
Abstract
Although stress due to racial and ethnic differences can negatively impact life satisfaction, there is a lack of focus on the differences between minority and nonminority older adults in how stress and coping skills impact life satisfaction. The objectives of this study are to explore (a) the differences between minority and nonminority older adults in their levels of life satisfaction, stress, and coping skills; and (b) the mediating effects of coping skills on the relationship between perceived stress and life satisfaction among both groups. Cross-sectional data from the Well Elderly 2 study (N = 460) were utilized in bivariate and mediation analyses. Minority older adults reported higher levels of stress and prioritized different coping skills. Mediation was not supported for either group. These findings enable practitioners to focus on the coping skills more frequently identified by clients’ racial/ethnic grouping, as well as to target the primary stressors identified.
Introduction
The life satisfaction of older adults is worthy of specific attention due to not only the decrease of life satisfaction found in adults aged 75 and older (Netuveli et al., 2006), but also to the link between life satisfaction and terminal decline in older adults (Gerstorf et al., 2008). Gerstorf and colleagues (2008) found that the rate of life satisfaction decline tripled in older adults within the last 4 years of life, and that this decline was prolonged for those with a longer lifespan. A number of obstacles to life satisfaction particularly affect older adults who are members of racial and ethnic minority groups, including discrimination, financial and health issues, language barriers, and/or cultural differences (Baernholdt et al., 2012; Kahn & Pearlin, 2006; Utsey, Payne, et al., 2002).
The disadvantaged social status of older adult minority group members often leads to an increase in one of the barriers to life satisfaction, stress, when compared with nonminority group members (Keyes et al., 2011; Moritsugo & Sue, 1983; Williams et al., 1997). This is sometimes referred to as minority stress (Meyer, 2003; Wei et al., 2010). While this increased stress can impact the life satisfaction of minority group members of various ages (Utsey, Payne, et al., 2002), exposure to the cumulative experience of disadvantage (i.e., multiple jeopardy) might make minority older adults more vulnerable in terms of stress and ensuring life satisfaction in their later lives. Multiple jeopardy is considered when minority group members face “double burdens” or “multiple hazards” such as discrimination in both age and race (Bowleg et al., 2003; Ferraro & Farmer, 1996). From this perspective, minority older adults may experience higher levels of stress and lower levels of life satisfaction as compared to older adults from nonminority groups. For example, according to Utsey, Payne and colleagues (2002), African American older adults reported lower levels of education, lower occupational status, and lower income when compared to White older adults. As increases in stressors can negatively impact life satisfaction (Utsey, Chae, et al., 2002), this emphasizes the need for methods of stress reduction.
Several studies have identified effective coping skills as a protective factor that can be used to help reduce levels of stress (Surujlal et al., 2013; Utsey et al., 2000). According to the transactional theory of stress and coping (Lazarus & Folkman, 1984), coping skills refer to a person’s ability to manage problems by utilizing cognitive behavioral efforts when confronted by stressful situations (Stein & Nyamathi, 1998). The possession or lack of coping skills determine how people control stressful situations or if they have an appropriate mastery of their responses to stress (Pearlin & Schooler, 1978). Research in the United States shows mixed findings in the coping styles used among racial/ethnic groups, but not in the amount of coping utilized. A study on Mexican immigrants, Mexican-Americans, and non-Hispanic Whites found similar levels of perceived stress and the total number of coping styles used by the three groups, but found differences in the type of coping used (Farley et al., 2005). In terms of individual coping skills, Mexican citizen groups preferred utilizing denial and religion as coping skills while Mexican-Americans and non-Hispanic Whites did not illustrate differences in coping styles (whether in aggregate or in terms of individual coping styles). A study on racial discrimination, coping, life satisfaction, and self-esteem among African Americans found that when African Americans face stress regarding racism and discrimination, they tend to seek out social support as a coping mechanism (Utsey et al., 2000). Another study examining the coping skills used by Black and White participants indicated a higher use of both problem-focused coping and emotion-focused coping among Black participants when compared to their White counterparts—except in racially stressful situations when both Black and White participants used more confrontive coping (Plummer & Slane, 1996). The age range of participants in the various studies vary greatly, however, and so it is unknown whether the findings in these studies are applicable to older adults of differing racial/ethnic groups. Altogether, more specific information is needed in determining the relationship between perceived stress and the effectiveness of using coping skills in later life.
In sum, life satisfaction, stress, and coping skills may be interrelated. Some research has shown that along with their impact on stress, coping skills might critically influence life satisfaction (Gattino et al., 2015; Surujlal et al., 2013; Tartaglia et al., 2018). In addition, the relationship between stress and life satisfaction may vary when coping skills are considered.
