
Abstract
Programs and policies are increasingly framed by the logics of “evidence-based policy,” a term subject to critical scrutiny and change after it emerged as an explicit valuing of specific types of quantitative data as objective, and a devaluing of most types of qualitative data. The transfer of “evidence-based” approaches to drug policy was mobilized by a distrust of people who use drugs, and of people who work with them. This distrust remains important, but contemporary policy also mobilizes individual narratives and lived experience through the growing use of biographical stories. Contemporary drug policy, like other policy areas, is also increasingly constituted by changing forms of technology, through new types of data use and data linkage, and of digital and social media. In this article, we consider the current and likely future impacts of changes to policy. We examine two Australian policies: the Australian Priority Investment Approach to Welfare (Try, Test and Learn), and the child protection reform, Their Futures Matter. Both use the “investment approach” to calculate policy costs and aims, represent important developments in the policy figuring of populations, and affect the well-being of many people who use drugs. Based on analysis of these policies, and interviews with people who use drugs who participated in a qualitative study on blood-borne virus serodiscordance, we ask, what are the likely effects, risks, and benefits of these changes for people who use drugs and others subject to public scrutiny and distrust? We argue that as long as the stigmatization of drug use remains prevalent, it is unlikely that the potential for more sophisticated and just recognition of the complexity of drug use will find a place in the forms of information and knowledge recognized in policy as evidence.
Introduction
Drug policy is constituted by policy formation and implementation across several sectors, including health, justice, human services, housing, and education. One of the most important recent developments affecting these sectors has been the emergence of “evidence-based policy,” a term that organizes practices and debates around the types of information recognized as valid for policy. Evidence-based policy emerged from the discipline of medicine as an explicit valuing of specific types of quantitative data as objective and generalizable, and a corresponding devaluing of most types of qualitative data. Randomized controlled clinical trials are generally accepted as producing the “gold standard” of evidence in this paradigm, in part because they exclude, by design, social and contextual factors such as patient beliefs and therapeutic relationships (Tucker & Roth, 2006). The transfer of “evidence-based” approaches to drug policy was therefore mobilized by a distrust of the capacity of people who use drugs, and of practitioners who work with people who use drugs, to provide reliable accounts of their own lives. This distrust remains important, but contemporary policy mobilizes individual narratives and lived experience, through the growing use of biographical stories and case studies. Contemporary drug policy is also increasingly constituted by changing forms of technology, through new types of data use and data linkage, and the use of digital and social media.
In this article, we consider the likely impact of these changes to policy, especially on people who use illicit drugs and other marginalized groups. We examine two instances of the “investment approach” in Australian policy, both of which have implications for people who use drugs: the Australian Priority Investment Approach to Welfare (Try, Test and Learn) and the child protection reform Their Futures Matter. Based on analysis of these policies, and findings from a qualitative study on families living with blood-borne virus serodiscordance, we ask, what are the likely effects, risks, and benefits of these changes for people who use drugs and others subject to public scrutiny and distrust? How will the use of data-driven evidence alongside the use of lived experience work in practice? What possibilities are available to ensure that changes to policy incorporate both critical perspectives on human agency, subjectivity, and knowledges, and democratic principles of participatory policymaking? We argue that evidence-based policy is changing, and that two important yet contesting components of these changes are an increasing faith in actuarial models of calculation which take no account of social worlds, and increasing recognition of the place of lived experience and especially vignettes or summaries of lived experience. These changes are taking place in environments in which long-standing stigmatization of drug use remains prevalent. Without systemic changes to reduce this stigmatization, it is unlikely that the potential for more sophisticated and just recognition of the complexity of drug use will find a place in the forms of information and knowledge recognized in policy as evidence.
Background
In recent years, lived experience has been animated as a valuable and authentic source in social policy formation. Inspired by new social movements around race and gender, “consumer participation” first became highly visible in mental health and disability, and is now recognized as essential to both sectors (Shakespeare, 1993; Telford & Faulkner, 2004). It is also emerging in other policy arenas. People with lived experience of homelessness, out-of-home care, and prison are now invited to participate in policy and advocacy forums, as are representatives of Indigenous communities and LGBTQI communities (PIAC, 2019; State of Victoria, 2019). Although this recognition of the value of lived experience is far from routine in all policy arenas, it is now untenable for new policies to be implemented without at least a gesture toward consultation, collaboration, and, increasingly, “co-design” (Australian Government, 2019b).
