
Abstract
The objective of this study is to test self-efficacy as a mediator in the relationship between three lifestyle activities (exercise, volunteering, and computer use) and self-perceptions of aging (SPA) among older adults. We hypothesize that increased self-efficacy will mediate the relationship between lifestyle activities and more positive SPA. This is a cross-sectional, secondary data analysis drawn from the 2016 wave of the Health and Retirement Study (HRS; n = 4,561). Bootstrapping procedures were applied to test the significance of the indirect effects of self-efficacy in the relationship between lifestyle activities and SPA. Results indicate significant direct effects between exercise, computer use, and self-efficacy. Direct effects were observed between exercise, volunteering, computer use, and SPA. Self-efficacy partially mediated the relationship between exercise, volunteering, computer use, and SPA. Implications for practitioners working with older adults are discussed. Future research should test formal intervention programs aimed at reducing internalized ageism through additional pathways.
Ageism is a prevalent, largely unchallenged form of discrimination in Western society (Nelson, 2002; Palmore, 1999). The term signifies any bias, stereotype, prejudice, or discrimination toward an individual based solely on that person’s age (Nelson, 2002). A unique quality of ageism is that old age is something all people will experience given a long life. In fact, ageism has been described as a “prejudice against our feared future self” (Nelson, 2005, p. 207). Therefore, the internalization of ageism is critical to understanding this issue.
A growing body of research demonstrates that internalized age stereotypes have significant associations with numerous public health outcomes, including longevity (Levy et al., 2002), physical functioning (Levy, Pilver, Chung, et al., 2014), mental health concerns (Levy, Pilver, & Pietrzak, 2014), cardiovascular events (Levy et al., 2000), cognitive decline (Levy et al., 2018), and likelihood of recovery from disability (Levy et al., 2012). These outcomes are described as having accumulated impacts across the lifespan (Levy, 2009).
While the literature documents public health impacts of internalized ageism, limited research exists about activities which may reduce internalized ageism because this construct has most often been studied as an independent, rather than dependent, variable. It remains unknown what types of social engagement, lifestyle behaviors, or other activities may be effective in reducing internalized ageism, in turn promoting positive health outcomes for older adults.
Background
Theoretical Framing
The present study is guided by stereotype embodiment theory (SET) and successful aging. SET is a useful theory for conceptualizing how internalized ageism affects older adults. Levy describes how this theory “has four components: The stereotypes (a) become internalized across the lifespan, (b) can operate unconsciously, (c) gain salience from self-relevance, and (d) utilize multiple pathways” (Levy, 2009, p. 332). In terms of the utilization of multiple pathways, Levy describes three primary pathways of age stereotypes: psychological, behavioral, and physiological. The present study applies SET’s application of the psychological pathway in particular due to self-efficacy being tested as a mediator. SET posits that older adults may not engage in healthy lifestyle behaviors because they may assume these are not worth the effort. Therefore, the current study also applies successful aging through its focus on the benefits of healthy lifestyle behaviors and active engagement with life (Rowe & Kahn, 1998, p. 38).
SET postulates that three distinct yet related constructs influence pathways towards health outcomes: age discrimination, age stereotypes, and self-perceptions of aging (SPA; Levy, 2009). SPA is a common variable in literature operationalizing the individual, internalized impacts of ageism (Chang et al., 2020). Therefore, SPA has been selected as the dependent variable within the present study.
Self-Efficacy
Self-efficacy is defined as “how well one can execute courses of action required to deal with prospective situations” (Bandura, 1982, p. 122). Self-efficacy acts as a potential mediator in the relationship between lifestyle or social participation activities and SPA. One systematic review finds that self-efficacy plays a mediating role in the relationship between ageism and health (Chang et al., 2020). In particular, research indicates that self-efficacy mediates the relationship between SPA and physical functioning (Tovel et al., 2017), SPA and healthy eating Klusmann et al. (2019), as well as stereotypic beliefs about aging and health-promoting behaviors (Yeom, 2014). A recent factor analysis with a sample of Korean older adults describes the following dimensions of self-efficacy: competence and social self-efficacy, including both internal and interactive forms of social self-efficacy (Hur, 2018).