To examine this topic further, the transactional theory of stress and coping (Lazarus & Folkman, 1984) is used as a framework illustrating the relationships between these related variables. This theory evaluates the process of how coping can be used to mitigate stress and emphasizes the importance of emotion and environment in this relationship (Lazarus & Folkman, 1984). Life satisfaction can be considered a long-term outcome in this theory. Coping strategies are divided into emotion-based strategies (focused on dealing with the problem by adjusting the individual’s response to it) and problem-based strategies (focused on dealing with the stressor itself by trying to fix it or mitigate its effects). Carver and colleagues (1989) added an additional component to coping strategies by separating out unhelpful (i.e., maladaptive) coping strategies. The Coping Orientation to Problems Experienced (COPE) scale by Carver and colleagues (1989) illustrates this difference as the various subscales are grouped into these three categories: emotion-based coping, problem-based coping, and maladaptive coping.
Although the transactional theory of stress and coping describes coping as a mediator in the relationship between stress and its short- and long-term outcomes (e.g., life satisfaction; Folkman et al., 1986), relatively little is known about whether coping skills might function as a mediator between stress and life satisfaction specifically among diverse older adult populations. The diversity in coping skills used among varying racial/ethnic groups described in previous research may impact this relationship. Thus, the current study considers the interplay of the relationships between life satisfaction, stress, and coping skills both with different racial and ethnic groups and with the older adult population. The objectives of this study are (a) to examine the differences between minority and nonminority older adults in their levels of life satisfaction, stress, and coping skills; and (b) to examine whether coping skills might function as a mediator between stress and life satisfaction among minority and nonminority older adult groups. Based on previous research, three main hypotheses have been proposed:
Overall, this study is intended to provide better information about the relationships between life satisfaction, stress, and coping skills among older adults. The intent of this study is to help researchers and practitioners be more aware of how differences in minority status may affect these relationships.
Methods
Data
Data were utilized from the Well Elderly 2 study in Los Angles, California, 2004–2008. The purpose of this study was to determine if a preventative lifestyle-based intervention for occupational therapy for older adults was effective and/or cost effective (Clark et al., 2012). The participants were recruited from 21 sites in Los Angeles, including retirement communities, senior housing, and community centers for older adults (Jackson et al., 2009). Participants were excluded if they were not proficient in either English or Spanish, could not attend the intervention, or did not understand or finish the assessment with the assistant. Participants completed a baseline questionnaire before they started and then were given a follow-up questionnaire 6 months after the intervention period. The Well Elderly 2 study consisted of a face-to-face survey that contained measures of health-related quality of life, life satisfaction, and depression. The current study only utilized baseline data. Of the total number of baseline participants (N = 460), 172 were White, 151 were African American, 97 were Hispanic, 18 were Asian, 20 were of other racial/ethnic backgrounds, and two refused to answer. Ages ranged from 60 to 90 years. Participants who identified as White were designated as nonminority for analysis in this study. Participants who identified as African American, Hispanic, Asian, or from other racial/ethnic groups were designated as minority group members in this study. The participants who did not provide racial or ethnic information were designated as missing.
Measures
Life Satisfaction
The Life Satisfaction Index-Z (LSI-Z; Wood et al., 1969) was used to assess life satisfaction. The LSI-Z has been frequently utilized in measures of well-being and quality of life (Stanley et al., 2003). It consists of 13 items presented on a three-point scale (0 = Disagree, 1 = Unsure and 2 = Agree). For example, one of the questions is “As I grow older, things seem better than I thought they would be.” The scale score is calculated by the sum of scores of all 13 items; scores may range from 0 through 26. A higher total score indicates that people have a higher level of life satisfaction. The reliability of the LSI-Z was .79 (Wood et al., 1969). In the current study, Cronbach’s α for this measure was acceptable (α = .77).
Stress
To assess participants’ levels of stress, the Perceived Stress Scale (PSS; Cohen et al., 1983) was utilized. The PSS originally consisted of 14 items; however, the PSS was modified to 18 items by Well Elderly 2 researchers to assess the frequency with which individuals perceive their stress as due to poor health, transportation, social relationships, finances, neighborhood, and related to racial factors. Participants were asked how often they felt or thought about various issues in daily life. For example, one of the questions is “How often have you been upset because of poor health?” Response options utilize a five-point Likert-type scale (1 = Never, 2 = Almost Never, 3 = Sometimes, 4 = Fairly Often, and 5 = Very Often). The total stress score is calculated by the sum of the scores of all 18 items; scores may range from 18 through 90. A higher total score indicates that people have a higher level of perceived stress. The reliability of the PSS ranged from .84 to .86 (Cohen et al., 1983). Cronbach’s α for this measure was good in the present sample (α = .86).
