
Abstract
Disability is a common reason for the loss of independence. There is a dearth of data on older adults with disability in south-eastern Nigeria. Using a multistage sampling technique and disability indexes, we assessed 816 persons aged 65 years and above living with a disability. While respondents’ experiences of abuse and property inheritance differ by gender, they have poor health status. Elevated risks of disability were associated with gender, increased age, education, smoking, alcohol use, and engagement in physical exercise. Findings suggest urgency in formulating and implementing ageing welfare policy in this African community undergoing demographic and social changes. While this is underway, we recommend a massive health promotion among older adults in this community. We also suggest the integration of courses on ageing in schools’ curriculum since ageing is a life course phenomenon. This in the long run would provide ageing-friendly education that averts old age's deleterious effects.
Background
Old age, most often, is associated with functional impairments and disability, making it a vulnerable stage of life. Operationally defined, disability relates to any impediment to older person's ability to effectively carry out their Activities of Daily Living (ADL) or Instrumental Activities of Daily Living (IADL). Across the globe, the proportion of older adults with a disability varies. Specifically in Nigeria, over three million (NPC, 2006) have at least one form of disability. On the other hand, Lang & Upah (2008) revealed that as many as over 19 million live with a disability in Nigeria. Irrespective of the figures reported, disability, especially among older adults, is under-researched and has been within the biomedical purview. Although this clinical perspective is crucial, however, the absence of a social dimension creates a critical gap in the literature. Moreover, with no policy focus on older adults generally, it becomes germane to understand disability among older adults relative to their health and social conditions, to inform ageing policies in Nigeria, especially in the southeast where the study was conducted.
Gender relations, living arrangements, health accessibility and affordability, economic factors, lifestyles in earlier years, life chances, and choices present specific consequences for older adults’ wellbeing. In a patriarchal society, older women with disability face double jeopardy of being disabled and multidimensionally poor as a result of poverty, social exclusion, and lack of land/property ownership that find expression in patriarchy. Their long-term exposure to inequity along the life course, resulting from discrimination and disadvantages in labor force participation, is reflective of lifetime poverty (NPC, 2003). With implications for independent living and the need for adjustment or change, living arrangements in later life change especially when there is a disability (Ramashala, 2001). Although in Africa, social change to some extent is eroding living arrangements (Apt, 1992), and many households constitute skipped generation (UNFPA and HelpAge, 2012) consequent upon migration (rural-urban) of middle generation (adults), living arrangements are still rooted in the extended family system with its close knit-network. Many older adults continue to live with their children, spouses, or relatives. In other societies, living arrangements vary as many older adults live in institutional homes.
Attaining physical and mental health of the highest standard require that older persons have access to affordable long-term health care that is both curative and preventive, with the necessary health information (UNFPA and HelpAge International, 2012). However, as health care becomes “an essential commodity” and out-of-pocket payment persists, older adults with a disability are unable to have access to affordable health care, thus increasing their vulnerability.
In this paper, we reported socio-demographic characteristics of older adults with disability in south-eastern Nigeria. We also presented correlates of their disability. The respondents’ living arrangements, experience of abuse, reportage of abuse, health status, as well as channels, and quality of health care received were analyzed. Lastly, we discussed these variables and proffered some policy recommendations.
Methods
This study is community-based, cross-sectional, and exploration of health and social conditions of older adults with disability in south-eastern Nigeria. Older adults (defined as population aged 65 and above) constitute 4.5% of the total population and comprises mostly the Igbo-speaking language extraction in Nigeria. The choice of the study area is purposive and consequent upon the need for empirically informed policy recommendations for the improvement of older adults’ welfare in the region. A multistage sampling technique comprising cluster, systematic and simple random sampling procedures were used to enlist 1030 respondents. The Katz index Activities of Daily Living (ADL) and Lawton Instrumental Activities of Daily Living (IADL) were used to predetermine disability by asking the selected 1030 respondents if they needed help to perform ADL or IADL. When they responded “Yes” in any of those activities, they were considered to have a disability. While respondents who did not have any disability were discontinued, a total of 816 respondents with any disability were further assessed in the study.