These developments in policy sit alongside long-standing efforts in the social sciences and humanities to capture first-person stories of lived experience. Research methods in these disciplines are mobilized to do analytic justice to both experience itself and the strategies that people use to narrate it. This is particularly important and challenging, as Rance et al. (2017) argue for the lived experience of people who use drugs. That lived experience is shaped by intense social opprobrium and disadvantage, social forces that also produce and constrain narratives of the self. Storytelling is thus an intrinsically social process; so called “personal” stories necessarily reflect and incorporate wider social meanings, drawing on specific historical moments and sociocultural contexts. This, we contend, holds particular implications for those whose lived experience and identities are intimately bound up with a stigmatized social practice […] Struggles over narration therefore become struggles over identity. (Rance et al., 2017, p. 2224) This entails focussing on processes of identity production, insisting on the discursive nature of “experience” and on the politics of its construction. Experience is at once always already an interpretation and something that needs to be interpreted. What counts as experience is neither self-evident nor straightforward; it is always contested, and always therefore political. (Scott, 1991, p. 797)
The status of lived experience in policy is complicated by analyses of the contingent, political nature of experience. It is complicated further by the ongoing salience of far more skeptical attitudes toward experience. Part of this is distrust of the experiences and views of people who use illicit drugs, which manifests in multiple ways: People who use drugs are treated as duplicitous by health professionals and other institutional workers, their articulated needs and interests are re-interpreted by service systems, and their accounts of selves and lives are remade into narratives of trauma and delusion (Fraser et al., 2014; Fraser & valentine, 2008; Lancaster et al., 2015; for a remarkable corrective intervention, see Fraser et al., 2016). Part of this is a suspicion within policy and practice of experience in general as subjective and unreliable. The rise of evidence-based policy, which is now familiar as a term connoting technical standards of objectivity and empirical grounding, emerged as an explicit response to distrust of the experiences and judgments of practitioners (valentine, 2009). Clinical interventions and the administration of drugs, according to the rationale of evidence-based policy, could be consistently carried out across different locations and by different people because implementation of programs and administration of drugs was standardized and identical regardless of context. In contrast, policy interventions were based on opinions and stereotypes that could not be meaningfully tested in terms of implementation or outcomes, and could not be consistently replicated because practices changed according to context. The solution, according to the same rationale, was to eliminate the role of experience and judgment and standardize implementation of social programs.
Unsurprisingly, this very narrow definition of evidence and exclusion of human insight has been subject to sustained criticism, and our purpose in this article is to analyze some important ways in which evidence-based policy has changed over time and how it may further change. Our argument is that an important change is the presentation of evidence of lived experience and narratives of the self, which have specific and potentially very important implications for people who use drugs. This is because policy and other public discourses have strong traditions of valuing and recognizing particular types of biographical narratives of people who use drugs, which follow an arc of decline and redemption and a trajectory from “addict” to “clean.” All narratives of the self are formed by available frames and tropes. In the case of “addiction,” one of the most common of these are “stereotypical ruin-redemption accounts” (Pienaar & Dilkes-Frayne, 2017, p. 152) in which the former is characterized by the loss of the “capacity for self-control, autonomy and free will” (Pienaar et al., 2017, p. 520) and redemption by the resumption of economic participation and conformity to social norms. Such accounts are foundational to 12-step programs but are also more broadly familiar (Fomiatti et al., 2017, 2019; Keane, 2001). They tend to be characterized, as Fomiatti et al. (2017) argue, by critical turning points, and describe: a now familiar narrative arc: motivated by “rock bottom” experiences, individuals come to reject their drug-using lifestyles and gradually develop “non-addict” identities through participation in “normal” social relationships, practices and responsibilities. (Fomiatti et al., 2017, p. 175)
Method
This article proceeds in two distinct sections which have different data sources. The first is policy documents from two Australian initiatives which have been selected to demonstrate changes to the use of data and calculation in human services and welfare policy. They have been selected because they represent instances of new, data-driven policy, known as the investment approach. These areas of policy have significant impacts on people who use drugs, who are often specifically targeted by new modes of punitive welfare policies such as welfare quarantining and other forms of conditionality (Seear et al., 2018). The investment approach first became part of the policy agenda in New Zealand in the 1990s and has since been adopted in Australia. At Commonwealth level, the Australian Priority Investment Approach to Welfare and the programs and policies attached to it, the Try, Test and Learn Fund (Australian Government, 2019a) uses actuarial analysis to estimate Australia’s overall future lifetime welfare costs, the projected cost of future welfare payments to different population groups, and allocates funding to programs targeting those groups.
In NSW, Their Futures Matter, a child protection reform (NSW Government, 2019d), similarly uses actuarial techniques to calculate future costs for the population as a whole and specific population groups. In this case, costs include those related to government services that are the responsibilities of states and territories as well as Commonwealth welfare payments: those related to child protection, housing, justice, health, education, mental health, alcohol and other drugs (AOD), and parental risk factors (specifically mental health, AOD, domestic violence, corrections). Our analytic approach draws from the work of Suzanne Fraser, David Moore, and other critical drug researchers (e.g., Dwyer & Moore, 2013; Fomiatti et al., 2017; Fraser et al., 2014; Fraser & Seear, 2016; Lancaster, Ritter, et al., 2019; Pienaar & Dilkes-Frayne, 2017; Seear, 2020), who use the policy analysis tools of Bacchi (2015) and the theoretical frameworks developed by Mol (1999) and others to assess the realities made through policy practices: “policies, governmental technologies and other practices [form] an ontological politics that “enables some realities and disables others” (Lancaster, Rhodes, & Rance, 2019, p. 3, citing Mol, 1999).
The second source of data is from our own research project, My health, our family, the first study to document the experiences of families with mixed infection status, or serodiscordance, of blood-borne viruses in Australia. These included 31 people with one (or more) of the three blood-borne viral infections, of whom 19 were currently using drugs or had in the past, 15 family members, 15 people who fitted both categories. The parameters of “family” were self-defined by participants and included partners, parents, children, siblings, pets, and extended family, as well as families of choice, affinity, or intimate connection. The study received ethics approval from relevant institutions (see Acknowledgments).
As part of this study, in-depth interviews with people living with one or more of these infections, and with their family members, were conducted from 2017 to 2019 with 81 people in total. Data collection focused on the Sydney metropolitan area and surrounding regions in the state of New South Wales (NSW), which has the largest population of people with HIV in Australia, as well as a significant prevalence of hepatitis C and hepatitis B (Kirby Institute, 2017). Interviews were conducted either in person or by phone/video apps depending on preference. A semi-structured interview guide was used to explore the family impacts of diagnosis and disclosure, the relational dynamics of family life in the context of serodiscordance, how participants made sense of and responded to stigma and secrecy, and how families negotiate unfolding responsibilities associated with care and treatment. Interview recordings were transcribed verbatim, checked for accuracy, and de-identified. All participants were given a pseudonym. Transcripts were imported into the qualitative data software program QSR NVivo 12, to enable the data to be managed effectively during the coding process.