Coping Skills
To assess the mediating variable, individual coping skills, the COPE scale was used (Carver et al., 1989). The COPE scale originally consisted of 60 items; however, 36 items were selected from the original COPE scale by Well Elderly 2 researchers. These items assess a variety of coping skills such as Active Coping (e.g., I did what had to be done, one step at a time), Planning (e.g., I made a plan of action), Suppression of Competing Activities (e.g., I kept myself from getting distracted by other thoughts or activities), Positive Reinterpretation and Growth (e.g., I looked for something good in what was happening), Acceptance (e.g., I accepted that this had happened and that it couldn’t be changed), Religious Coping (e.g., I tried to find comfort in my religion), Behavioral Disengagement (e.g., I admitted to myself that I couldn’t deal with it, and quit trying), Mental Disengagement (e.g., I turned to work or other substitute activities to take my mind off things), Self-Blame (e.g., I’ve been blaming myself for things that happened), and Drugs and Alcohol (e.g., I used alcohol or drugs to make myself feel better). Participations were asked what they generally did and felt when they experienced stressful events on a four-point scale (1 = I usually did not do this at all, 2 = I usually did this a little bit, 3 = I usually did this a medium amount, and 4 = I usually did this a lot). The score is calculated by the averaging the scores of all 36 items; scores may range from 36 to 144. A higher total score indicates that coping skills are used more frequently. Reliabilities from the original COPE Inventory were provided for each of the subscales, which had alphas ranging from .62 to .92 (Carver et al., 1989). Cronbach’s α for this measure was high in the present sample (α = .90).
Socio-Demographic Characteristics
Sociodemographic items include information on sex, race and ethnicity, level of education, employment, and income. For example, level of education was measured by the question: “How far did you go in school?” This was measured by asking participants to check their answers on an eight-point Likert scale ranging from 0 to 4 years of school completed to postgraduate study.
Data Analysis
Simple and multiple regression techniques were used to examine the relationships between the variables. First, descriptive statistics utilized for sociodemographic variables, stress, coping skills, and life satisfaction to offer a basic understanding of the sample characteristics. Second, t-tests were run between minority and nonminority participants with each of the three main variables (i.e., stress, life satisfaction, and coping skills) to determine if significant differences exist between groups. Third, Spearman correlations were used to assess the relationships between independent and outcome variables. If each of the bivariate relationships (i.e., simple regression) are