Exercise, Volunteerism, Computer Use, and Self-Efficacy Among Older Adults
A preliminary literature documents the relationship between lifestyle or social participation activities and self-efficacy. In particular, exercise, volunteering, and computer use are three activities which may influence older adults’ self-efficacy. A large review of systematic reviews finds self-efficacy to be one of the most consistent predictors of physical activity for adults (Bauman et al., 2012). Physical activity is also shown to have a strong effect on self-efficacy, while self-efficacy mediates the relationship between physical activity and quality of life for older adults (Mudrak et al., 2016). Direct effects between walking and self-efficacy are documented, in addition to indirect effects between walking and functional limitations through the mediating path of self-efficacy (Mullen et al., 2012).
Self-efficacy also plays a prominent role in research on volunteerism (Kossowska & Łaguna, 2018; Wang et al., 2011). In particular, studies indicate that volunteering increases self-efficacy for middle-aged and older adults (Brown et al., 2012). A study with Korean older adults indicates a strong association between volunteering and a sense of “inward social self-efficacy” (Hur, 2018, p. 295). Volunteers for caregivers of people with dementia are shown to have fairly high levels of self-efficacy, potentially leading to increased health service use and overall well-being (Charlesworth et al., 2017). Additionally, self-efficacy serves a mediator in the relationships between personality and volunteer engagement (Kossowska & Łaguna, 2018), between organizational environment and volunteer intention (Wang et al., 2011), and between volunteering and well-being (Brown et al., 2012).
A growing literature also describes the impact of computer use on self-efficacy among older adults. For example, older adults demonstrate increased computer self-efficacy when using online health information (Hall et al., 2015). A recent qualitative study describes self-efficacy as a theme as it relates to technology use in general, in addition to being an outcome of technology use among older adult veterans (Leone et al., 2018). Furthermore, a recent factor analysis finds that older adults’ perception of their computer role and time on the internet are significant predictors of self-efficacy (Zheng et al., 2015).
Study Aim and Hypothesis
The purpose of this study is to explore a topic which, to our knowledge, has yet to receive attention in the literature: lifestyle activities to reduce internalized ageism operationalized by SPA. Currently, there is limited research discussing both the influence of SPA on self-efficacy and self-efficacy on SPA. While preliminary literature demonstrates the effects of volunteering, exercise, and computer use on self-efficacy, a paucity of research explores the relationship between lifestyle or social participation activities and SPA. SPA is selected as the dependent variable in the present study given its application in SET and potential influence on health outcomes for older adults.
Despite current gaps in the literature, SET and successful aging point towards healthy lifestyle behaviors being one potential factor which may improve SPA for older adults. The reviewed literature also supports self-efficacy as a potential mediator within this relationship. Synthesizing the literature review with relevant theoretical frameworks, the aim of the present study is to test the influence of self-efficacy as a mediator in the relationship between three activities (exercise, volunteering, and computer use) and SPA among older adults 50 + years of age. We hypothesize that increased self-efficacy will mediate the relationship between these activities (exercise, volunteering, and computer use) and more positive SPA.
Methods
Data Source
This is a secondary data analysis drawn from the Health and Retirement Study (HRS), a biannual, nationally representative survey of adults 50 + years of age and their spouses of any age (Heeringa & Connor, 1995). The HRS receives support from the National Institute of Aging (U01AG009740) and the Social Security Administration. This study incorporates a multi-stage, area-clustered, stratified sample design which includes an oversampling of African American and Hispanic older adults, as well as Florida households (Ofstedal et al., 2011). The HRS is approved by the University of Michigan Institutional Review Board.
This study utilizes data from the 2016 wave of the HRS. The core HRS survey gathers information on income, work, assets, health, and disability collected either through an in-person or phone interview. A total of 20,912 respondents completed the core survey during the 2016 wave of the HRS (response rate = 84.38%). Data for this study are drawn primarily from respondent level data on the leave-behind questionnaire, which assesses measures of psychosocial well-being, including self-efficacy and SPA, as well as frequency of involvement in 21 social participation activities. Respondent level data come from the respondents or their proxy when respondents are unable to complete an interview. The leave-behind questionnaire is self-administered by a rotating half of the sample every 4 years after completion of the core survey. 10,238 participants were eligible and 6,370 completed the leave-behind questionnaire in 2016 (response rate = 62.22%). Response rates for the leave-behind questionnaire are likely lower because this questionnaire is self-administered after the core survey and returned by respondents via mail.