The ADL includes dressing, bathing, toileting, transferring, continence and feeding. The IADL includes laundry, food preparation, ability to handle finances, housekeeping, responsibility for one's medication, transportation, shopping, ability to use the telephone, physical activities such as attending meetings and engageing in physical exercises.
Life history and in-depth interviews were administered to 24 purposively selected participants. The study was both self- and proxy reports by primary caregivers.
Findings
As shown in Table 1, more than two-thirds (73.5%) reside in rural areas. Males account for 63% of the total sample. Respondents’ mean age is 72.9 years. Nearly 3 in 5 (45.0%) have no formal education. Almost 8 out of 10 (79.2%) respondents have any type of disability. Respondents’ socioeconomic status categorized as low, medium, and high is generated from the number of household items they owned. Those with household items less or equal to two are categorized in the low socioeconomic status; those with three to five items are in the medium group; those with six to ten or more household items are categorized as high. About 4 in 10 respondents (41.1%) are classified in the medium (average) socioeconomic status. More than half (55.2%) have medium income (scaled between N20,001.00 and N80,000.00) in their previous work. Only 13.5% have high previous income, and a lower proportion have high current income (scaled between N80,000.00 and above). Both previous and current occupations are primarily elementary (subsistence farmers) for most of the respondents.
Socio-Demographic Characteristics of Respondents.

Living Arrangement
Although respondents did not live in institutional homes, their opinions were sought on preference for an institutional home. Only seven affirmed their need to change their environment with the perception of better care if in an institutional home. The others (90.2%) preferred the confines of their personal homes and family members even when given the opportunity to live in an institutional home. Reasons adduced vary. While many wanted to protect their family members against witchcraft and evil persons, others wanted to prevent their homes from being encroached on by neighbors. Other reasons were: To help raise their grandchildren and to have their family members around them always.
Respondents’ preference for their personal homes is a strong indication of the kinship system in Africa where ties with extended families are still maintained despite the wave of urbanization and modernization. Therefore, taking older adults away from their homes to shelter them in an institutional home may lead to alienation. In their case, it may be difficult to adjust and learn new norms and roles of the institution. Thus, any intervention for older adults in this region and generally in Nigeria should be community based.
Experience of Abuse
Experiences of physical and emotional abuse were reported by the respondents. While more males (64.7%) experienced emotional abuse, more females (53.8%) experienced physical abuse. Females’ experience of physical abuse depicts vulnerability; pointing to power structure (dominance) and powerlessness of women in a patriarchal society coupled with their life history of subservience. Perpetrators of abuse were mostly people in a position of trust and related to the respondents mostly children, spouses, and relatives (69.6%). Only 3.7% of perpetrators of violence were caregivers. The lesser percentage of caregivers is adduced to the informal caregiving received by most elderly in many developing countries including south-eastern Nigeria where institutional homes are few as these elderly prefer to be around their family members in old age. People not related to the elderly, regarded as strangers, constituted only 26.8% of perpetrators.
Substantiated in literature, abuse usually takes place within the confines of a trusting relationship and by someone close to the victim such as relatives. On the other hand, hiring caregivers to care for older adults in their homes raises the question of how safe these older adults are before paid caregivers. A female respondent aged 67 and crippled recalled her experience of abuse from a hired caregiver as follows: My children hired a girl to care for me. I loved her that I gave her some of my wrappers (clothes). But this girl maltreated me and I felt heartbroken. She would starve me and not wash my clothes. Because of the love I have for her, I asked her what I have done against her but she did not say anything. One particular Sunday, a daughter of mine visited and cooked food. She asked her to give me the food at a specified time but she failed to do so. I did not know about the instruction my daughter gave her. I felt so hungry. When my daughter visited the next day, I realized that she cooked food for me. I was forced to open up to my daughter about everything she has done against me. They had to sack her but I told them to let her go with the wrappers I gave her for free. Now, my grandson is looking after me in the interim while plans are made for an alternative (IDI/Female/67/Crippled/Rural).