significant, mediation is probable. Lastly, to test the mediating effect of coping skills, analyses were performed with using Hayes’s (2017) PROCESS macro. To obtain robust standard errors in parameter estimation, the bootstrapping method was applied while examining the significance of the effects. Using this method, 95% confidence intervals of the effects were obtained from 10,000 resamples of the data. Confidence intervals should be interpreted as significant at α = 0.05, when zero is not included in the interval.
Results
Descriptive Characteristics of the Sample
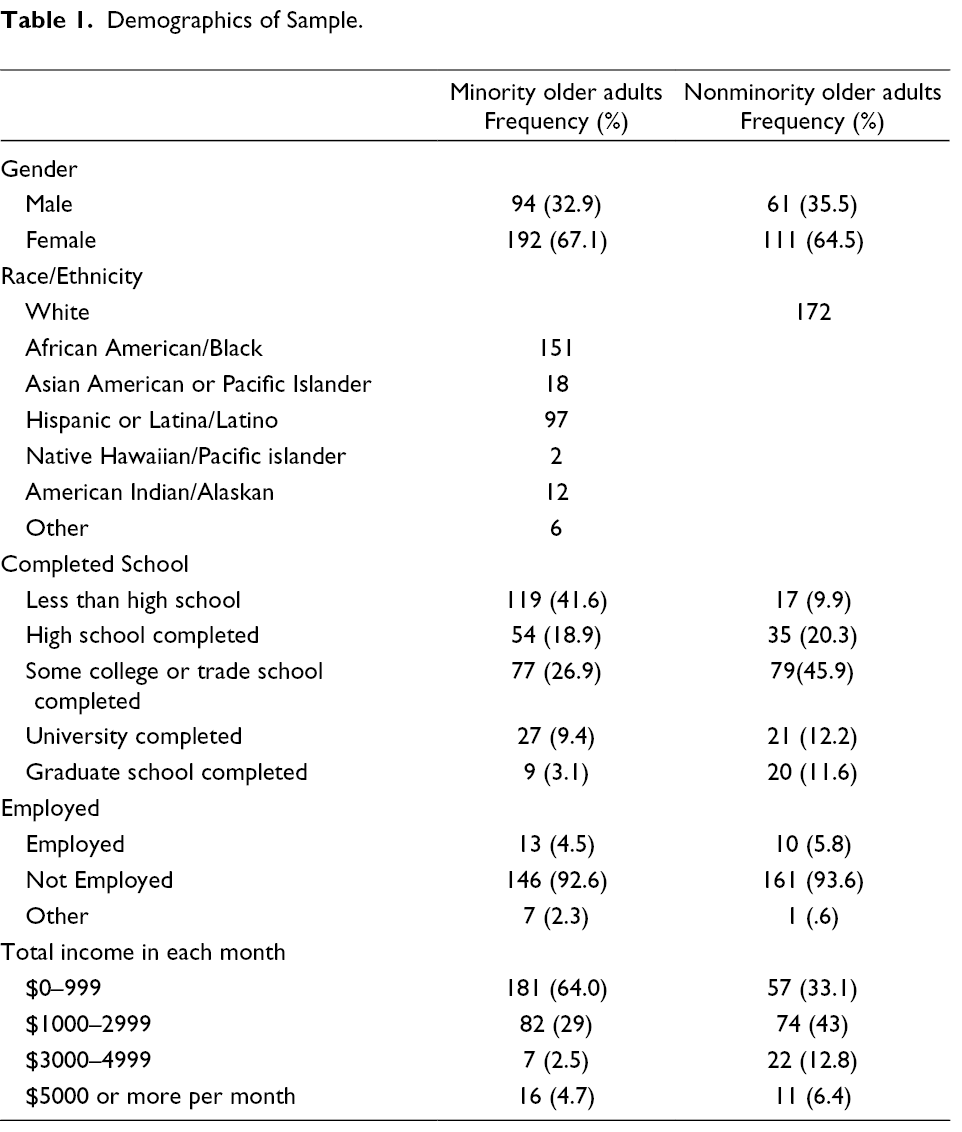
For the purpose of the current study, only 286 minority older adults and 172 nonminority older adults, who completed the baseline survey, were included in the analyses. The characteristics of both the older adult groups are displayed in Table 1. Among the minority older adult group, the majority of participants were female (n = 192, 67%), retired (n = 146, 92.6%), and made less than $1000 per month (64%), while many had less than a high school education (n = 119, 41.6%). Twenty-nine percent of participants made $1000–2999 per month. On the other hand, among White older adults, the majority of participants were female (n = 111, 64.5%) and retired (93.6%), while many completed some college (n = 79, 45.9%), and made between $1000 and $2999 per month (n = 74, 43%).
Demographics of Sample.
Types of Stress and Overall Life Satisfaction
A comparison of types of stress and overall life satisfaction for the older adult groups are shown in Table 2. We found that minority participants reported higher levels of stress than nonminority participants. This difference was significant (t = −3.927, df = 351.344, p = .000). The two top stressors (finances and poor health) were the same for both groups. However, the third top stressors were different in both groups. Minority participants reported transportation; however, nonminority participants reported social relationship as the third top stressor.
Types of Stress and Life Satisfaction.
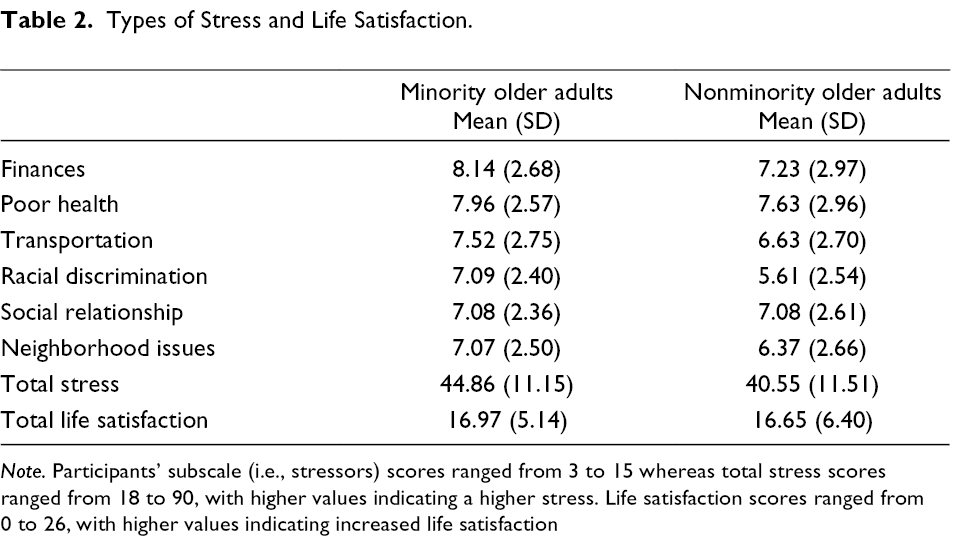
Note. Participants’ subscale (i.e., stressors) scores ranged from 3 to 15 whereas total stress scores ranged from 18 to 90, with higher values indicating a higher stress. Life satisfaction scores ranged from 0 to 26, with higher values indicating increased life satisfaction
The lowest three stressors for minority older adults were racial discrimination, social relationship, and neighborhood issues. These results differed for nonminority older adults, whose lowest three stressors were transportation, neighborhood issues, and racial discrimination.
With regard to life satisfaction, the differences between minority older adults and nonminority older adults was not significant (t = −.594, df = 302.836, p = .57).
Types of Coping Skills
A comparison of types of coping skills for the older adult groups is shown in Table 3.
Types of Coping Skills.