Measures
Self-Perceptions of Aging (SPA)
Eight items measure respondents’ positive (four items) and negative (four items) SPA. Five of the eight items are drawn from the Attitudes Toward Own Aging subscale of the Philadelphia Geriatric Center Moral Scale (Lawton, 1975; Liang & Bollen, 1983; Smith et al., 2017). Three items were added from the Berlin Aging Study to increase the reliability of a unidimensional scale (Kotter-Grühn et al., 2009; Smith et al., 2017). Examples of positive items include “I am as happy now as when I was younger” and “So far, I am satisfied with the way that I am aging.” Examples of negative items include “The older I get, the more useless I feel” and “Getting older has brought with it many things that I do not like.” We reverse coded the four negative items to create an eight-item unidimensional positive scale. Items are measured on a six-point Likert-type scale (1 = Strongly disagree to 6 = Strongly agree). We created a mean score variable to measure SPA through one item (M = 3.93, SD = 1.04, and α = .82), with a higher score indicating more positive SPA.
Self-Efficacy
A variety of terms are used for self-efficacy, including “personal sense of control…self-efficacy…agency…mastery” (Smith et al., 2017, p. 28). Five items measure respondents’ perceived mastery (Lachman & Weaver, 1998; Pearlin & Schooler, 1978). The five items state: “I can do just about anything I really set my mind to,” “When I really want to do something, I usually find a way to succeed at it,” “Whether or not I am able to get what I want is in my own hands,” “What happens to me in the future mostly depends on me,” and “I can do the things that I want to do.” Items are coded on a six-point Likert-type scale (1 = Strongly disagree to 6 = Strongly agree). We created a mean score variable to measure self-efficacy through one item (M = 4.81, SD = 1.08, and α = .90), with a higher score indicating greater self-efficacy.
Social Participation/Lifestyle Activities (Exercise, Volunteering, Computer Use)
The leave behind questionnaire includes 21 items which measure frequency of participation in a wide variety of social participation and lifestyle activities (adapted from Hultsch et al., 1999; Jopp & Hertzog, 2010; Parslow et al., 2006; Salthouse et al., 2002). These activities include caregiving, intergenerational family or neighborhood activities, volunteering with children or youth, other volunteer/charity work, attending an educational or training course, going to a sports or social club, attending non-religious organizational meetings, private prayer, reading, watching television, doing word games, playing cards or games, writing, using a computer, doing home/car maintenance or gardening, baking/cooking, making clothes or knitting/embroidery, working on a hobby or project, playing sports or exercise, walking for 20 minutes or more, and participating in a local community arts group (Smith et al., 2017, p. 16–17). These items ask participants how often they do each activity and are measured on a seven-point Likert-type scale (1 = Daily to 7 = Never/Not Relevant). We reverse coded the items so that higher values represent greater frequency of participation. For exercise, we combined two items: how often respondents “play sports or exercise” and how often respondents “walk for 20 minutes or more.” For volunteering, we also combined two items: how often respondents “do volunteer work with children or young people” and how often respondents “do any other volunteer or charity work.” We created a mean score variable to measure exercise (M = 4.11, SD = 1.92, and α = .67) and volunteering (M = 1.94, SD = 1.20, and α = .60) through one item. The item for computer use asks respondents how often they “use a computer for email, Internet, or other tasks” (M = 5.14, SD = 2.54).
Demographic Variables and Other Covariates
The following covariates are collected through self-report: Age in 2016, sex (0 = female, 1 = male), education (0 = less than high school, 1 = high school or above, including GED), race/ethnicity (0 = White, 1 = Black/African American), Hispanic or Latino ethnicity (0 = no, 1 = yes), functional limitation (0 = no difficulty, 1 = any difficulty as it relates to instrumental activities of daily living across the following five items: using a telephone, taking medication, managing money, shopping, and preparing meals), self-rated health on a five-point scale (1 = excellent to 5 = poor), and a combined variable of the number of friends and family other than one’s spouse whom the respondent considers to be a “close relationship.”