The scope of the study was much broader than the focus of this article, which uses illustrative vignettes from a small number of the participants who identified as current or previous drug users. This article is very selective in its use of data, as we explain in the Findings section. More complete analyses of the empirical findings, which draw more extensively on themes emerging from more of the interviews, are published elsewhere (Persson et al., 2019). That publication and other project outputs (Hamilton et al., 2018, Newman et al., 2019) reflect the project’s primary analytic tool of a coding framework, which was codeveloped by all members of the research team through multiple individual readings of transcripts followed by team discussions and agreement on optimal codes to capture key themes covered in the interviews. Our approach in this article is not thematic, but similar to that taken by Steggals and colleagues (2020), who also present vignettes of life histories. Our use of data is similarly “more theoretical than empirical [and] not intended to empirically establish our argument but rather help illustrate” (Steggals et al., 2020, p. 159) examples of specific types of narratives and their value in different contexts, as biographical strategy and policy story. As will become clear, our presentation of the data in the form of short summaries, highlighting specific episodes and events, resembles the presentation of lived experience in other formats, most notably policy documents.
Changing Evidence: New Policies and New Policy Models
As noted earlier, the emergence of evidence-based policy and in particular the privileging of randomized control trials as a means of generating evidence in social as well as clinical fields produced rigid hierarchies of evidence. These were mobilized in part by transparent devaluing of subjective experience and testimony. Evidence for policy and the field in which evidence can be seen to “count” has changed over time. Drèze (2018), for example, argues that the rigidity of attitudes is softening: Once upon a time, “evidence” was widely confused with randomized controlled trials (RCTs). The latter were held to be the paragon of rigour, and other forms of evidence, though not necessarily dismissed, were certainly devalued. Whenever observation, experience, reasoning or even statistical analysis suggested one thing and some RCT another, there was a tendency to assume that the RCT got it right [….] Today, the fever has come down and most economists would take a more nuanced view of what constitutes evidence. We also have a better understanding of the uses and misuses of RCTs. (Drèze, 2018, p. 45)
Distrust of the experiences and views of program and policy recipients, however, remains intact and may in fact be hardening. The investment approach to evidence-based policy is based on figuring welfare recipients in terms of costs, and setting policy aims as the prevention of future costs through the avoidance of future welfare payments. Economics has long had a place in policy design and evaluation and has long been subject to criticism for its assumptions and models of human behavior and decision making. It has also, however, developed measures of costs and benefits that account, in various ways, for the complex effects of interventions. The investment approach, however, is straightforwardly calculated in terms of money. When first introduced, it was specifically in terms of accounting: “We need new models and disciplines [that] borrow concepts from finance and accounting, something akin to a balance sheet, to recognise that long term dependency is a cost which will fall to future tax-payers” (Brown & Quilter, 1997, cited in Chapple, 2013, p. 57). The Australian policies that have adopted the investment approach to date feature this calculation approach as key components. Among their key outputs to date are reports produced by auditing firms: for the Commonwealth’s Australian Priority Investment Approach to Welfare by PwC, and for NSW’s Their Futures Matter by Taylor Fry, who also produced New Zealand’s first model in the 1990s (PWC, 2016; Their Futures Matter, 2019). The reports identify the elevated costs to society of groups of people with shared characteristics, named as “cohorts,” compared to a comparison group or the overall population. The Australian Priority Investment Approach to Welfare includes young carers and “at risk young people on income support,” Their Futures Matter includes children and young people affected by mental illness and vulnerable young people transitioning to adulthood; in both, alcohol and other drug use are identified as risk factors and costs.
As with another recent development, the use of wastewater analysis to track drug use (Lancaster, Ritter, et al., 2019), a notable feature of the investment approach, is the precision and finality of the figures they present, and the erasure of both the social contexts in which people live and the assumptions and methods used to produce the figures. The reports themselves are detailed with caveats and data limitations, and the Commonwealth report in particular requires literacy in reading statistical analyses and nonstandard graphical presentations. The findings, however, are consistently represented in policy documents, media releases, infographics, and bullet lists without these details (Porter, 2016, 2017). They are presented in dollar terms, with headline figures comparing the relative costs of welfare receipt, service use, and justice interventions between specified cohorts and the general population (see Figure 1).