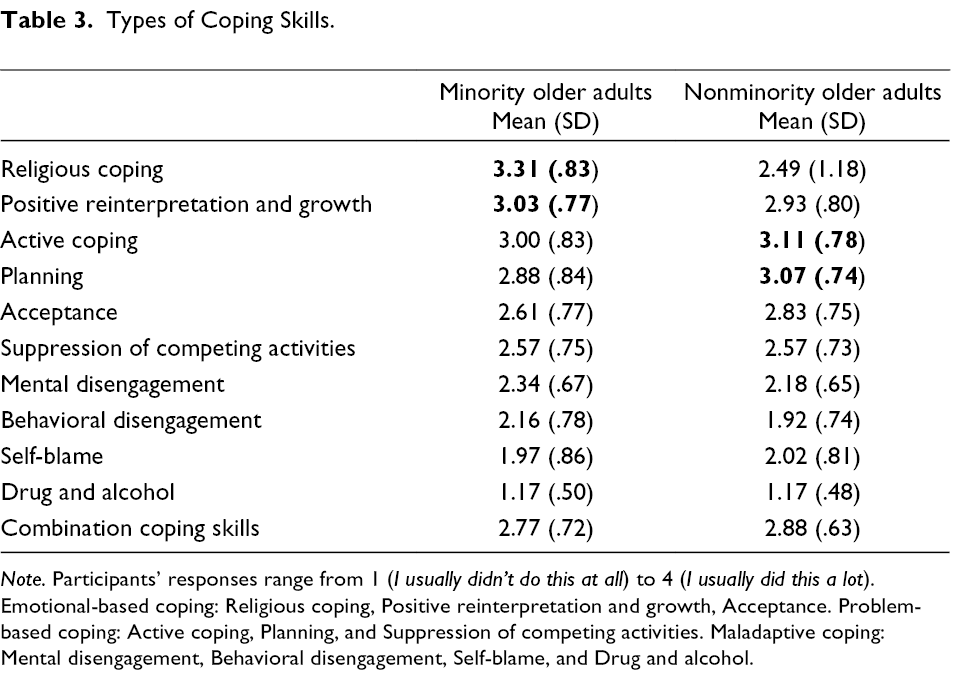
Note. Participants’ responses range from 1 (I usually didn’t do this at all) to 4 (I usually did this a lot). Emotional-based coping: Religious coping, Positive reinterpretation and growth, Acceptance. Problem-based coping: Active coping, Planning, and Suppression of competing activities. Maladaptive coping: Mental disengagement, Behavioral disengagement, Self-blame, and Drug and alcohol.
Nonminority participants reported higher levels of coping skills than minority participants, but this difference was not significant (t = 1.629, df = 398.301, p = .104). Specifically, the three top coping skills for minority participants were religious coping, positive reinterpretation and growth, and active coping. On the other hand, the top three coping skills for nonminority participants included active coping, planning, and positive reinterpretation and growth.
Bivariate Correlations
A Pearson correlation coefficient was computed to assess the relationship between the various coping skills, total stress, and total life satisfaction (Table 4). Overall, total stress was negatively associated with life satisfaction among minority older adults (r = −.40, p < .01) and nonminority older adults (r = −.51, p < .01). A comparison of total coping skills and subsets of coping skills (e.g., active coping, planning, positive reinterpretation and growth, and self-blame) with life satisfaction was conducted among both groups. Specifically, participants with higher levels of total coping skills, active coping, planning, and positive reinterpretation and growth were more likely to be satisfied with life among both groups. Participants with lower levels of self-blame as a coping skill were also more likely to be satisfied with life among both minority older adults and nonminority older adults. In addition, minority older adults with a lower level of drug and alcohol use as a coping skill were more likely to be satisfied with life (r = −.14, p < .05); however, this result was not supported among nonminority older adults (r = .02, p > .05). Nonminority older adults with a higher level of acceptance (r = .29, p < .01), a higher level of religious coping (r = .18, p < .05), and a lower level of behavioral disengagement (r = −.20, p < .01) were more likely to be satisfied with life.
Correlations Among Study Variables.
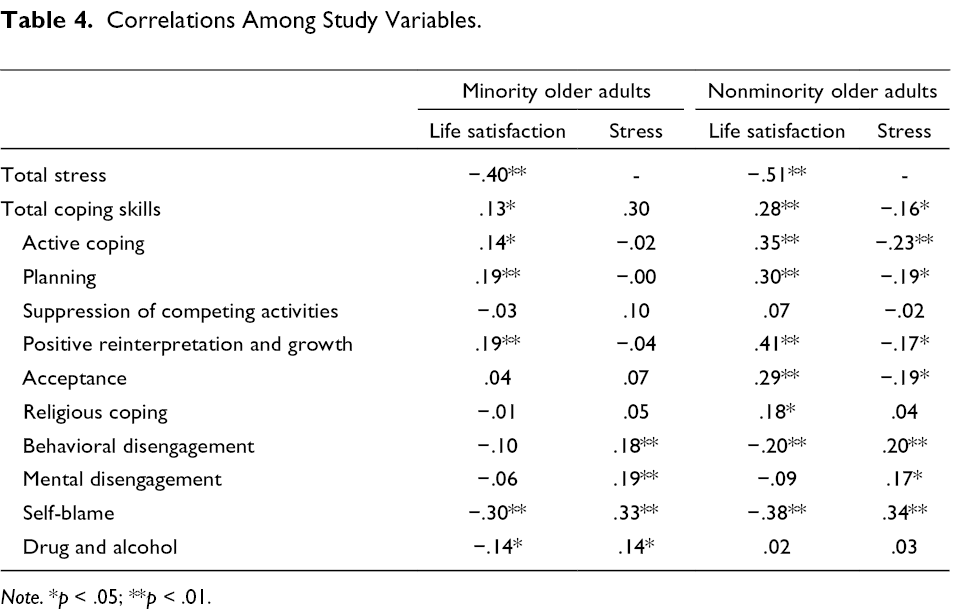
Note. *p < .05; **p < .01.