Statistical Analysis
We used the RAND longitudinal file, a user-friendly file drawn from all HRS waves with cleaned and processed variables. Variables of interest had less than 2.2% missing; therefore, we used listwise deletion to account for missing data. Analyses were conducted using the Statistical Package for the Social Sciences (SPSS) version 26.0. First, we conducted descriptive statistics and bivariate correlations across all variables.
We applied the Hayes PROCESS macro in SPSS (Hayes, 2018) to test our hypothesis that increased self-efficacy would mediate the relationship between three activities (exercise, volunteering, and computer use) and more positive SPA while holding constant all covariates. The following set of regressions were conducted: (1) the dependent variable (SPA) was regressed on each of the three independent variables (exercise, volunteering, and computer use), (2) the mediator (self-efficacy) was regressed on the three independent variables (exercise, volunteering, and computer use), and (3) the dependent variable (SPA) was regressed on the mediator (self-efficacy). The above three steps were conducted while holding constant all covariates.
Indirect (mediation) effects were conducted by using bootstrapping procedures (Hayes, 2018). Unstandardized indirect effects for 5,000 bootstrapped samples were computed to test the significance of indirect effects. Confidence intervals were set at the 95% level. This process provides an approximation of the sampling distribution of the indirect effects. The indirect effects are interpreted as significant in cases where the 95% confidence interval does not contain zero (Shrout & Bolger, 2002).
Results
Sample characteristics and bivariate correlations across all variables are presented in Table 1. This cross-sectional sample is comprised of 4,561 participants with an average age of 67.66 (SD = 10.62) and more female (60.32%) than male (39.68%) respondents. 80.8% of the sample identify as White, 19.21% identify as Black/African American, and 7.27% identify as Hispanic or Latino. 89% of the sample has a high school education or higher. Respondents report experiencing functional limitation on 20% of items measuring independent activities of daily living (IADL’s), with a relatively large standard deviation across responses (SD = .64). On average, participants report “good” health and having close to four friends or family members other than one’s spouse they would consider a “close relationship.”
Sample Characteristics and Bivariate Correlations (N = 4,561)

Note. *p < .05; **p < .01; 0 = "no," 1 = "yes"
Participants’ mean score of 3.93 for SPA is close to an average response option of “slightly agree,” signifying that overall SPA for this sample is slightly positive but less positive than “somewhat” or “strongly agree” options. The mean value of 4.81 for self-efficacy is closest to the response that participants “somewhat agree” with positive items related to self-efficacy. The mean score of 4.11 for exercise indicates that participants exercise, on average, “several times a month.” The mean score of 1.94 for volunteering means that participants, on average, report volunteering less frequently than once per month. The mean score of 5.14 for computer use demonstrates that, on average, participants use a computer “once a week.” Significant correlations (p < .01) are observed between each of the three independent variables (exercise, volunteering, and computer use), the mediator (self-efficacy), and the dependent variable (SPA).
Table 2 details the results of the regression analyses while holding constant all covariates. Results are organized with self-efficacy as the dependent variable in model 1: F(11, 4549) =35.43, p < .001, R2 = .08, followed by SPA as the dependent variable in model 2: F(12, 4548) =154.89, p < .001, R2 = .29). Significant direct effects are observed between exercise and self-efficacy (β = .07, p < .001), as well as between computer use and self-efficacy (β = .03, p < .001), but not between volunteering and self-efficacy (β = −.001, p = .96). Results indicate significant direct effects between exercise and SPA (β = .11, p < .001), volunteering and SPA (β = .04, p < .001), and computer use and SPA (β = .02, p < .001). A significant direct effect is also observed between self-efficacy and SPA (β = .34, p < .001). Model 1 explains 8% of the variance in self-efficacy, while Model 2 explains 29% of the variance in SPA.