Some older adults may likely opt for institutional homes where they are available because it is their last option especially when they have experienced a series of abuse from people who ought to comfort them or when they do not have children. A respondent narrated his ordeal in the hands of some villagers (relatives) as follows: I am 83 years old. I have had partial deafness for over 15 years and I am currently suffering from cough and ulcer. I resided and worked in Northern Nigeria for a long time but had to relocate to Enugu some years back because of my health. I stopped schooling in standard six because the tendency to go to College or University was very low and was the luxury of the rich then. My wife and I have no children and there is no one to care for us. We have been childless all our lives but I love my wife. In 2011, I developed an eye problem and went for surgery twice. We have been moving from place to place in search of a solution. Although I worked as a government official, I have not received my pension and gratuity. Despite all these, my wife and I were able to build a house but the house is empty because we have no children. At some point when we were moving around for medical attention, the villagers destroyed our building. We relocated to this place because the community was against us. It was a terrible and painful period for us then but we thank God for the Catholic Church that came to our assistance and handed us over to Reverend Sisters to take care of us. I just wish the government will look into old people's experience of abuse and discrimination, and also assist older adults that are experiencing or may have experienced abuse. It will also be good if the government will fund and assist with old people's homes where people like us can go when life threatens us (Life History/83/Male/Urban).
In another narrative, a female respondent aged 70 recounted how she suffered and was abused by her spouse (husband). Experiencing physical abuse by females in the hands of their husbands gives a clear indication of gender-based violence inherent in most patriarchal societies. For some too, old age might be a state of misery especially when there are no children or supportive spouse or adequate financial support as could be deduced in the account below: I am 70 years old but life has been miserable. I am suffering. I have no children now. I had two but they have all died. I am a well-educated woman. I have Bachelor's Degree in Education (B.Ed.), a Teachers’ Training Certificate (TTC Diploma) and National Certificate in Education (NCE). I retired in 1978. My pension has not been regular and, now, they have stopped it. I went to find out why but there was no plausible reason. I once trained someone who became a Professor and I sponsored him overseas but he died. I was not informed about his death until they brought his corpse back to Nigeria. It was such a painful moment because I had hoped he would care for me after the death of my children. Since then, I developed high blood pressure and arthritis coupled with blindness. Notwithstanding my plights, my husband drove me away and got another woman. He maltreated me so badly. I suffered so much. I wish I can die. My husband has been threatening me. At a point, he locked me up in a room and denied me food. Then, a neighbour was indeed helpful and my case was later reported to the Catholic Church. Since then, they have accommodated and supported me. Disability is a hopeless situation especially when you have no child. My husband abandoned me. I am desperate and there is nobody to help me except God. I pray God comes faster. It is painful. I am very sick. I wish the government can pay my pension so I can buy essential things I need (Life History/Female/70/Urban/Blind).
Report of Abuse by Respondents and Channels of Reports
Of all the respondents that experienced any form of abuse, more than half (63.4%) did not report their abuse. Disaggregated by their reasons, 47.3% felt it was a family issue and that family members or children cannot be reported; 32.7% did not report out of fear of what might happen to them afterward like being abandoned or risk of facing more troubles after reporting. The rest (20%) stated that they were ignorant of where, how, or who to report to.
On the other hand, of the 36.6% that reported their experience of abuse, the majority (79%) utilized informal channels like village head, children, community leaders, kinsmen, and relatives. Only 21% reported formally to the police and the court.
Property Inheritance
The study also sought to know if women inherited properties. The findings revealed that only one in five females (20.6%) inherited any property. All male respondents (79.4%) who inherited property stated it was their hereditary or children's right.
However, the reasons differed between males and females who did not inherit any property. While males (35.7%) who did not inherit any revealed that there was nothing to inherit either because their parents had nothing or sold off everything they had. On the other hand, female respondents (64.3%) who did not inherit any property bemoaned cultural practices against women that prevented them from their entitlement or inheritance including forceful denial and acquisition by their husband's family at the death of their husband. A female respondent, widowed, recounted her experiences in the hands of her in-laws as follows: After the death of my husband, my husband's brothers did not only take the proceeds realized from the funeral but they gradually laid claims to his properties saying it belonged to their family and not my husband alone. The worst was that they shared them and gave me nothing and I know it is because I have no male child. This is unfair but I have resigned to fate. What I can boast of is just this roof under my head. (IDI/Rural/Female/69 years/Crippled).