Participants of both groups were compared with regard to their stress levels and their methods of coping. Higher levels of stress were significantly associated with lower levels of total coping skills among nonminority older adults (r = −.16, p < .05), whereas minority groups did not report a significant association between these variables (r = .03, p > .05). Both groups displayed higher levels of stress when higher levels of behavioral disengagement, mental disengagement, and self-blame were present. Higher levels of drug and alcohol use were also significantly associated with higher stress levels among minority older adults (r = .14, p < .05). Higher stress levels were also associated with less use of certain coping skills among nonminority participants: active coping (r = −.23, p < .01), planning (r = −.19, p < .05), positive reinterpretation and growth (r = −.17, p < .05), and acceptance (r = −.19, p < .05). These relationships were not significant among minority older adults though.
Testing for Mediation Effect
As a main hypothesis, this study assumed that coping skills might function as a mediator between stress and life satisfaction among minority and nonminority older adult groups (Table 5). Results from a simple mediation analysis indicated that the mediation was not supported for either minority or nonminority older adults. To be specific, while controlling for demographic variables, stress was negatively associated with life satisfaction. The indirect effect of stress on life satisfaction through coping skills was not significant. This model shows that stress was not significantly associated with coping skills, although coping skills was positively associated with life satisfaction. According to the mediation analysis, there is evidence that stress is negatively associated with life satisfaction above and beyond the indirect effect.
Evaluating the Mediation of Coping Skills in the Association Between Stress and Life Satisfaction.
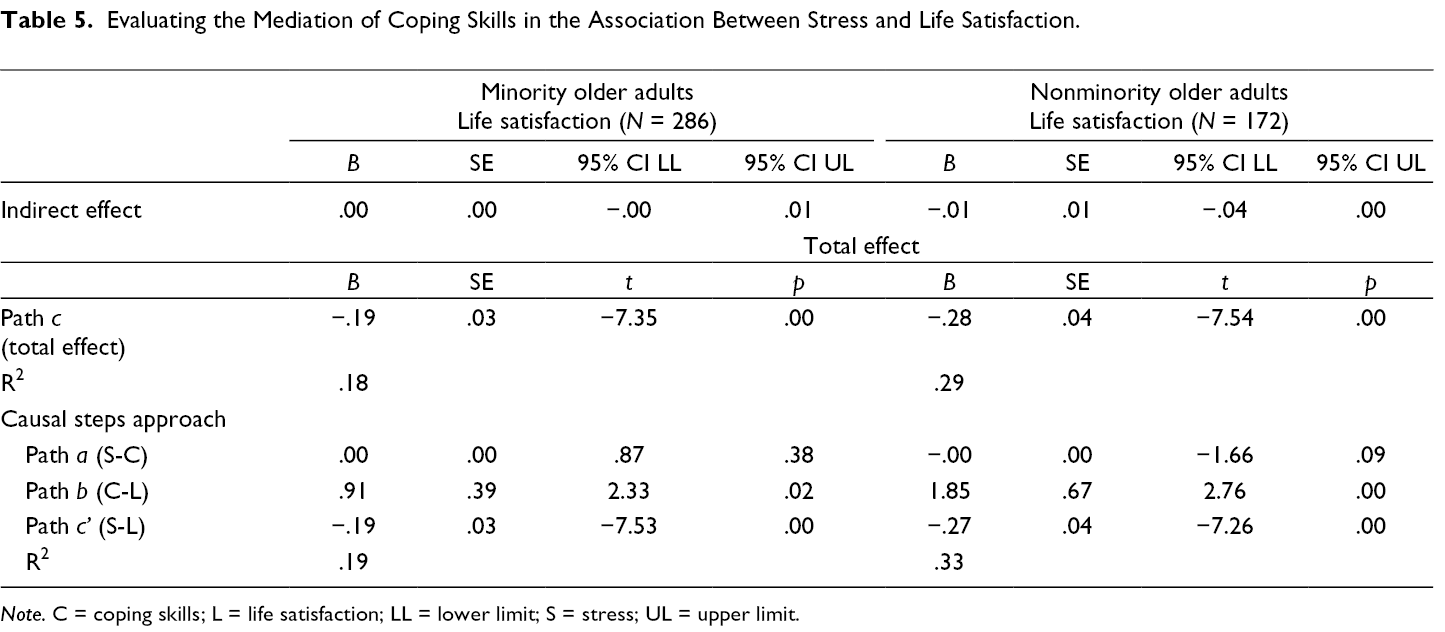
Note. C = coping skills; L = life satisfaction; LL = lower limit; S = stress; UL = upper limit.