Regression Results Predicting Self-Efficacy and Self-Perceptions of Aging (N = 4,561)
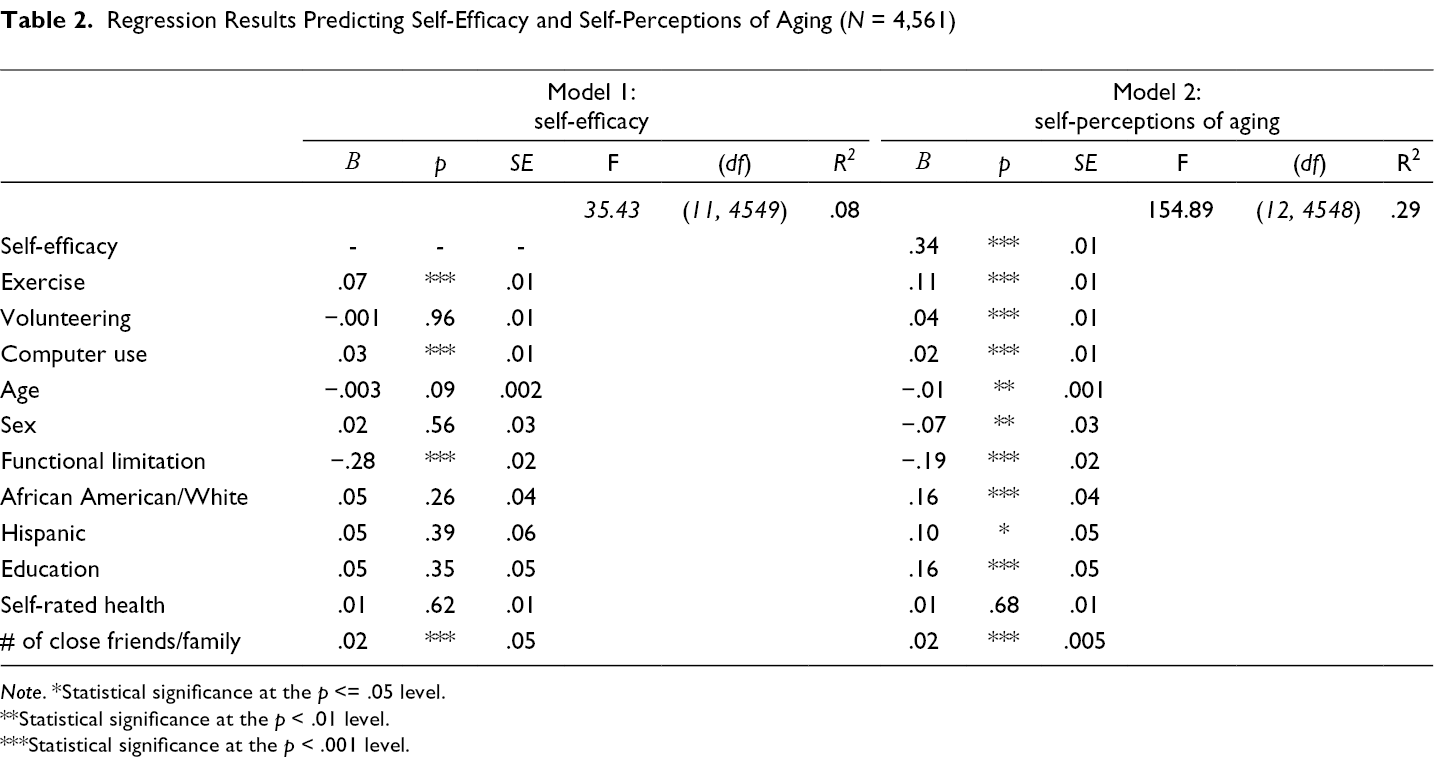
Note. *Statistical significance at the p <= .05 level.
**Statistical significance at the p < .01 level.
***Statistical significance at the p < .001 level.
Figure 1 depicts the mediation model. The results indicate that self-efficacy partially mediates the relationship between the three independent variables (exercise, volunteering, and computer use) and SPA. Bootstrap estimates and 95% confidence intervals suggest that the indirect effect is statistically significant, β = .02, (.02; .03).
