplete (e.g., if they did not complete a clinical history form), they were excluded from the present analyses. The patients were referred for an assessment by their primary care provider or a specialist (e.g., a neurologist or a psychiatrist). Common referral questions included examination of subjective cognitive complaints (e.g., problems with memory and concentration) as well as assistance with a differential diagnosis of cognitive complaints (normal aging vs. a mild or major neurocognitive disorder). Referring providers also commonly requested examination of cognitive strengths and weaknesses as well as treatment recommendations. All assessments included in the present study were completed as part of a medically necessary clinical neuropsychological evaluation; none were conducted in a forensic, research, or another nonclinical context.
Participants
In this sample, age ranged from 56 to 94 years, with an average age of 73 (SD = 8.30) years. Average education level was 14.11 (SD = 2.68) years. In terms of gender, the sample was approximately 43% male and 57% female. Approximately 65.5% of the sample reported Caucasian race. In terms of medical diagnoses, the vast majority of participants (n = 268; 75%) had at least one active medical diagnosis, with an average number of medical diagnoses reported per person ranging from 0 to 17 (M = 2.56, SD = 2.93). Most commonly reported medical diagnoses included hypertension (n = 154; 43.3%), diabetes (n = 82; 23%), hyperlipidemia (n = 53; 14.9%), arthritis (n = 42; 11.8%), heart disease (n = 28; 7.9%), non-central nervous system (CNS) cancer (n = 20; 5.6%; most common: breast, prostate, and skin cancer); gastroesophageal reflux disease (n = 11; 3%), and kidney disease (n = 8, 2.2%). Approximately one-third of participants had history of a neurological disorder (n = 104, 29.2%). Most common neurological presentations included a neurocognitive disorder (n = 80, 22.5%), stroke (n = 18, 5%), migraines (n = 13, 3.7%), traumatic brain injury (n = 9; 2.5%), seizure disorder (n = 9; 2.5%), Parkinson’s disease (n = 8; 2.2%), multiple sclerosis (n = 3; 1%), and brain tumor (n = 1; 0.3%; meningioma). Almost one-quarter of participants had a diagnosable psychiatric disorder (n = 84, 23.6%), such as a depressive disorder (n = 60; 16.9%), anxiety disorder (n = 37, 10.4%), or PTSD (n = 11; 3.1%). Detailed characteristics of the studied sample are presented in Table 1.
Sociodemographic Characteristics of Participants (N = 356).

Note. DRS-2 = Mattis Dementia Rating Scale-2; AEMSS = Age- and Education-Corrected MOANS Scaled Score (M = 10; SD = 3); MOANS = Mayo’s Older Americans Normative Studies; TFLS = Texas Functional Living Scale; TOPF = Test of Premorbid Functioning; number of medical conditions = average number of active medical problems reported for each participant; psychiatric disorder = number of participants diagnosed with a psychiatric disorder; neurological disorder = number of participants diagnosed with a neurological disorder.
Participants completed a clinical history form (medical, psychiatric, and social), a clinical interview, the revised Dementia Rating Scale-2 (DRS-2), the Texas Functional Living Scale (TFLS), the Test of Premorbid Functioning (TOPF), and measures of performance validity (ACS Word Choice Test and Green’s Medical Symptom Validity Test), among other tests of neuropsychological functioning. Only participants who passed performance validity measures were included in the current analyses. In the present study, all interviews were completed by a board-certified neuropsychologist or a licensed clinical psychologist with specialized post-doctoral training in clinical neuropsychology. All assessments were administered and scored by the aforementioned clinicians or by psychometrists with specialized training in neuropsychological assessment (under supervision of doctoral-level psychologists).