Discussion
This study examined various types of life satisfaction, stress, and coping skills, as well as whether coping skills might function as a mediator between stress and life satisfaction among minority and nonminority older adult groups. First, consistent with the first hypothesis and with previous research (U.S. Department of Health and Human Services, 2001; Velez et al., 2017), this study found that minority older adults faced significantly higher levels of stress than nonminority older adults. Specifically, minority older adults reported three top stress factors: finances, poor health, and transportation. Nonminority older adults also indicated similar stressors with the top three being poor health, finances, and social relationship. The lowest stressor among nonminority older adults was racial discrimination; however, it is interesting that racial discrimination was not among the top three stressors facing minority older adults. This finding is surprising as previous research on discrimination indicates that racially and ethnically diverse minority older adults reported high levels of experience with discrimination. As discrimination negatively impacts life satisfaction (Ayalon & Gum, 2011; Barnes et al., 2008; Benjamins & Whitman, 2014), it was thought that discrimination would be ranked higher among the stressors. The top stressors found in the current study (e.g., financial and physical issues) appear to be basic needs. It is possible that the participants’ primary stressors focused on more essential issues in daily lives among minority older adults than other types of stressors, such as the experience of discrimination. It may be important for practitioners to assist minority older adults with stressors related to the basic needs of daily life before concentrating on other stressors that the clients may experience. As such, practitioners might evaluate the stressors their clients experience and prioritize addressing the stressors related to the clients’ basic needs in their action plan. For example, practitioners with clients dealing with financial stressors can assist their clients in looking at their spending patterns and triggers or link them with resources which target their problem (e.g., managing debt, finding work, getting more education, etc.). Practitioners might also help clients apply for various programs (e.g., Medicaid, Supplemental Security Income, etc.) to better meet their basic needs and thus reduce the level of stress in their daily lives. While more targeted research in the area of stressors related to basic needs is recommended, practitioners seeking to improve the life satisfaction of their older adult clients may wish to place a particular emphasis on stressors related to basic needs.
Inconsistent with the second part of the first hypothesis, minority older adults did not report a lower degree of life satisfaction than their nonminority group counterparts. This is incongruent with previous research (Baernholdt, Yan, et al., 2012). One possible reason for this inconsistency is that the current study grouped all racial and ethnic minority groups together for the analyses. Some research shows, however, that minority groups can differ in their levels of life satisfaction; for example, Blacks having lower levels of life satisfaction than Whites, but Hispanics reporting higher levels of life satisfaction than Whites (Knies et al., 2016). Research has shown that variances in cultural norms can result in changes in life satisfaction (Kuppens et al., 2008). This suggests that grouping all of the minority groups together in the same analysis may mask some differences in life satisfaction levels. Researchers should note that although minority groups may all experience multiple jeopardy, it is important to keep in mind the uniqueness that each culture imparts on differing minority group members. A second possible reason is that research has shown that life satisfaction can be significantly impacted by geographic area (Holzer et al., 2005). As the current study took place in one city in the United States (Los Angeles, California), it is possible that these life satisfaction scores would differ if participants lived in another location.
Next, consistent with the second hypothesis, this study found that the top coping skill used by minority older adults varied from that of nonminority older adults. Religious coping (e.g., praying) was the most frequently used coping skill among minority older adults, whereas active coping (e.g., taking action to improve the situation) was the most frequently used coping skill among nonminority older adults. The use of religious coping as one of the top coping skills used by minority older adults is consistent with previous studies (Chatters et al., 2008; Dunn & Horgas, 2004; Ward et al., 2013). In general, religious coping is useful for reducing stress and improving life satisfaction. For example, previous studies on religious coping have indicated that racially and ethnically diverse minority groups, women, and immigrants use religious coping skills more frequently as compared to others who do not share the same backgrounds (Chatters et al., 2008; Dunn & Horgas, 2004). However, in the bivariate analyses, we found that even though minority older adults used religious coping most frequently in daily life, religious coping was not significantly associated with life satisfaction among minority older adults. This was not the case among nonminority older adults. This finding implies that in spite of the importance of religion in minority older adult lives, this coping mechanism may not be efficacious in improving life satisfaction in minority older adults, though it is successful in doing so with their nonminority counterparts.