This situation is reflective of some conditions women are faced with, coupled with double jeopardy of being disabled and poor owing to lack of property or land ownership.
Health Status of Respondents and Channels of Health Care by Respondents
Respondents had various kinds of health-related challenges. They self-reported their overall health using three indexes—poor, fair and good. Only one in ten (11.3%) rated their health as good and nearly half (47.7%) indicated that their overall health was poor. Respondents’ poor health status was corroborated by the number that was ill in the past 4 weeks that preceded the study. Accordingly, more than half (56%) had at least one illness including malaria, typhoid, high blood pressure, ulcer, prostate cancer, and waist pain. About 37% accessed healthcare from patent-medicine shops/chemists, followed by Government Health Facility (34%), and Private Health facility (20%). Healthcare payment across these facilities was out-of-pocket.
Quality of Health Care Received
Respondents were asked to rate the quality of care they received. This relates to the extent to which health services increased health outcomes for patients based on the World Health Organisation six domains of quality of care relating to:
Effective Efficient Accessible Acceptable Equitable Safe
The overall score for each category (not, less and very) was computed and re-categorized as (poor, fair, and good) respectively. This helped to give a composite attribute for quality of care received as either poor or just fair or good as shown in Table 2. The majority reported that the quality of health care they received was just fair (46.8%). Reasons might be attributed to the out-of-pocket payment typical in developing countries where ageing welfare policies and health insurance for the elderly are lacking.
Percentage Distribution of Quality of Health CareServices Received.
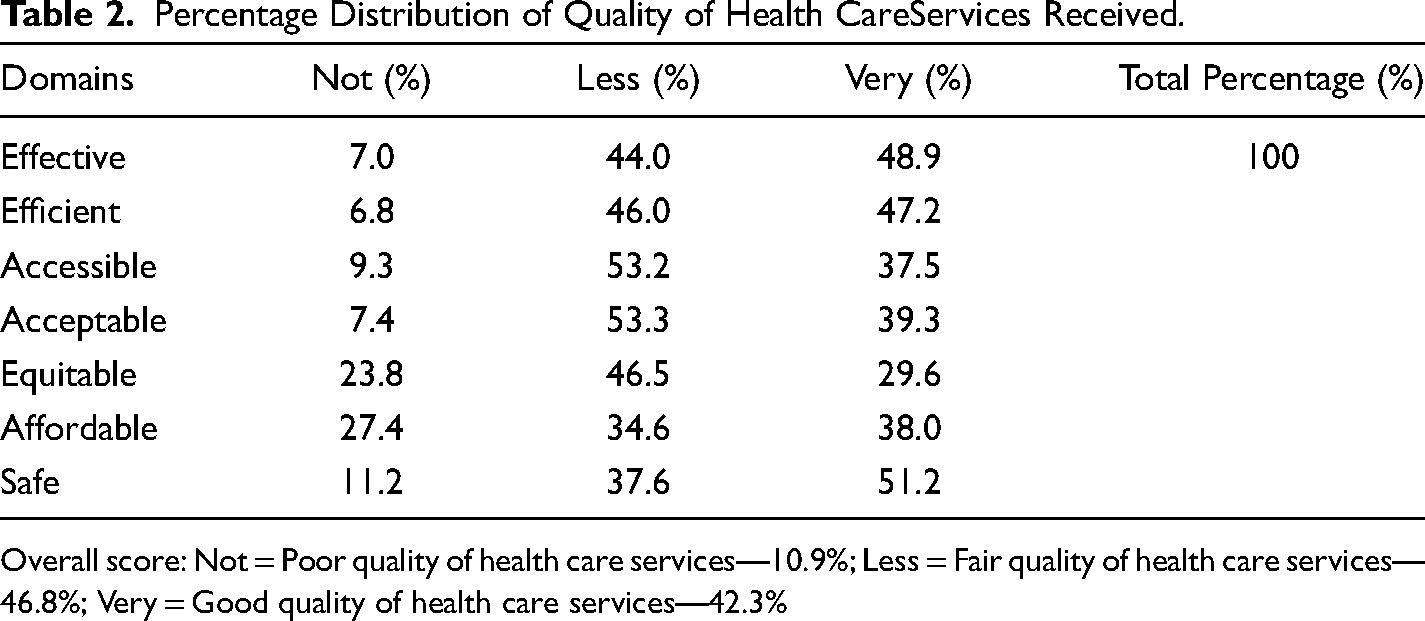
Overall score: Not = Poor quality of health care services—10.9%; Less = Fair quality of health care services—46.8%; Very = Good quality of health care services—42.3%
Respondents Types of Disability
Various types of disabilities had by respondents are shown in Table 3. This was categorized as sight, hearing, mobility, pain, and mental related disability.