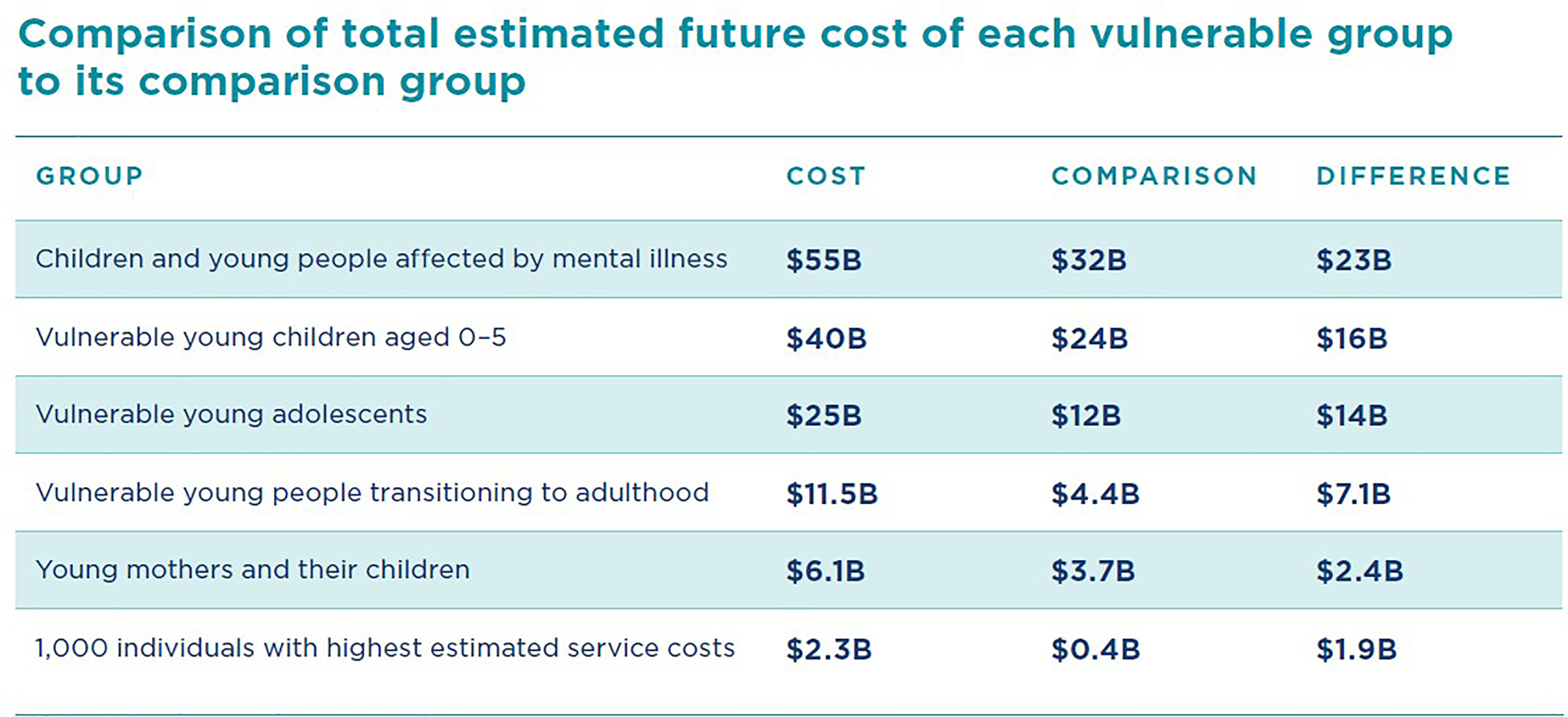
Comparison of total estimated future cost of each vulnerable group to its comparison group. Source: Their Futures Matter (2019, p. 20). © State of New South Wales through Department of Communities and Justice, licensed under Creative Commons Attribution 3.0 Australia License (https://creativecommons.org/licenses/by/3.0/au/legalcode).
The investment approach is notable as a new presence in evidence-based policy in at least two ways. First, it comes at a time when, as Dreze (2018) and others note, the claims for RCTs are being moderated by recognition of the importance of the social, and critical attention to policy design and implementation. The investment approach, in contrast, represents new modes of figuring populations which reify objectivity, depersonalization and the evacuation of the social.
The second notable point how this figuring is mobilized is by its privileging of the future at expense of present experiences: Actuarial modelling is claimed to “allow us to look into the future and see where we are headed” (Australian Government, 2019a). The Australian Priority Investment Approach to Welfare and Their Futures Matter both emphasize intervening early in the lives of specified groups of people, especially young people, to prevent their trajectories following those of others. Policy is framed primarily as a means to avoid costs and outcomes, that is, to avoid the very existence of those adults who now cost so much. (As it happens, the argument that vulnerable people are more expensive than privileged people in terms of public expenditure is inaccurate, but this is not relevant for our purposes here, Whiteford, 2015). This emphasis on the future is found in other examples of policy exhortations based on modelling and assumptions, as Lancaster et al.’s (2019) analysis of the WHO’s Global Health Sector Strategy on Viral Hepatitis shows. Targets for global incidence and treatment rates for viral hepatitis figure time as “an actor in the making of elimination, helping to constitute imagined futures. Indeed, what is rendered in these targets is a shared, universal future as much as an urgent concern in the present” (Lancaster, Rhodes, et al., 2019, p. 5). Futurity is a means of orienting present practices toward a sense of urgency and a need to act now.
In the context of policy targeting marginalized groups, including people who use drugs, the implications of this figuring of the future are especially fraught. Public discussions of people who use drugs are often marked by the devaluing of their citizen entitlements, including respect (Seear, 2020). It is surely no coincidence that the policy documents identify the vulnerable cohorts as “future liabilities,” an overt naming of people as costs rather than citizens, and an overt casting of people as damaging the future. As Edelman’s (2004) psychoanalytic readings of futurity and queer politics demonstrates, public politics is mobilized by the future, represented by “the Child.” This is a figuring of “an ideal, entitled to claim full rights to its future share in the nation’s good, though at the cost of limiting the rights ‘real’ citizens are allowed” (Edelman, 2004, p. 11). The reliance on futurity and future children for an imagining of public good always has costs for actually existing adult citizens, whose own needs are rendered invisible. Edelman shows that the costs are higher for those adult citizens who are marginalized and often despised because they are, in these constructions, something like a threat to the future being imagined.