Both minority and nonminority groups reported similar coping skills among their other most frequently used coping skills with the top three being active coping, planning, and positive reinterpretation and growth (with the exception of religious coping for minority members). Although used in a different order among both groups, positive reinterpretation and growth, active coping, and planning were significantly associated with life satisfaction among both minority and nonminority older adults. All three of these skills can be fostered through the use of cognitive therapy. Research indicates that cognitive intervention or activities enable older adults to improve mental and physical health (Hofmann et al., 2012; Reijnders et al., 2013). Therefore, practitioners should consider the cognitive intervention as a feasible approach for improving life satisfaction of older adults regardless of their race or ethnicity. For example, positive reinterpretation and growth illustrates a common technique in cognitive behavioral therapy (Craig & Austin, 2016). Using this technique, an individual would try to reframe a negative situation to see it in a more positive light. A practitioner might encourage a client who was recently fired from their job to reframe this problem into an opportunity to re-examine their professional career to determine if they are doing what they really want to do or if something else would fit them better. If they decide they like their current path, they can see this as an opportunity to identify what wasn’t working in their last job and brainstorm ways to fix that in the future.
While some problem-based and emotion-based coping skills (i.e., nonmaladaptive) have been shown to have significant relationships among minority older adults with regard to life satisfaction, the only coping skills that were significantly related to stress among minority participants on the bivariate level were maladaptive coping skills (e.g., drug and alcohol use, self-blame, behavioral disengagement, and mental disengagement). This was not the case for nonminority participants. For the nonminority older adults, all three types of coping skills significantly affected their stress levels. This indicates that while practitioners working with minority older adults experiencing stress might choose to discourage their clients from utilizing maladaptive coping skills, their efforts to encourage nonmaladaptive coping skills may not be as impactful with regard to stress reduction. It may be that other coping skills exist that were not captured in the widely used COPE scale (Carver et al., 1989), which might benefit minority older adults. To investigate this avenue of research would likely necessitate a thorough scan of the literature, or a more qualitative approach—interviewing minority older adults to determine if any methods of coping are being utilized which are not currently accounted for on the current scale.
Lastly, contrary to the third hypothesis, coping skills did not function as a mediator between stress and life satisfaction among either group. This finding also appears to contradict the transactional theory of stress and coping (Lazarus & Folkman, 1984), where coping is seen as a mediator between stress and its outcomes (e.g., life satisfaction; Folkman et al., 1986). This finding indicates that in the mediation model, although both stress and coping skills were significantly associated with life satisfaction, stress was not significantly associated with coping skills for either group when the demographic characteristics were held constant. This unexpected finding may be explained in several ways. First, we expected that stress was positively associated with coping skills; however, the position of the variables might be wrong. Some studies have indicated that while coping has long been considered to be a response to stressful situations, coping can also be considered an action that preempts stressful situations when individuals anticipate the stress to come. This preemptive use of coping has been found to have various positive outcomes on stress (Abbas et al., 2013; Greenglass & Fiksenbaum, 2009). In other words, coping skills can be used as a protective resource to reduce the level of stress at the outset rather than reducing the level of stress experienced retroactively (McMillan et al., 2006). As such, the current analysis may not be capturing the full relationship between the variables. Second, much of the previous research has targeted a younger population of racially and ethnically diverse minority groups (Keyes et al., 2011; Utsey et al., 2000). The findings from the current study imply that the relationship identified in previous research might disappear over time. Future research should re-examine relationships between stress and coping skills to find a better understanding of their order. Conducting more studies on this topic area with various ages in this population may help to determine if the relationship between life satisfaction, stress, and coping skills changes as minority participants age.
Limitations
There are a few limitations that should be noted. First, this original study focused on a specific area (i.e., California) for data collection so the findings of the current study cannot be generalized to the overall minority older adult population in the United States. Second, this study did not delve into the influence of culture despite its focus on racial and ethnic differences between participants. In the current article, the participant race variable was collapsed to specify only minority older adults and nonminority older adults. Many of the minority groups included in this study were not able to be examined individually due to limitations in sample size. A more targeted future study with a larger number of group members from other minority groups would be recommended. Although the current analysis allowed us to examine broad differences between minority and nonminority groups, it did not enable us to delve into the differences between the various minority groups in the areas of life satisfaction, stress, and coping skills. Different cultures have different values and beliefs which may impact how individuals cope with stress and experience life satisfaction. Thus, it might be helpful for future researchers to examine each racial/ethnic minority grouping individually. Lastly, for purpose of the current study, cross-sectional data were used (e.g., baseline data only), which limits interpretations of causality.
Conclusion
This study explored life satisfaction, stress, and coping skills among both minority and nonminority older adult groups. The findings of this study provide insights regarding how practitioners offer services to older adults in all racial and ethnic groups in the areas of variances in life satisfaction, the treatment of stressors, and the use of coping skills. Based on these findings, practitioners should be able to focus their clients on the coping skills that are more likely to improve life satisfaction in both minority and nonminority older adults, as well as target the stressors most needed to be addressed in their minority clients.
Footnotes
Acknowledgements
We appreciate that Dr. Florence Clark and colleagues publicly shared the Well-Elderly 2 data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the esearch, authorship, and/or publication of this article.
Author Biographies