Measures
Exercise, Sleep, and Health Conditions
Exercise and sleep habits were assessed using the clinical history form and the subsequent clinical interview. During intake assessments, participants completed a history form on which they indicated whether they engaged in regular physical exercise or experienced any sleep disturbances. Questions that were included in the clinical history form stated, “Do you exercise on a regular basis?” and “Do you have any sleep complaints?” Patients circled “yes” or “no” in response to these questions. Responses were later reviewed and discussed in clinical interviews (completed by doctoral-level psychologists or a board-certified neuropsychologist) to obtain further information regarding exercise and sleep habits. Based on the follow-up questions, the doctoral-level clinician made a determination whether the patient’s responses would be dichotomized into “yes” or “no” category regarding regular exercise and sleep disturbance. This information was later used in the clinical report to provide treatment recommendations. Participants also reported their psychiatric, neurologic, and medical conditions on the clinical history form. These data combined with medical records received from referring providers were used to determine participants’ health status.
Revised Dementia Rating Scale-2 (DRS-2)
The Mattis DRS is a neuropsychological measure of cognitive functioning (Smith et al., 1994). Early investigations of the psychometric qualities of the original DRS found that total scores correlated with cognitive decline (Smith et al., 1994). In terms of convergent validity, DRS scores correlated with age, education, and intelligence quotient (Smith et al., 1994). DRS subscales also significantly correlated with appropriate indices from the Wechsler Adult Intelligence Scale-Revised and the Wechsler Memory Scale-Revised (Smith et al., 1994). The current study utilized the revised version, DRS-2, a 144-item assessment of cognitive status in adults with cognitive impairment (Jurica et al., 2001). This instrument assesses several facets of cognitive functioning that are impacted by dementia including attention, initiation and perseveration, construction, conceptualization, and memory (Jurica et al., 2001). Cronbach’s α for the DRS-2 in the present sample was 0.77, indicating acceptable internal consistency (Tavakol & Dennick, 2011). DRS-2 age- and education-corrected scale scores (AEMSS) were used in the present study; higher scores represent better cognitive functioning.
Texas Functional Living Scale (TFLS)
The TFLS (Cullum et al., 2009) is a measure of IADLs. TFLS includes 24 performance-based items and yields a total score, as well as four subscale scores: time, money and calculation, communication, and memory (Cullum et al., 2009). The TFLS incorporates ecologically valid tasks, including hands-on calculations with money (e.g., providing change), using an analog clock, calendar, check book, phone, and setting a microwave (Whipple Drozdick & Cullum, 2011). The TFLS has demonstrated evidence of robust reliability, internal consistency, and validity (both convergent and discriminant) with several measures of adaptive functioning (Cullum et al., 2001). The TFLS has also been found to strongly correlate with concurrent criteria, including the Mini-Mental State Examination (0.92) and informant-based ratings of daily living skills (Cullum et al., 2001). TFLS subscale scores have been shown to be highly correlated (r > 0.90 for most) with the TFLS total score (Cullum et al., 2001). Cronbach’s α for the TFLS in the present sample was 0.73, indicating acceptable internal consistency (Tavakol & Dennick, 2011). The TFLS total scores were utilized in the present study to assess functional abilities; higher scores represent better functional capacity.
Test of Premorbid Functioning (TOPF)
The TOPF was designed to estimate premorbid cognitive abilities of individuals ages 16–90 (Pearson, 2009). The TOPF is a successor of the Wechsler Test of Adult Reading (Ginsberg, 2003). TOPF standard scores were utilized in the present study.
Statistical Analyses
Two univariate factorial analyses of variance (ANCOVA) were conducted to evaluate differences in cognitive functioning (measured by the DRS-2 AEMSS total) and functional capacity (measured by the TFLS total score) based on exercise and sleep complaints while adjusting for the number of health conditions, psychiatric diagnoses, neurological diagnoses, and premorbid functioning. Because DRS-2 AEMSS scores are already adjusted for age and education, no additional covariates were added in the DRS-2 models. However, given that raw total TFLS scores were utilized in the present study, all models involving TFLS also included age and education as demographic covariates. Follow-up multivariate analysis of covariance (MANCOVA) was also conducted with five DRS-2 subscale scores as dependent variables to ascertain which facets of cognitive functioning are associated with sleep and exercise. Exercise and sleep complaints were included as two independent variables in each analysis. These were dichotomized based on participants’ self-report on the clinical history form and the clinical interviews. All analyses were completed using Statistical Package for the Social Sciences (SPSS) version 25.0. To reduce Type I error due to multiple comparisons, false discovery rate (FDR; Benjamini & Hochberg, 1995) was used to determine significant outcomes (step-down approach), correcting the FDR at p < .05. Prior to analyses, data were screened for data entry errors, missing values, as well as univariate and multivariate outliers. No nonrandom patterns in missing data have been identified and missing values were not replaced. Additionally, data were examined for normality and homogeneity of variance. These examinations revealed that assumptions for ANCOVA and MANCOVA analyses were met and further analysis was acceptable.