Percentage Distribution by Types of Disability Among the Older Adults.

Correlates of Disability Among Older Adults
Significant relationships were found between socio-demographic variables (Table 4), economic variables (Table 5), variables on lifestyles (Table 6) of respondents, and their disabilities. Gender is significantly related to mobility, pain, and mental related disability. Age is significantly related to mobility disability. Respondents’ economic status significantly related to all forms of disability except that associated with pain (osteoarthritis/rheumatism, lower back pain). While smoking had a significant relationship with a mobility-related disability, current engagement in exercise and use of alcohol significantly related to mental disability.
Correlates of Disability and Socio-Demographic Variables.

*Significant @<0.05
Correlates of Disability and Economic Variables.

*Significant at <0.05.
Correlates of Disability and Lifestyle Variables.

*Significant at <.05
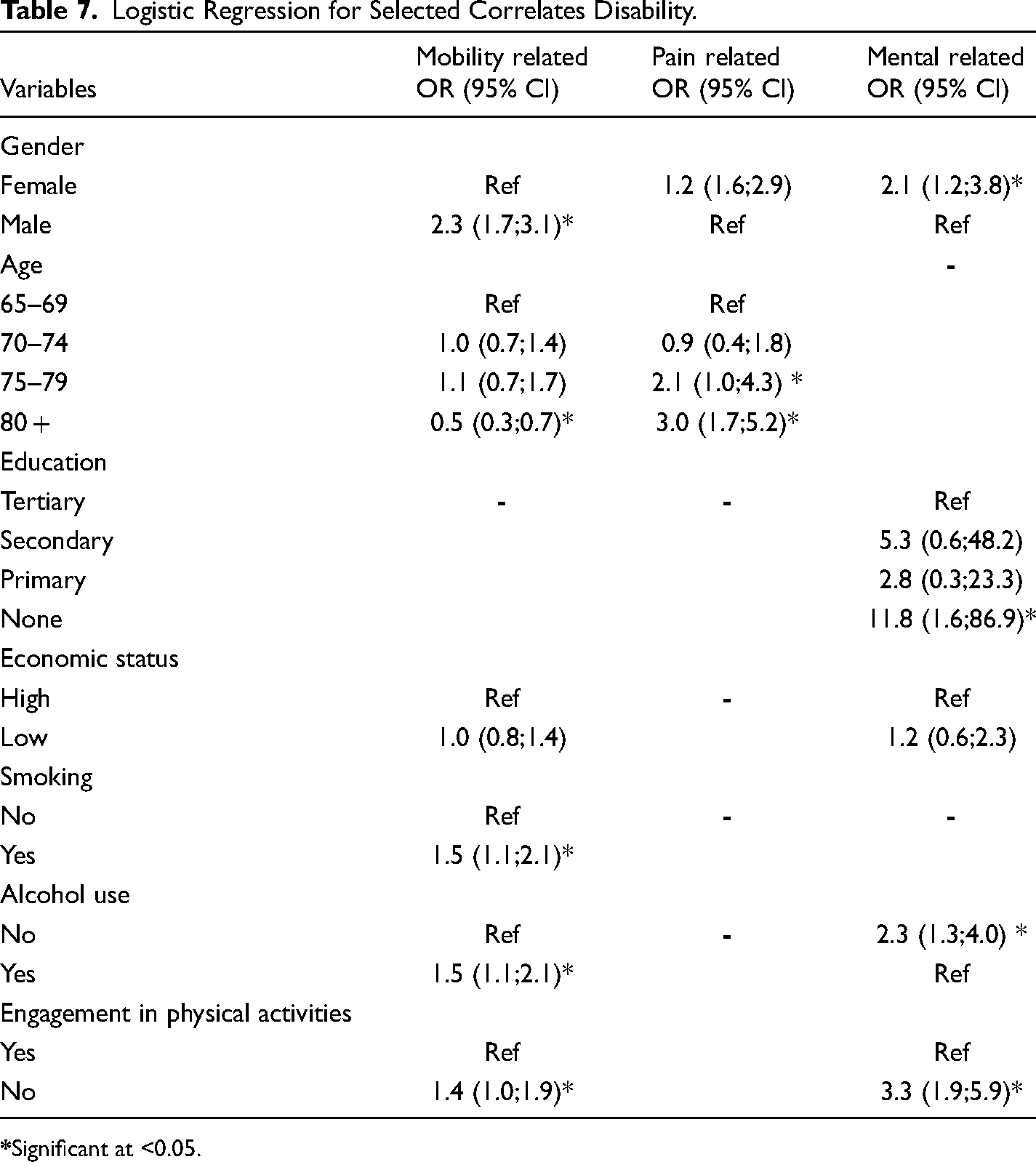
Logistic Regression for Selected Correlates of Disability
Compared to males, females were more likely to have pain and mental-related disabilities. As age increased, older adults in the most advanced age were three times more likely to have pain-related disabilities than other age groups. Although respondents’ aged 70 years and above had similar odds of having mobility problems, they were at a higher risk compared to those aged 65–69. Across all levels of education, respondents below tertiary education were at higher risk of having mental-related disabilities. However, those with no education were eleven times more likely to have this disability compared to all others. Use of alcohol, smoking, and engagement in physical activities were also significantly associated with some of these disabilities (Table 7).
Logistic Regression for Selected Correlates Disability.
Discussion