Yet the question of representation in these new modes of policy is complicated by the presence of different figurings and language. The models that cast people as costs are interspersed with instances of lived experience. One instance of this is an emphasis on participation. The Australian Investment Approach to Welfare cohort reports are accompanied by funding initiatives that privilege co-design, community participation, and “an open and collaborative approach [….] Co-development activities are embedded” (Australian Government, 2019c). Even more striking is another feature of ways that policy discourses have changed, the increasing use of images and video. In particular, Their Futures Matter includes vignettes and quotes from individuals and families, illustrated with photos. One page, describing a program for families who are at risk of their children being removed, for example, is introduced with a quote from “Mum”: “At the first meeting we felt that [the program] was something completely different that we have not been exposed to before and we felt that the weight has been lifted off our shoulders” (NSW Government, 2019c). The website also features several de-identified (i.e., the names are pseudonyms) vignettes. Prior to starting [the program] Eva, a single mother, had her two-year-old son in her care and her five-year-old daughter in the long-term care of her maternal grandmother. Eva’s daughter had very limited supervised contact, seeing each other three times per year. With the family’s [program] therapist’s support, Eva has developed a range of relapse prevention strategies, which she uses if she is triggered. This includes going to the gym and connecting with other people in a support group. She now has a leadership role in this group which she enjoys. As a result of this support, Eva has been granted bi-monthly unsupervised contact with her daughter. This has strengthened the siblings’ bond. Eva is very excited for every visit and grateful for her therapists support and understanding. She has put her son into childcare two days a week, is looking for a stable job and has commenced studying a Certificate IV in Community Services. As a result of the family’s achievements, [the statutory child protection agency] have completed a risk-reassessment and have decided to close the case with the department. (NSW Government, 2019a) The Taylor family was referred to [a program] due to domestic violence and the father’s drug use. Despite these pressing issues and facing homelessness, like many other mothers in a similar situation, Kelly avoided involvement of [the family support and statutory child protection agency] Family and Community Services (FACS) due to her fear of having her three sons taken away and having to return to her home country – New Zealand. “Understanding their cultural background played a vital role in helping this family,” explained FACS case worker. The family was matched with Jacqui [a program therapist], with Pacific Islander background (Samoan), who effectively engaged with both parents. Jacqui’s understanding of Kelly’s strong ties to her Maori family and her heritage helped to break the barriers and earned the family’s trust. (NSW Government, 2019b)
The investment approach, then, is not a straightforward story of the social being erased, and it differs from older models of evidence-based policy. On the one hand a new instance of an already important trend of data-driven policy, it is on the other hand a new mode of using and appropriating narratives of individual experience. Older models of evidence-based policy are transparently dismissive of individual stories and subjective experience, with “expert” opinion at either the bottom of evidence hierarchies or excluded altogether, and lived experience invariably excluded. In contrast, Australia’s investment approach accompanies data with narratives and recognizes lived experience as important. Yet the types of lived experience presented are narrow, aligned with the policy goals and supporting the program activities associated with those goals, and render invisible those aspects of lived experience that are not presented. The presentation of familiar narrative tropes of rescue and redemption in the same policies as the presentation of people as future liabilities points to particular narrow uses of lived experience, in which narratives are used to illustrate an agenda of presenting people who use drugs as costs and the goal of policy to prevent this happening. It is difficult to see how alternative narratives, and narratives of alternative ways of being, could have a place here. Life stories, we argue in the next section, are more complicated and offer more possibilities than these presentations allow.
Change Narratives: Biographical Summaries
In this section, we present our own data from the research project described in the Methods section. We use data from the interviews in vignettes which are presented as illustrative and have been constricted to resemble the summarizing of life histories and significant events that are used in other formats, including websites (Pienaar & Dilkes-Frayne, 2017) and the policy documents we described in the previous section. In this, we acknowledge that we are purposively selecting quotes and constructing life histories from a very large, heterogeneous data set. We also acknowledge the injunction by Rance et al (2017, p. 2230) to recognize our roles as researchers in mediating these narratives: “in the face of the vulnerability and trust so often granted us by participants, we need to recognise not only our role in the making of people’s stories but our responsibility in the interpreting of them” (see also Pienaar & Dilkes-Frayne, 2017). While we have honored, to the best of our abilities and understanding, the priorities and views of our participants in presenting these vignettes, it is not possible to fully represent the complications of the themes and tropes in their interviews and all the nuances of their narratives.
The primary analytic mode for the overall project was thematic rather than the rigorous construction of case studies (Thomson & Holland, 2003), and we do not claim that the vignettes presented are case studies (as we noted in the Methods section, other publications from the project reflect that thematic approach). Instead, the vignettes were constructed from the data to summarize and synthesize the narratives of many participants, which took place over decades and featured significant life-course events. When these narratives were distilled into short biographical summaries, they were then subject to multiple editing and filtering decisions, both deliberate and unconscious, and these decisions are not visible in the narrative. In acknowledging the specificities and limitations of the vignettes, we make the point that this use of biographical summaries is an increasingly common practice and that the methods of selection and extraction are rarely acknowledged in policy and other public communications.
The vignettes are presented to illustrate the multivalence of individual experience. They evidence the richness and particularity of individual experiences and the strategies used by people, at points in time and over time, to manage and make sense of those experiences. They also reveal the narrative tropes and strategies that are available to people, and that the integration of events into narrative is often enabled the use of familiar tropes, including transformation and redemption, or alternatively, ongoing trauma and damage (valentine & Fraser, 2008).