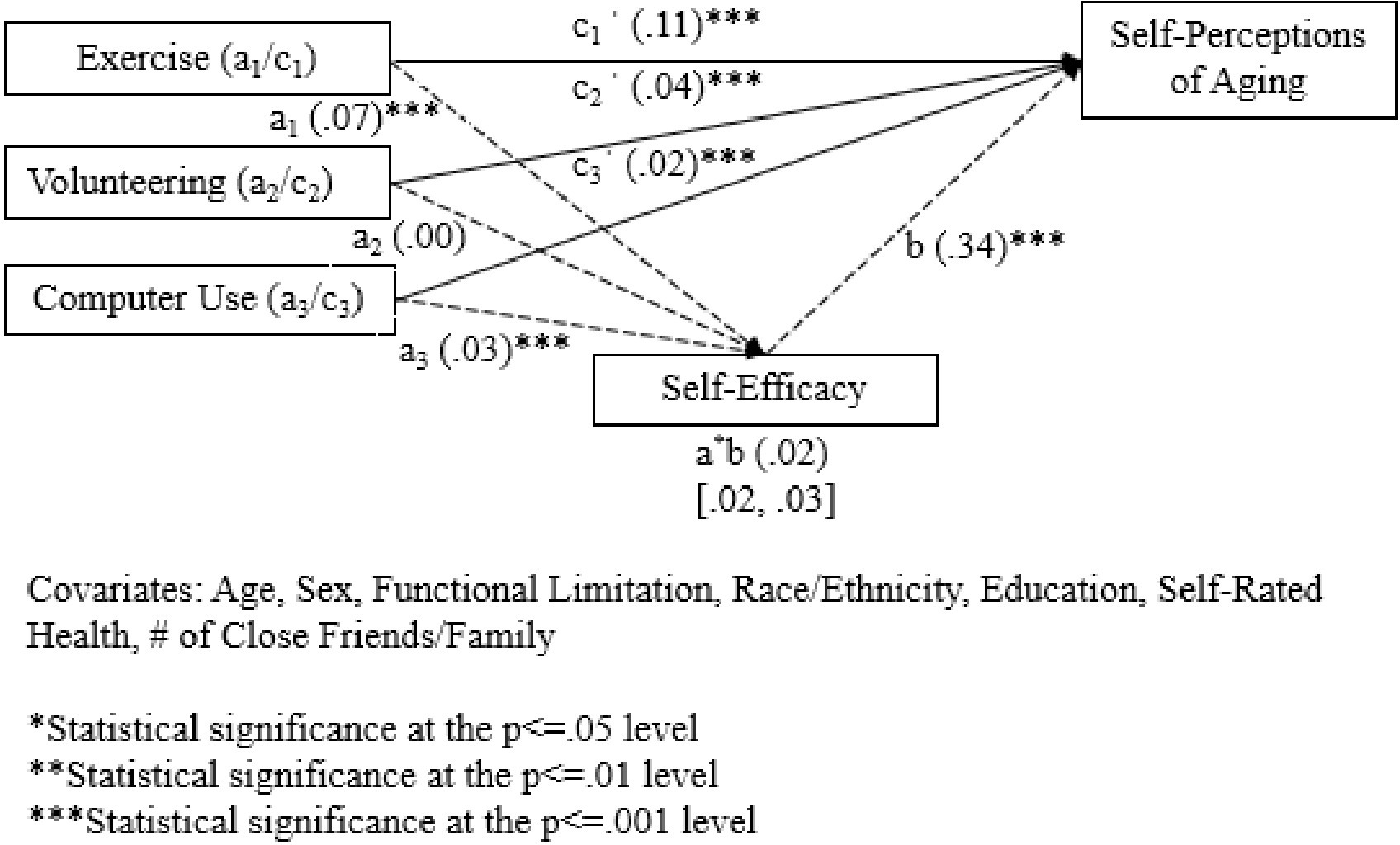
A mediation model of the independent variables (exercise, volunteering, and computer use) on the dependent variable (self-perceptions of aging) through the mediator of self-efficacy. a represents the direct effect of each of the independent variables on self-efficacy, b represents the direct effect of self-efficacy on self-perceptions of aging, and c· represents the direct effect of each of the independent variables on self-perceptions of aging, while holding constant relevant covariates. For a and c direct effects, exercise is denoted by a1/c1 volunteering by a2/c2, and computer use by a3/c3-,. a*b represents the indirect effect of the independent variables on the dependent variable through the mediator of self-efficacy.
Discussion
This study offers novel evidence about lifestyle activities which may help older adults improve their SPA through the mediating mechanism of self-efficacy. Therefore, this article contributes toward a burgeoning area of scholarship in terms of what can be done to improve SPA. The current state of literature on SPA and other operationalized constructs of internalized ageism (such as internalized age stereotypes) are primed for new research to examine interventions and mediating pathways which may reduce the known public health impacts of internalized ageism.