As observed, abuse occurs in a relationship of trust and causes harm that has some form of lasting impact (WHO, 2014). It is prominent among people with some form of vulnerability relating to disability, poor physical health, and mental disorder/depression; as well as individuals with financial incapacitation or low socioeconomic status (WHO, 2015). In less industrialized countries like Nigeria, abuse is not uncommon in older ages and many go unreported (Pillemer et al., 2016; Lachs & Berman, 2011). Respondents’ poor health status and an averagely rated quality of health care received is a reflection of the fragile health care system in Nigeria. This is further exacerbated by an out-of-pocket payment consequent upon the absence of social welfare and health insurance for older adults in Nigeria. Poor health among these older adults depicts co-morbidity in old age orchestrated by disability. Co-morbidity is facilitated by the environment with its disabling factors. In an Australian study, although about 40% of respondents had a severe disability, they rated their health as very good or excellent (Australian Bureau of Statistics, 2009) contrary to the present study. The WHO (2011) disability report stated that improved environmental factors can greatly enhance the health conditions of persons with disability through a public health prevention approach outlined as primary prevention, secondary prevention, and tertiary prevention. Primary prevention relates to raising awareness or sensitizations to avoid what causes a health problem before such begins. Secondary prevention is detecting and treating a condition early enough before it degenerates while tertiary prevention is prompt actions taken to treat a condition to reduce its already established impact on the body and prevent further complications as well.
Physiological changes and ageing precede the risk of deterioration of bodily organs and disability. Substantial evidence shows that disability associated with an increase in age (Wandera et al., 2014; Fried et al., 1999), leads to the inability or difficulty to live independently and perform ADL or IADL. Some factors such as gender, age, education, economic status, engagement in physical activities, and alcohol use were associated with mental related disability, particularly dementia. Females were twice more likely than males to have mental-related issues. In Azad et al. (2007), women had an increased likelihood of having dementia than males.