We present three vignettes, distilled from the interviews with George, Jackie, and Emily. In each case, we note the available narrative frames and tropes that organize their stories, and describe the elisions and gaps that the use of these frames inevitably produces. Trajectories of recovery and stories of trauma are powerful ways of telling an individual story, but doing so is also a necessary neglect of alternative stories.
George
George was in his mid-60s when we interviewed him and he described a long history of hepatitis, being first diagnosed with hepatitis B, hepatitis non-A non-B, and hepatitis D as a child as a displaced person in the Middle East. He thinks that he was probably infected with hepatitis C through injecting drugs, which he did from teenage years to adulthood, and he was formally diagnosed with hepatitis C in the early 1990s. He became very unwell around that time and was told he would likely die within five years. He was put on Interferon; “among the worst things I’ve ever had to endure in my life.” He “started dying” with “end-stage liver disease” after his unsuccessful treatment. He had a successful liver transplant a few years later, which he reports cleared all the various hepatitis he had.
He now works in the blood-borne virus sector, including as a public speaker, particularly focusing on stigma. His health is very important to him now, and he regularly attends the gym. End-stage liver disease, unconsciousness. I’m dying. They transplanted me in 1997. Successful transplant. I’m their star performer. Had to deal with a huge amount of immuno-suppressives. Then the miracle happened. They said, “We don’t know what’s going on here but you don’t have any hepatitis. Your body has cleared itself of all hepatitis.” [….] So I cleared the virus. Dealt with the medication. Gradually reduced. Spent 15 years in the gym. Got back into life and it’s been a very uphill journey. I’m their star performer they tell me. Very successful transplant. I’m 68. I’m very fit, strong.
George’s story uses ideas and tropes of transformation through recovery. The specific events of his life are organized into a narrative arc: from a low point of near-death to his current well-being, his story is of leaving behind ill health and drug use, and now of sharing that experience through working in the sector. His story is also imbued with the poignancy of his wife’s experience. Yet this narrative is also more complicated than a straightforward summary of redemption would allow, which can be illustrated in two ways. First, George declines to express regret and remorse for his history or to describe it as deviance. Instead, he describes his drug use as “naughty” and generative. “I wouldn’t change anything. I wouldn’t change a thing what happened to me because it all went to make me what I am today. So…You know what I mean? It was meant to be.” Second, in contrast to common accounts of isolation and estrangement, George reports that family support and connection has been important to him throughout his life. His wife, mother, and children have long known about his drug use and were hugely important during his transplant. They supported him a lot during this time, and he describes his mum as a “trooper.” He thinks while it must have been really hard for them to see him so ill and close to death, it also made the family very close and very honest and open. The family still celebrates his survival with a “significant occasion” each year to ensure the experience is memorialized down the family line, and George’s dedication to his health has inspired his grandchildren to be active in playing sport and cultivating their own physical fitness.
Jackie
Jackie was a transgender woman in her late 40s when we interviewed her, and she described a harrowing life story characterized by drug use and other “risky” practices, contextualized by ongoing trauma and betrayal. Well, I was abandoned at birth. And then I was like, yeah, I went to my grandmother until I was one…. And I went to my dad’s brother and his wife, and the wife chained me up under the house until I was four and a half, on a lead. And then I went to my great aunt and I had to have like speech therapy and learn how to talk and that. Then I was molested from five years old. Yeah. And it goes on and on.
Jackie’s story is one of early trauma compounded by later abuse and deprivation, in which drugs can be understood as a response to adverse circumstances and a way of managing them. Hepatitis C and HIV infection were both cause and consequence of social and economic immiseration for her. Her story is at once deeply personal and highly social, and in its description of drug use as subsequent to trauma, aligned with discursive associations between drug use and personal adversity. Like George’s story, however, Jackie’s narrative is more complicated than any straightforward summary of trauma, fall, and recovery. While extremely distressing, her narrative describes achievements and strengths, which happened because of, rather than in spite of, her circumstances. She’s now a peer support person with people who use drugs and have hepatitis C and supports people to go on treatment. As a peer worker, she is part of a team making significant contributions to the viral hepatitis “elimination agenda” of recruiting as many people as possible to treatment. And in my last meeting that we had, they were saying about the hep C things, people being, the numbers being low. It’s because we’ve cured, had over 700 of our clients on treatment and cured. Like, you know. So that’s why it’s so thing, yeah. Well, everyone’s spinning out because there’s not many people coming, wanting to access it. And it’s because we’ve done them all. When you’re on hep C treatment, you’ve also got to think of your mental, your mental state of mind. And [friend] was always there to make sure my mental state of mind was in check. So they were always there to pick me up when I was falling again…they also made sure I ate and that I ate every day. And [friend] would always give me a blanket or something to, so, if…we were going to be sleeping rough that night, there was a blanket there for us.
Emily
Emily was in her mid-50s when she took part in an interview, and she had been diagnosed with hepatitis C in the late 1990s. She was working in the blood-borne virus sector and had recently undergone DAA treatment. For some time after diagnosis, hepatitis C did not occupy a large part of her life, and Emily reported that her doctor downplayed its significance and she “de-prioritized” it for many years. More recently, she explained that despite her own experience of cure, hepatitis C has become “quite huge all around me,” as knowledge and science has evolved. Several of her friends have hepatitis C and are struggling, which she feels is being silenced by the contemporary “elimination agenda” and the dominant discourse of treatment optimism, “it’s kind of turned into this, you know, massive thing…But it’s just kind of ironic because it’s this thing that I didn’t really figure was going to play such a big role in my personal life.”