Results
Cognitive Functioning
Results of the ANCOVA (with DRS-2 AEMSS total as the dependent variable and the following covariates: premorbid functioning, medical, neurological, and psychiatric conditions) indicated significant differences in global cognitive functioning based on both exercise and sleep habits. Interaction between sleep and exercise was not significant (Table 2). Post-hoc comparison of means revealed that participants who reported regularly engaging in physical exercise displayed significantly higher DRS-2 scores, as compared to participants who did not exercise regularly. Similarly, participants who reported no sleep concerns had a higher mean DRS-2 score, compared to DRS-2 scores of participants endorsing sleep problems. Means, standard errors, and effect sizes for all main effects are presented in Table 3. Exploratory post-hoc pairwise comparisons (Bonferroni adjusted) revealed that participants who reported exercising with no sleep problems had the highest DRS-2 total scores, whereas participants who reported not exercising and endorsed sleep concerns had the lowest DRS-2 total scores (scores between these two groups were statistically significantly different). Participants who endorsed only one positive health factor (e.g., exercising regularly or no sleep concerns) were not significantly different from one another (or from the lowest and highest groups) and received scores that were between the groups endorsing both or no health factors. Descriptive statistics for these exploratory comparisons are presented in Table 4. Graphic representation of DRS-2 scores based on self-reported exercise habits and sleep complaints can be found in Figure 1.

DRS-2 age- and education-corrected MOANS scaled scores based on self-reported exercise habits and sleep complaints. Note. DRS-2 = Dementia Rating Scale-2; MOANS = Mayo’s Older Americans Normative Studies. Higher scores represent better cognitive functioning. Error bars represent standard error.
Results of MANCOVA and ANCOVA Analyses for Cognitive Functioning (DRS-2) and Functional Capacity (TFLS) Based on Sleep and Exercise Habits.
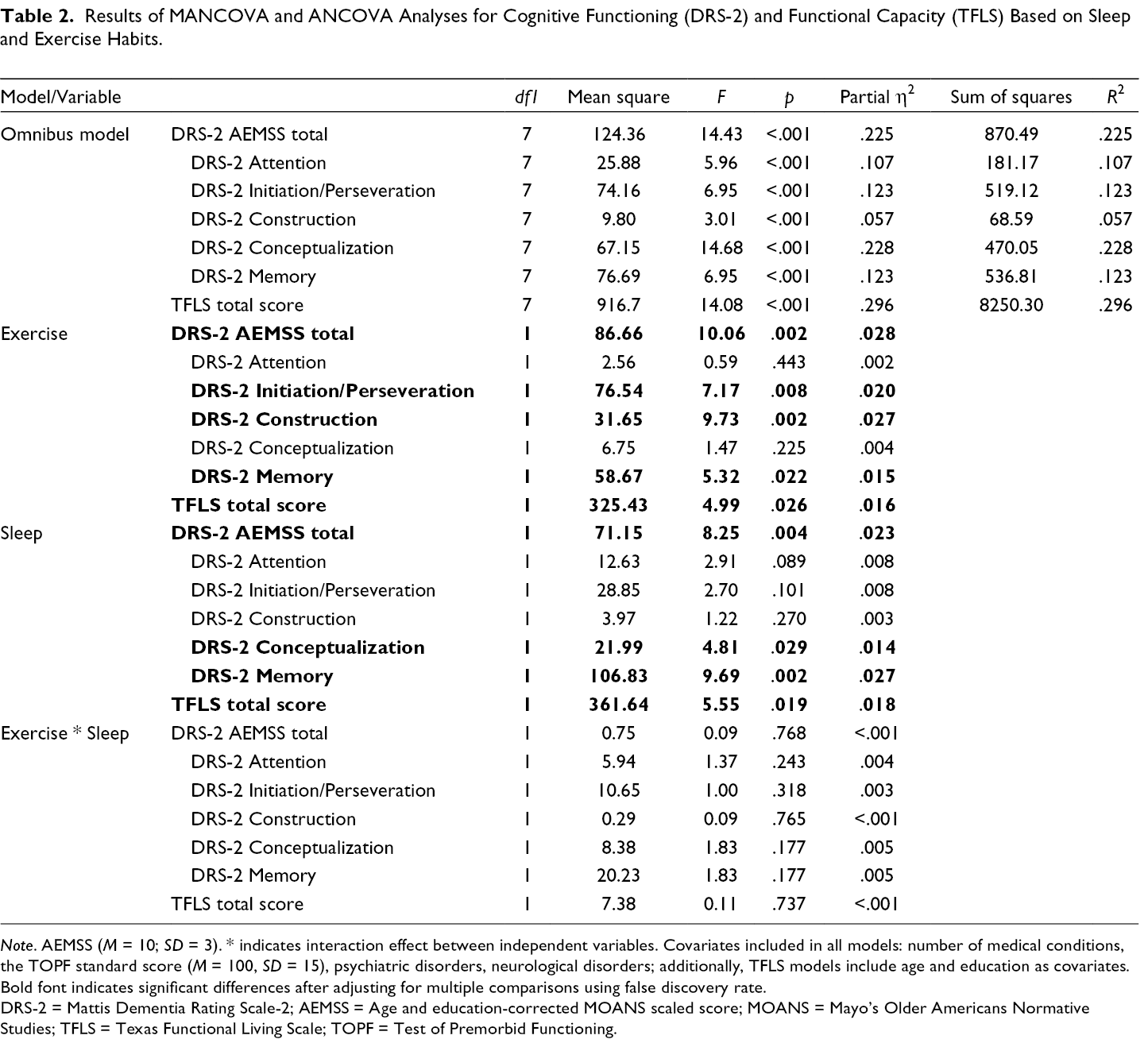
Note. AEMSS (M = 10; SD = 3). * indicates interaction effect between independent variables. Covariates included in all models: number of medical conditions, the TOPF standard score (M = 100, SD = 15), psychiatric disorders, neurological disorders; additionally, TFLS models include age and education as covariates.
Bold font indicates significant differences after adjusting for multiple comparisons using false discovery rate.
DRS-2 = Mattis Dementia Rating Scale-2; AEMSS = Age and education-corrected MOANS scaled score; MOANS = Mayo’s Older Americans Normative Studies; TFLS = Texas Functional Living Scale; TOPF = Test of Premorbid Functioning.
Descriptive Statistics for ANCOVAs Comparing Cognitive Functioning and Functional Capacity Levels Based on Lifestyle Factors.

Note. AEMSS (M = 10; SD = 3). Covariates included in all models: number of medical conditions, the TOPF standard score (M = 100, SD = 15), psychiatric disorders, and neurological disorders; additionally, TFLS models include age and education as covariates. Higher scores represent better cognitive functioning (DRS-2) or better functional capacity (TFLS).
Bold font indicates significant differences after adjusting for multiple comparisons using false discovery rate.
DRS-2 = Mattis Dementia Rating Scale-2; AEMSS = Age and education-corrected MOANS scaled score; MOANS = Mayo’s Older Americans Normative Studies; TFLS = Texas Functional Living Scale; TOPF = Test of Premorbid Functioning.
Post-Hoc Pairwise Comparisons Examining Combined Effects of Exercise and Sleep Disturbance on Cognitive Functioning and Functional Capacity.
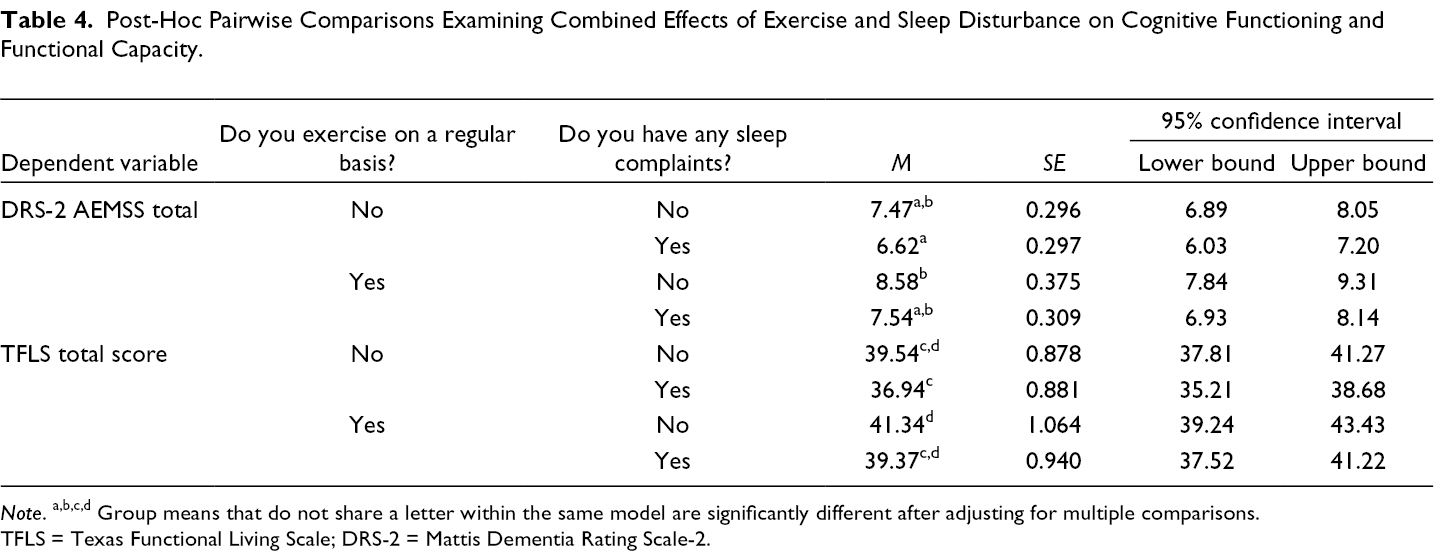
Note. a,b,c,d Group means that do not share a letter within the same model are significantly different after adjusting for multiple comparisons.
TFLS = Texas Functional Living Scale; DRS-2 = Mattis Dementia Rating Scale-2.
Follow-up MANCOVA was conducted to examine differences in DRS-2 subscales based on self-reported exercise and sleep habits. Five subscales of the DRS-2 were included as dependent variables, whereas premorbid functioning as well as medical, neurological, and psychiatric conditions were included as covariates. The omnibus MANCOVA model revealed significant main effects for exercise (Wilks λ = .958, F(5, 344) = 3.02, p = .011, partial η2 = .042) and sleep (Wilks λ = .955, F(5, 344) = 3.26, p = .007, partial η2 = .045) on the combined dependent variable (DV). Interaction between the two factors was not significant (Wilks λ = .974, F(5, 344) = 1.86, p = .101, partial η2 = .026) for the combined DV. Significant main effects for exercise were also observed on the following three subscales of the DRS-2: initiation/perseveration, construction, and memory. Significant main effects for sleep were observed for conceptualization and memory subscales. Interactions were not significant for any of the DRS-2 subscales. Comprehensive information for these analyses is presented in Table 2.