Respondents with a low level of education had a higher risk of having dementia compared to those with tertiary education. However, those with no formal education had twelve times elevated risk for dementia compared to others. In a systematic review on education and dementia, Caamano-Isorna et al. (2006) concluded that low education constituted a risk factor for dementia. Similarly, in a Chinese study, Zhang et al. (1990) found that a low level of education was a risk factor for dementia, and individuals with lower educational levels had a greater risk of dementia. Supporting this, the cognitive reserve hypothesis posits that certain life experiences cushion the effect of dementia. On this, Roe et al. (2007) hinged education as a predictive factor for dementia. Individuals with higher level of education or greater cognition, as stated, do not manifest dementia symptoms early as those with low or no education. Invariably,with our study's findings, we hypothesize that higher education may be linked with higher socioeconomic status and people with higher level of education are better able to deal with changes associated with age and take preventive or protective measures for their health. In other words, they may be more likely to adopt healthy lifestyles that have implications for mental health.
That respondents who did not use alcohol were twice more likely to have a mental-related disability (dementia) than those who used, may be suggestive that certain level of alcohol intake cushions the incidence of dementia in later years. According to Neafsey (2011), certain level or units of alcohol intake or limited drinking in earlier years may protect against dementia in later years. This evidence, however, does not obliterate the deleterious effect of heavy alcohol consumption beyond the recommended quantity per day/week.
Physical exercise significantly associated with dementia. Stated differently, physical exercise which may not necessarily be strenuous over a life course, protected against dementia and promoted health (Alexandre et al., 2014; Blankevoort et al., 2010; Boyle et al., 2007; Chow et al., 2012; Sjölund et al., 2015; King et al., 1998; WHO, 2011). In Norton et al. (2014), lack of physical activities contributed to about 20% risk of dementia. Thus, scholars (Fiatarone Singh 2002; Goldberg & Chavin, 1997; King et al., 1998; Mehr & Tatum, 2002; Spirduso & Cronin, 2001) recommended physical exercise to cushion the effect of disability in old ages.
Mobility-related disability, mainly stroke, associated with gender, age, economic status, smoking, alcohol use, and engagement in physical activities. In this study, stroke constituted the greatest burden of any type of disability and males had higher odds of having stroke than females. Similarly, Diep et al. (2010) reported that among older population, stroke constituted the greatest disease burden. In Wyller (1999) study, stroke was higher among males than females. While Gill et al. (1986) associated alcohol consumption as an independent risk factor, especially among males who are heavy drinkers or consumers of alcohol, it is recommended that further studies focus on predictors of this association. Occupation is significantly associated with stroke. On this, Wada et al. (2016) suggested that certain types of occupation may be a greater risk factor for stroke. We recommend more research to clarify the association. Like other studies (Shah & Cole, 2010; Shinton & Beevers, 1989), we found that smoking is a risk factor for stroke. Smokers were twice more likely to have stroke compared to non-smokers.
Finally, respondents also had a high burden of osteoarthritis/rheumatism (pain related disability) which was associated significantly with age and gender. While pain-related disability increased with age, females were more likely to suffer from it than males. This type of disability limits mobility, increases pain, decreases quality of life and may lead to depression as suggested by studies (Badley, 1995; Gabriel et al., 1997; Hughes & Dunlop, 1995; Katz, 1995; Verbrugge & Juarez, 2006).
Older adults in Nigeria live predominantly in rural areas and majority have no or low level of formal education. A greater proportion of the age cohorts have a disability related to sight, hearing, mobility, pain and mental disability. They have a medium to low socio-economic status and are predominantly farmers. They do not live in institutional homes and nine in every ten older adults prefer their individual homes where they interact daily with family members. While their experiences of abuse and property inheritance differ according to gender, they generally have poor health status. Their disability correlated with various socio-demographic, economic, and lifestyle variables. There is, therefore, a dire need for health promotion among older adults in southeastern Nigeria. We recommend community-based health care that incorporates informal caregivers. Since ageing is a life course phenomenon, integrating ageing into schools curriculum would help the teeming young population to prepare for old age, adopt healthy lifestyles that cushion disability in later years and avert their associated costs. It is important that the government considers formulating and implementing an old age welfare policy for older adults. This policy should be need-based and gender sensitive.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.