Emily was estranged from her sisters and mother for a long time because of her drug use. She had “started to reconcile a bit with my family” after her sisters agreed to have a relationship that was open and honest about drug use and hepatitis C. She felt that hepatitis C treatment was a “safer narrative” for families than drugs, and believed her sisters probably now saw her treatment and cure as a kind of recovery, perhaps because of Emily’s refusal of a redemption story. I think it might give them a bit of a kind of, you know, redemption edge that they can cling onto or something, you know? Because I won’t play into that otherwise in terms of my drug use, you know. I’m not the recovering drug user or anything. But I think they sort of see me, “Oh, you know, you don’t have hep C anymore,” you know. “That’s a good thing,” you know. And I know other people who talk about that with their families, that they even do treatment at all because they think it’s going to change the way that their families view them: that their families will view them more positively and be able to put that aside, you know, that history aside a little bit.
The life summaries from George, Jackie, and Emily reveal different experiences, and in turn different possibilities for their representation as narratives. George and Jackie provide complicated, nuanced biographical accounts that require time and skilled reading for comprehensive understanding, and are stories that lend themselves readily to tropes of “authenticity” because they provide a chronology, evoke similar narratives, and offer hope as a function of recovery. Their stories are recognizable as representative of particular kinds of experience. As we have argued, however, this representation requires us to neglect attending to those parts of their accounts that do not “fit”: George’s declining to regret his drug use or associate them with isolation, Jackie’s strengths and achievements as a peer worker. The narratives of other participants were less available to appropriation: This is not to argue that the experiences that they represented were more or less complicated than George and Jackie’s, but that the form and content of their stories were notably different. Emily, as described above, explicitly rejected a redemption narrative. Other participants provided biographies that were chronologically fragmented, hesitant, or otherwise difficult to represent in summary form. They provided accounts that are productive and rich for thematic analysis in qualitative research (see Persson et al., 2019) but would be less useful for websites or policy documents. To return to the questions we raised earlier about the potential risks and benefits of increasing use of lived experience in policy: in the absence of systemic efforts to represent narratives of drug use that fall outside dominant tropes of redemption and trauma, one likely effect is that these narratives will not be represented in policy representations of lived experience. The potential risks of lived experience finding a greater place in policy are compounded by the exclusion of both the processes by which lived experience vignettes are composed, and the parts of life that do not fit policy goals. They are compounded still further by the implications of the investment approach to policy: So far, the evidence suggests that representations of lived experience will be those that align with the logic that the primary aim of welfare policy is preventing costs.
Conclusion
The vignettes we present here are from a research study collected for specific purposes and necessarily translated and changed through the process of transcription, coding, and editing. Our ongoing responsibilities as researchers are to represent the stories of our participants as they choose to tell them, and to frame their stories with analysis that contextualizes their accounts and deepens our understanding. One of our concerns is that these responsibilities are not shared by others who tell the stories of vulnerable people in public forums. Research is always imperfect and incomplete, but it affords certain protections, not least through its constraints: Researchers are always limited in the claims that they can make, especially when it comes to the “real lives” of research participants. The use of biographical narratives in policy is generally not framed by the same constraints.
Critical policy research has long called for, and itself demonstrated, the benefits of a wide analytic lens in understanding biographical narratives. Such analysis allows, inter alia, the incorporation of structural drivers of disadvantage and marginalization, the ongoing creation and recreation of resilience, strengths and capacities, and the possibility of alternative stories to those which are commonly told of deficit and pathology (Chandler et al., 2013; Ferguson et al., 2019; Fernandes, 2016; Fine, 1995; Fraser et al., 2016). This critical analysis remains vitally important: Our primary argument here though is that contemporary policy developments, including the use of lived experience, may change the tasks and barriers associated with it.
As noted earlier, digital stories are an important phenomenon in the changes occurring in policy and research and are associated with hopes for more inclusive and diverse representations of lived experience. Yet just as the hopes for the democratizing and emancipatory potential of web-based media have been disappointed, it is also possible that the potential benefits of the increased presence of lived experience in drug policy will be countered and undone by its appropriation toward the status quo. In a critical analysis of lived experience narratives in policy, Sujatha Fernandes argues that lived experience narratives are becoming more important in public forums and that these narratives are almost always circumscribed by the narrow range of tropes and frames used to structure them. Social media and other technology are enabling digital stories in the public sphere to become ever more present, she argues, and this is rarely acknowledged as a specific mode of instrumental or “curated” stories (see also Sunderland & Matthews, 2019). Curated stories generally individualize social structures and interpret adversity in terms of private or personal circumstances. Fernandes’ analysis of the accounts of low-paid workers, people living in war zones, activists, and victims of violence are all rendered familiar through narrative conventions and explanatory tropes: “histories, ambiguities, and political struggles are erased in an effort to create warm and reliable portraits of others who are “just like us” (Fernandes, 2017, p. 2). In addition, while digital storytelling is often conceptualized as a way for people to tell their stories, in policy and research this is not the case: Digital stories in these arenas are directed by and produced for others. Curated stories on the Their Futures Matter website are designed to look like people telling their stories, and not designed to reveal the selection, production, and editing of those stories, nor to acknowledge the use of these stories in promoting a policy agenda which calls people who use drugs “future liabilities.”