Functional Capacity
Next, an ANCOVA was conducted to evaluate differences in adaptive functioning (measured by the TFLS total score as the dependent variable and the following covariates: age, education, premorbid functioning, medical, neurological, and psychiatric conditions) based on exercise and sleep quality. Results of this ANCOVA revealed significant differences in functional capacity based on exercise and sleep quality. Interactions among independent variables again were not significant. Post-hoc comparison of means revealed that participants who reported regularly engaging in physical exercise and those who denied subjective sleep complaints had significantly higher TFLS scores. Means, standard errors, and effect sizes for all main effects are presented in Table 3. Exploratory post-hoc pairwise comparisons (Bonferroni adjusted) revealed that participants who reported exercising with no sleep problems had the highest TFLS scores, and their scores were significantly higher compared to scores of participants who reported not exercising and endorsed sleep concerns. Participants who endorsed only one positive health factor (e.g., exercising regularly or no sleep concerns) were not significantly different from one another (or from any other group) and received scores that were between the groups endorsing both or no health factors. Descriptive statistics for these exploratory comparisons are presented in Table 4. Graphic representation of TFLS scores based on self-reported exercise habits and sleep complaints can be found in Figure 2.

TFLS total scores based on self-reported exercise habits and sleep complaints. Note. TFLS = Texas Functional Living Scale. Higher scores represent better functional capacity. Error bars represent standard error.
Discussion
Results of the present study revealed statistically significant differences in cognitive functioning and functional capacity based on exercise habits and sleep concerns. Specifically, participants who reported exercising regularly, as well as those who reported the absence of sleep problems, displayed better scores on tests of global cognitive functioning and functional abilities. Additionally, follow-up analyses demonstrated that participants who score better on multiple measures of well-being (e.g., those who report both good sleep quality and regular exercise) perform better on neurocognitive tests and measures of functional capacity as compared to those who do not engage in health-promoting behaviors.
Present findings are consistent with previous research suggesting that exercise is associated with better cognition and functional capacity in older adults (e.g., Paterson & Warburton, 2010). However, the question regarding what entails optimal frequency and duration of physical activity continues to remain a topic of debate (de Souto Barreto et al., 2016; Geda et al., 2010; Hoffmann et al., 2016; Northey et al., 2018; Rathore & Lom, 2017; Sofi et al., 2011). Previously published research has demonstrated a dose-response relationship between exercise and cognitive function (de Souto Barreto et al., 2016; Hoffmann et al., 2016; Ludyga et al., 2020). For example, Ludyga et al. (2020) completed a meta-regression of 80 randomized control trials and found that effect sizes increased with longer intervention length and session duration. Additionally, Hoffmann et al. (2016) conducted a randomized control trial of 200 patients with mild Alzheimer’s Disease (AD) and found that patients who exercised with high attendance and intensity had better cognitive functioning. Some studies reveal that exercise of moderate intensity and duration may provide the most benefits to cognition (Northey et al., 2018), whereas other research indicates that even low frequency of physical activity (e.g., several times per month) has been associated with better cognition in aging (de Souto Barreto et al., 2016). Some authors report protective effects of all levels of exercise (low, moderate, and high) against cognitive impairment (Sofi et al., 2011).
Extant research involving functional capacity presents similar challenges for developing specific recommendations for exercise. For example, a meta-analysis by Paterson and Warburton (2010) demonstrated that both aerobic and resistance-training interventions improved physiological and functional abilities in older adults. Further, both moderate and high levels of exercise have been shown to reduce disability, with a dose-response relationship between more complex functioning and exercise intensity. While the authors concluded that recommendations for minimal activity are difficult to provide, it is well established that at least a moderate level of activity offers protective benefits (Paterson & Warburton, 2010). Although the ability to make specific recommendations to patients regarding activity type and intensity is yet to be developed, healthcare providers may consider discussing with their patients participation in a variety of physical exercises that would be safe, enjoyable, and practical to engage in regularly. Of note, the importance of interventions focused on the improvement of functional capacity in older adults has received emerging recognition in recent years. For example, the American Heart Association (Forman et al., 2017) issued a scientific statement for healthcare professionals emphasizing the crucial role that functional outcomes ought to play in designing various therapies for older adults with chronic health conditions (such as cardiovascular disease). Forman et al. (2017) recommended that exercise intervention programs for older adults should be designed specifically with an emphasis on the capacity to perform ADLs, maintain independence, and optimize quality of life.
Regarding sleep quality, results of the present study revealed that participants who endorsed sleep concerns had lower scores on neuropsychological tests and assessments of functional capacity, as compared to those who endorsed no sleep problems. These findings are also in line with published research indicating that sleep problems have been associated with poorer functional capacity (Brimah et al., 2013; Chien & Chen, 2015; Vincent et al., 2021) and worse cognitive functioning (Ju et al., 2014; Kronholm et al., 2009; Potvin et al., 2012; Yaffe et al., 2014) in older age. Additionally, extant studies have suggested that sleep problems may be related to processes that age the brain and may result in brain atrophy and progression of cognitive impairment (Sexton et al., 2014; Yaffe et al., 2014). It is not yet clear from extant literature whether poor sleep quality leads to cognitive impairment or whether it is one of the associated features of cognitive decline (Ju et al., 2014), but addressing sleep concerns may be one of potential intervention targets for improving cognition and functional capacity. Of course, no causal conclusions or statements regarding the directionality of the observed relationships can be made based on the cross-sectional design of the present study, but further research examining sleep quality and changes in cognition and functional abilities over time may be beneficial to provide further understanding of the nature of these relationships.
Results of the present study also demonstrated that participants with multiple risk factors (lack of exercise and significant sleep concerns) displayed significantly lower scores on cognitive tests and measures of adaptive functioning, whereas those who reported no sleep concerns and regular exercise scored significantly higher on all measures (as compared to the group with multiple risk factors). Thus, the results point to a potential compounding effect of multiple protective factors, which is consistent with extant literature as well (Karssemeijer et al., 2017; Kesse-Guyot et al., 2014). Some investigators have proposed that monotherapies or interventions aimed at only one risk factor may be not as effective in addressing cognitive decline as comprehensive therapeutic programs. For example, Bredesen (2014) conducted a pilot study of personalized interventions for patients with varying levels of cognitive impairment and demonstrated sustained and marked improvements in cognition in 90% of patients who adhered to the program. Interventions tailored to each patient included improvements in sleep quality, increase in exercise, and stress reduction, among others (Bredesen, 2014). Furthermore, published research has indicated that physical activity may improve sleep quality and attenuate deficits in IADLs in older adults with neurological disorders, such as Alzheimer’s disease (Nascimento et al., 2014). Conversely, other studies have demonstrated that sleep disturbance may be associated with limitations in physical activity and IADL impairment (Loh et al., 2017), indicating that perhaps one risk factor (e.g., lack of physical activity or sleep disturbance) may exacerbate another one, and together the combination of these factors may result in poorer functional and cognitive outcomes. Thus, findings of published research and of the present study suggest that further investigations of combined interventions and the directionality of the relationship between multiple lifestyle factors are needed.
Overall, the current study highlights the need for additional research examining which lifestyle interventions are especially salient for people with and without genetic predispositions to develop cognitive impairment and subsequent functional impairment. For example, while existing research indicates that exercise has benefits for long-term cognitive health and functional ability, future research may focus on exploring specific types, frequency, and intensity of physical exercises that provide optimal benefit. Additionally, it would be of interest to conduct longitudinal studies to investigate whether physical exercise delays the onset of cognitive decline and functional impairment or slows down their progression. Finally, sleep quality can also be assessed in a more comprehensive manner in future research that may examine the links between cognition, functional capacity, and sleep quality, total sleep duration, uninterrupted sleep duration, as well as associated sleep disorders (e.g., sleep apnea). Clinicians (e.g., physicians, psychologists, neuropsychologists, nurses, and other healthcare providers) may also consider including a more thorough examination of lifestyle factors into their assessments as well as a more comprehensive discussion of these factors in their clinical recommendations, given the associations with better cognition and functional capacity found in the current study.
As previously mentioned, it is likely that impaired cognitive function and functional disability may present as comorbidities (e.g., De Vriendt et al., 2012). Additionally, deficits in functional capacity may be indicative of cognitive impairment in older adults (Ord et al., 2019), and impairment in complex functional capacity may predict progression of mild cognitive impairment to dementia as early as 2 years before diagnosis (Cloutier et al., 2021). Thus, functional capacity may represent an area for early assessment and intervention in improving overall quality of life and ability to maintain independence in the context of cognitive decline. Evidence that the same lifestyle interventions may improve both domains (cognition and functional capacity) underscores the importance of assessing lifestyle factors when providing treatment recommendations (Vreugdenhil et al., 2012). Additionally, patients with higher baseline functioning and more improvements in functional ability following intervention have demonstrated a greater ability to adhere to treatment recommendations for cognitive impairment (Amofa et al., 2020). Thus, improvements in functional ability may result in higher effectiveness of interventions aimed at addressing cognitive impairment.
The present study is not without limitations that should be considered when evaluating the findings. First, utilizing self-reported and dichotomized data to assess lifestyle factors presents several limitations: limited variability as a consequence of a restricted range, potential problems with replicability of the findings, inability to fully account for type and frequency of exercise, and inability to comprehensively evaluate the extent of sleep concerns. Second, the definitions of optimal health as well as a healthy lifestyle differ significantly from person to person. While the scientific community has developed overarching recommendations, it is important to take into consideration individual differences, given the self-report nature of utilized data. Future studies should include more comprehensive and validated assessments of health behaviors. Third, the range of cognitive functioning in the present study was somewhat restricted due to the outpatient nature of the neuropsychological assessment in a clinical setting (cognitive functioning was in the normal to mildly impaired range for most participants). Future studies may include participants with lower levels of cognition to further investigate group differences in cognitive functioning and functional capacity based on lifestyle factors. Finally, effect sizes observed in the present study were in the small-to-medium range, indicating that after adjustment for age, education, and health status, differences in cognitive functioning and functional capacity based on lifestyle factors were rather modest. Therefore, findings need to be interpreted in light of the limited magnitude of effect sizes and further research is needed to investigate whether a difference of several points on objective measures of cognition and functional living may in fact translate to measurable variability in functional independence and quality of life in older adulthood.
Conclusions
Overall, results of the present study suggest that lifestyle factors (such as exercise and sleep quality) are associated with objective performance on tests of neuropsychological functioning and functional abilities. Moreover, addressing several lifestyle factors may have a positive synergistic effect on cognition, as participants engaging in several health-promoting behaviors (e.g., regular exercise and healthy sleep) displayed the highest levels of cognitive and adaptive functioning. Results of the present study preclude any conclusions regarding the causality of the observed relationships due to the cross-sectional design. Nevertheless, these findings may assist in the development of treatment recommendations for individuals seeking to maintain cognitive functioning or attenuate cognitive decline. Further research examining the relationship between lifestyle factors and brain health is needed.
Footnotes
Acknowledgments
Writing of this manuscript was supported by the Department of Veterans Affairs Office of Academic Affiliations Advanced Fellowship Program in Mental Illness Research and Treatment, the Research & Academic Affairs Service Line, Salisbury VA Medical Center, Salisbury, North Carolina, and the Department of Veterans Affairs Mid-Atlantic (VISN 6) Mental Illness Research, Education, and Clinical Center (MIRECC).
Authors’ note
The views, opinions and/or findings contained in this article are those of the authors and should not be construed as an official Regent University, US Department of Veterans Affairs or US Department of Defense position, policy or decision, unless so designated by other official documentation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received no specific grant or financial support from any funding agency in the public, commercial, or not-for-profit sectors.
Author Biographies