Findings from this study indicate significant direct effects between exercise, volunteering, and computer use on SPA. These findings are not surprising given the wide range of benefits already associated with these activities in the literature (Chu et al., 2009; Morrow-Howell et al., 2003; Rowe & Kahn, 1998). The non-significant direct effect between volunteering and self-efficacy is not consistent with the literature. However, our study’s participants had relatively low levels of volunteer activity, and future research should address this study’s research question with a more formal volunteer intervention.
Our finding that self-efficacy partially mediates the relationship between exercise, volunteering, computer use and SPA provides valuable information about one mechanism which may help improve how older adults feel about their own aging. Mediating mechanisms to reduce constructs of internalized ageism (such as SPA) may be particularly useful for scholars and practitioners due to the inherent challenges of influencing changes at an internalized level. The mediation results are also encouraging given the robust knowledge-base already established related to self-efficacy. Therefore, scholars may wish to pursue similar studies with additional independent variables of interest known to influence self-efficacy in older adults. Potential examples include memory-building activities (Beaudoin & Desrichard, 2017), mind-body interventions (Scult et al., 2015), and more specific exercise interventions such as Tai Chi (Tong et al., 2018).
Our results are in line, broadly speaking, with existing literature which suggests the potential mediating role of self-efficacy. However, there is much room for further scholarly exploration in this area. For example, a recent study found that negative SPA led to decreased control of life (a construct similar to self-efficacy), while low levels of control of life also led to increased SPA after a 4 year period (Luo et al., 2020). However, another study showing that self-efficacy mediates the relationship between SPA and physical functioning also found that SPA affects physical functioning, but physical functioning does not significantly affect SPA (Tovel et al., 2017). Research exploring the influence of self-efficacy on SPA, and in particular the mediating effect of self-efficacy on SPA, is still quite limited. This points towards the importance of continued research on the mediating role of self-efficacy as well as other potential mechanisms which may influence SPA for older adults.
Additionally, it is important to note that the mediation effects observed within this study were fairly small (i.e., the indirect effect of self-efficacy was .02). Given the robustness of Bandura’s work on self-efficacy and indications from the literature about the mediating role of self-efficacy between ageism and health (Chang et al., 2020; Klusmann et al., 2019; Levy et al., 2000; Tovel et al., 2017), self-efficacy should continue to be explored as a mediating mechanism in future studies. However, scholars may also want to pursue studies testing different potential mediators. Given the fact that little scholarship has explored mediating mechanisms with SPA as a dependent variable, it would certainly be worth exploring whether additional mediators shown to influence perceived well-being or constructs similar to SPA may also influence older adults’ SPA. For example, one recent study found that purpose in life and perceived social status mediated the relationship between volunteering and depressive symptoms (Yang & Matz, 2020). Furthermore, gratitude has been shown to mediate the relationship between contemplating life lessons and positive attitudes toward aging (Bryant et al., 2021). Therefore, purpose in life, perceived social status, and gratitude are just a few additional mediators worth exploring in research aiming to better understand pathways toward enhancing SPA for older adults.
Furthermore, despite the precedence and robust evidence surrounding the successful aging literature (Rowe & Kahn, 1998), it is possible that lifestyle activities alone may not be the most effective intervention in influencing older adults’ internalized ageism as measured by SPA. For example, a recent meta-analysis and systematic review found that interventions which combined both intergenerational contact and education were more effective in reducing ageism in general than either of these interventions on their own (Burnes et al., 2019). Therefore, in designing organized interventions to reduce internalized ageism, scholars and program developers should consider incorporating intentional education about ageism and positive perspectives on aging along with lifestyle activities. One program that has successfully incorporated education is the Frameworks Institute (https://www.frameworksinstitute.org), which has developed educational, narrative interventions to reframe how people think about aging and impact a variety of ageism-related outcomes (e.g., attitudes toward aging, collective efficacy toward aging, implicit age bias, us vs. them thinking, knowledge of systemic aging supports, etc.) (Busso et al., 2019; Sweetland et al., 2017). Such efforts could be combined with lifestyle programming for older adults to test whether effects on SPA would be more robust than in the present study.