The technologies of representing lived experience illustrate the broader potential benefits and risks to the interests of drug users in new forms of evidence-based policy making. Evidence-based policy is changing, but remains animated by a strong privileging of particular types of data, and, in the investment approach at least, a very narrowly defined definition of policy success. What would it take for the potential benefits of policy changes to be realized? First, it is necessary that the participation of people who use drugs in politics and policy is made genuinely available, and not just through the retelling of their stories by others. Stories, digital and otherwise, of lived experience are valuable contributions to knowledge and to the policy process, when space is made available to listen to those with lived experience and allow the authorship of their own stories to be recognized (Matthews & Sunderland, 2017). The capacities of people who use drugs to contribute to decisions made that affect them, and their entitlement to do so, have long been argued. The democratization of biographical narratives through digital forms, and the deliberate adoption of these forms in policy, may make this participation possible. The benefits of this participation will only be realized, of course, through responses on the part of policy and others, a first step in which is active listening to these stories (Dreher, 2009).
The risks come from the legacies of deep distrust of drug users and from an emphasis on appropriating authenticity and lived experience for policy, but in limited ways. First, there is a risk that the diversity of experience will be rendered invisible. While policy formation is undoubtedly strengthened if people who use drugs are genuine participants in the process, the experiences of a single person or group of people cannot be representative of the entire population. The needs and desires of people who use drugs are vastly diverse, as is the place of drugs in their lives. Any attempts to represent all of them will necessarily erase or distort some of them. Second, there is a risk that first-person narratives of lived experience are received as authentic, unmediated testimonies and the methods and decisions behind their production are made invisible. In part, this is because these narratives stand in stark contrast to the supposedly objective, and inarguably far more distant and impersonal, accounts produced in orthodox research outputs and policy documents. Compared to these latter accounts, first-person narratives are far less mediated and far more authentic, and it is a matter of social justice that the voices of those who have been ignored for so long are listened to with respect and without interpretative overlay. When arguing that narratives are inevitably mediated and framed, we are also making the point that this is a matter of degree. First-person narratives are not unvarnished truth, but they are certainly more authentic and less mediated than representations of experience made by policy makers, or for that matter by researches. It is important to reiterate here the reasons for the emergence of lived experience and participation in policy making in the first place. The involvement of people who use drugs in decisions that affect them is important as a matter of democratic principle and human rights, but also because so many of these decisions are based on disrespect, misrecognition, and narrow standards of normative practice. The vignettes presented here are evidence of the complicated lives and resilience of people who use drugs and people who face adversity. They show the ongoing failures of services and systems to meet the needs of people, for example, the repeated failures of services to protect Jackie as a child and the ongoing stigma toward hepatitis C reported by Emily, and the ongoing effects of these failures. They demonstrate the need for spaces in which people who use drugs can speak, and just as importantly the need for policy forums that have the capacity to actively listen to those voices (Bryant et al., 2008; Dreher, 2009; Rance & Treloar, 2015). Scott’s (1991) point that experience is something to be interpreted is important here: The experiences of people who use drugs should be significant influences in processes of change.
Equally, Scott’s point that experience is itself a process of interpretation is important. The voices of lived experience, in research or other forms including digital stories, are not straightforwardly direct and true accounts. Accounts of the self are mediated by the narrative frames that are available, and in the case of people who use drugs, the narrative frames that are most available are formed by dominant tropes of stigma, trauma, damage, and deficit. This is not universally the case, of course, and alternative narratives are possible in both the direct accounts of people who use drugs and through processes of mediating and translating those accounts. Nevertheless, the preponderance of stories recounting drug use, or disadvantage, or adversity, are framed by a narrow range of tropes. The growing place of curated stories makes it ever more likely that particular types of narratives, that fit a conventional account of individual deficit and rescue or redemption by beneficent services and support, are the only narratives presented as authentic accounts of experience in policy forums. Researchers and others with accepted roles in policy making have an ethical responsibility, we think, to ensure that the tasks of rigorously translating experience into evidence are incorporated into policy changes, and that the diverse and complicated lives of people who use drugs are richly present, not flattened into case studies, in these processes.
Footnotes
Authors’ Note
The views expressed herein are those of the authors and are not necessarily those of the Australian Research Council. The contributions of the investigator team were supported by the Centre for Social Research in Health and the Social Policy Research Centre at UNSW Sydney, both of which receive some support from UNSW Arts and Social Sciences, and by the Australian Research Centre in Sex, Health and Society and The Burnet Institute. All of these research groups receive funding from a range of external agencies.
Acknowledgments
Many thanks to all participants with lived experience, their families, and stakeholders, who generously shared their time and stories with us. Thanks also to the members of the project Advisory Committee, and other partner organizations who supported us with recruitment, including: ACON; Carers NSW; Concord and Canterbury Hospital Gastroenterology Units; Hepatitis ACT; Hepatitis NSW; Hepatitis SA; Illawarra Shoalhaven Sexual Health Service; Kirketon Road Centre; Multicultural HIV and Hepatitis Service; Paediatric HIV Service, Sydney Children’s Hospital; Positive Life NSW; Pozhet (Heterosexual HIV Service of NSW); Prince of Wales Hospital Liver Clinic; Relationships Australia NSW; Relationships Australia SA; Royal Prince Alfred Hospital Gastroenterology Unit; Royal Prince Alfred Hospital Sexual Health Clinic; St George Hospital Liver Clinic; Sydney Sexual Health Centre; and The Albion Centre. Research support and other key contributions were also provided by Dr. Kerryn Drysdale, Dr. Rebecca Gray, Dr. Jessica Botfield, Dr. Jake Rance, Dr. Lise Lafferty, and Ms. Jialing Cui.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported under Australian Research Council’s Discovery Project funding scheme (DP160100134).