Limitations
Despite the strengths of this study in terms of its novelty, use of theory, and the positive implication that certain lifestyle activities may help improve SPA, there are some limitations which are important to note. First, the measurement of exercise, volunteering, and computer use is somewhat simplified, with exercise and volunteering measured by two items and computer use only one item as part of the HRS leave-behind questionnaire. Future research should incorporate more formal, organized intervention studies clearly focused on these lifestyle activities. The present study was limited by incorporating items from a much larger survey in which these activities were not the primary focus.
Another limitation of this study is the cross-sectional design, which precludes the ability to make claims of causality about the results. As important as mediation effects are, the results of this study should be viewed with caution at this time due to the lack of temporal precedence in this analysis. Additionally, the lack of randomization or use of a control group further affects the internal validity of this study. Both the cross-sectional design and lack of randomization make it quite difficult to parse out whether the lifestyle activities analyzed in this study would truly account for changes in self-efficacy or SPA. Furthermore, the statistically significant findings may be related to the relatively large sample size. However, we did conduct post-hoc analyses with smaller subsamples based on age (i.e., ages 50–59, 60–60, 70–79, and 80+), and the results were consistent with the overall findings presented within this study.
Within this conversation, it is also important to note critical equity gaps to participation in the lifestyle activities tested in this study. A long-standing critique of successful aging has been its focus on individual-level lifestyle behaviors such as exercise, diet, or smoking (Franklin & Tate, 2009; Katz & Calasanti, 2015) and relative inattention to structural inequities and health disparities (Katz & Calasanti, 2015). Specific to volunteering, inequity in volunteer engagement based on race/ethnicity (Tang et al., 2012) and challenges of volunteer recruitment for low-SES adults due to barriers such as transportation, poor health, and the dual demands of caregiving (McBride, 2007; Morrow-Howell et al., 2009) have been identified. In terms of computer use, the Pew Research Center found that men, adults over age 65, and individuals with less education are less likely to search online for health information specifically (Fox, 2008). One study also found health literacy and health numeracy to be barriers in the use and access of internet technology for low-income adults (Jensen et al., 2010). Therefore, while the present study provides hopeful avenues for improving SPA in older adults, the results need to be viewed within context and also acknowledge structural barriers and inequitable access to such activities for marginalized communities. Furthermore, it is possible that theoretical frameworks other than SET may be necessary for scholars to pursue structural-level interventions to reduce internalized ageism.
Conclusion
Despite these limitations, the present study is to our knowledge the first to show that lifestyle activities may influence SPA for older adults through the mediating role of self-efficacy. The findings offer positive implications about the effects of exercise, volunteering, and computer use among older adults. The results make sense in light of strong theoretical and evidentiary support from the successful aging literature (Mudrak et al., 2016; Rowe & Kahn, 1998). However, given the limited amount of literature with SPA as a dependent variable and self-efficacy as a mediator, as well as the small indirect effects found in this study, future research should continue to explore to what extent these and other lifestyle activities, within the context of structural-level factors, may influence self-efficacy and other mediating mechanisms to enhance SPA for older adults.
Ageism is a powerful force which is internalized and has accumulated health impacts across the lifespan according to SET (Levy, 2009). Stigma and fears related to the aging process are powerful, but the results of this study support the need to continue bolstering programming related to exercise, volunteering, and computer use for older adults. Additionally, practitioners who work individually with older adults struggling with changes related to the aging process may want to encourage clients to pursue these activities. The results from this study indicate that these activities may be one means of combatting the powerful force of ageism, which is unconsciously internalized and associated with numerous negative health outcomes across the lifespan (Levy, 2009).
The present study is strongly informed by SET, and this theory also paves the way for how future studies may wish to evaluate efforts to improve SPA for older adults. This study focuses on testing the psychological pathway within SET in particular. Yet, SET suggests additional pathways future research may focus on: namely, the behavioral and physiological pathways. As one example within the behavioral pathway, future researchers could test physical activity as a mediator by exploring whether intergenerational programming increases physical activity for older adults, which may in turn enhance SPA. Within the physiological pathway, future studies could explore whether mindfulness decreases physiological stress, which in turn may contribute to more positive SPA. Many promising paths forward are possible for improving how adults feel about their own aging through an integration of SET with successful aging.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies