
Abstract
Substance use treatment services in Canada have historically relied on professionals with lived and living experience of substance use and recovery. This qualitative study explored how 22 such professionals working in one prairie province navigated the demands of their professional roles. The unique contribution of this research lies in situating those experiences within the context of health service delivery in geographically dispersed, rural communities characterized by managerial approaches and resource limitations. Findings indicate that firstly, professional maturation and longer time in the field were related to self-disclosing one's recovery status less frequently and more intentionally; secondly, burnout and stigma related to fewer confidential supports in rural community recovery networks shared with service users can unbalance one's recovery and professional roles; thirdly, the narratives of self-care, individual growth, and self-sufficiency were considered a way to overcome work-related pressures; and fourthly, participants reported using their experiential knowledge of substance use and recovery along evidence-informed practices in their professional capacity. The findings suggest the need to recognize recovery as a continuum and to provide tailored, localized supports and other specialized substance use services for substance use professionals with lived experience and living experience.
Keywords
Introduction
Substance use treatment services around the world have traditionally employed counsellors or professionals in equivalent positions with lived or living experience of substance use and recovery. This phenomenon has created professional workspaces where personal and professional aspects of one's life become closely intertwined (Best et al., 2016; Curtis & Eby, 2010; Doukas & Cullen, 2010; Ducharme et al., 2008; Janikowski & Glover-Graf, 2003; Knudsen et al., 2006; McGrath & DeDiego, 2023; Oberleitner et al., 2021). Research from various counselling practice domains indicates that counsellors’ well-being is important for their counselling effectiveness), with psychotherapy or other personal supports significantly enhancing their professional functioning (Lorentzen et al., 2011). Additionally, work-related training, support and supervision, shared values, ethics, and reflection foster a greater sense of belonging to the professional community (Dollarhide et al., 2023).
Counsellors with Lived Experience and the Continuum of Recovery
Substance use counsellors with lived experience must balance multiple networks and role adjustments as they develop their personal and professional identities (Best et al., 2016; McGrath & DeDiego, 2023). Social identity transformation of substance use professionals in recovery often involves adopting new values and norms aligned with recovery-based social systems while managing the demands of their profession (Best et al., 2016; McGrath & DeDiego, 2023).
Historically, research on substance use counsellors in recovery focused on identifying their characteristics and how their lived experience is related to their clinical work (Chapman et al., 2019; Doukas & Cullen, 2010, 2011; Ham et al., 2013; Hanson, 2005; Hecksher, 2007; Jones et al., 2009; Knox and Hill, 2003), the issues of self-disclosure in a clinical context (Dilts et al., 1997), and clients’ perceptions of their clinical effectiveness (Culbreth, 2000). Despite the common belief that counsellors with lived experience have some professional advantage over counsellors without recovery experience when providing treatment, the research evidence has been inconclusive (Chapman et al., 2019; Doukas & Cullen, 2011; Eddie et al., 2019). Some studies reported additional benefits to clients’ perceptions of their recovery journey when counsellors had personal recovery experiences (Conti-O’Hare, 1998; Jackson, 2001), whereas others did not find that clients’ therapeutic outcomes improved due to counsellors’ lived experience (Culbreth, 2000; Eddie et al., 2019). Earlier research identified challenges such as overidentifying with client experiences, difficulties maintaining professional boundaries, and a lack of support to prevent personal relapse (Doukas & Cullen, 2011; White et al., 2003). Additionally, research showed that recovering counsellors tend to have less education compared to their non-recovering counterparts, and their personal recovery experiences influence their clinical decision-making. For instance, studies that observed a tendency among counsellors in abstinence-based recovery to favor abstinence-based treatments highlight distinct professional development and clinical practices within this group of service providers (Crabb & Linton, 2007; McGovern et al., 2004; Morgenstern et al., 2001; Novotna, Dobbins, Henderson, et al., 2015; Novotna, Dobbins, Sword, et al., 2015; Oser et al., 2011; Sias et al., 2006).
The evolution of treatment interventions, notably framing recovery as a continuum rather than a use/no use dichotomy, has moved substance use treatment beyond the mere symptom suppression to consider overall health, increased quality of life, and engagement in a solutions-based recovery (Bartram, 2021; el-Guebaly, 2012; White, 2015). The conceptualization of recovery as a sustained effort to improve one's well-being has facilitated greater involvement of individuals with both lived and living experiences of substance use and recovery. Additionally, the expansion and “normalization” of harm reduction services and broader recovery perspectives have created more opportunities for individuals with lived experience to participate as peer supporters or substance use counsellors. Notably, opportunities for engagement, mentoring, and training peer support workers have led to positive outcomes for service users by allowing them to share relatable perspectives and experiences (Bucur et al., 2020; Crowthers et al., 2022; Francia et al., 2023).
Substance Use Treatment Field in the Contemporary Context of Neoliberal Health Services
Despite more inclusive views on recovery and the broadening of the definition of success of provided interventions (Bucur et al., 2020; el-Guebaly, 2012), funding cuts to substance use services (Elliott, 2014), and crisis-driven financial supports for public health needs related to substance use negatively impact the substance use workforce (Canadian Centre on Substance Use and Addiction, 2021; Ross et al., 2022; Strike & Watson, 2019). System fragmentation and the stigma surrounding substance use treatment and recovery efforts hinder access to support for professionals with lived experience, as well as their potential to bridge the gap between service users and service providers (Eaton et al., 2015; Oberleitner et al., 2021). Amid limited support and tailored supervision, substance use counsellors with lived experience are often expected to demonstrate organizations’ commitment to bridging the gap between service users, while their experiential knowledge is simultaneously undermined as being too relational, client focused, and community driven (Bell et al., 2025). These tensions, so common within neoliberal health care, are then addressed through increased credentialing framed within formal quality assurance models (Carton, 2018; Lewiskin et al., 2021). The process of professionalization functions both as a regulatory mechanism and as a form of gatekeeping (Oberleitner et al., 2021; Silcox & Stewart, 2024), transforming lived experience into standardized labor, legitimized through educational credentials. In line with trends across other nonprofit sectors (Baines, 2010), experiential or tacit knowledge is incorporated into measurable competencies and outcomes aligned with neoliberal models of service efficiency (Ross et al., 2022). In Canada, individuals with lived experience have long been part of the country's substance use workforce, with the highest representation recorded in the Prairie provinces, almost 50% (Doukas & Cullen, 2009; Ogborne & Graves, 2005). Rural regions in general, characterized by vast geography and low population density (Statistics Canada, February 9, 2022), have typically high levels of stigma associated with substance use and recovery, resulting in poorer psychological well-being and decreased self-efficacy and self-esteem that ultimately influence the provision of and access to substance use services (Bartram, 2021; Miller et al., 2024).
Overall, substance use interventions in countries of the Global North often prioritize cost savings, performance efficiency, and individual responsibility when addressing adversity. These priorities frequently come at the cost of access to comprehensive and equitable substance use treatment services (Lewiskin et al., 2021; Moallef et al., 2021; Ross et al., 2022). The conflict between managerial control and public health ethics of substance use is evident in Canada, where discourses on individual responsibility conflict with ethical duties to protect everyone through appropriate public health measures (Hardill, 2019; Kusdemir & Oudshoorn, 2023). Given the evolving concepts of recovery and the influence of neoliberal policies on local service delivery, it is crucial to examine how professionals with lived experience leverage their experiential knowledge to inform interventions, supervision, and other forms of support at both individual and organizational levels.
Research Method
Qualitative health research provides a much-needed understanding of the processes underlying patterns of behaviors and detailed descriptions of the phenomena under study. We used the principles of qualitative thematic analysis (Braun & Clarke, 2006) to provide an insightful exploration of the personal substance use and recovery experience in relation to the research participants’ personal and professional well-being and development. Thematic analysis is a systematic yet flexible approach for identifying and analyzing patterns in data to gain a deeper understanding of the phenomenon under study (Braun & Clarke, 2006; Flick, 2018).
Purposeful sampling (Flick, 2018) was used to recruit substance use counsellors (or individuals working in equivalent positions) with personal recovery experience while stratifying the sample based on the following characteristics: community (urban, rural/remote); treatment modality (residential, outpatient, methadone, and related harm reduction approaches); and type of personal recovery experience (abstinence based, medically assisted, or moderation/controlled use based). The invitations to participate in the study were sent to a publicly available list of substance use treatment agencies across the province of Saskatchewan (SK) that has a population of approximately 1.2 million, with a land area of 591,000 km2 (Saskatchewan Bureau of Statistics, 2025). Substance use professionals with lived experience who met the following criteria were involved in the study: (1) working in a paid job position as a substance use counsellor (or an equivalent position) in substance use treatment agencies in SK, and (2) having personal experience of substance use or being in recovery. Being in recovery was understood and defined as having resolved the severe problems with alcohol or substance use by (a) abstaining from one's drug of choice for a minimum of 1 year before the interview or (b) being in medication-assisted recovery (MAR) or moderation-based recovery for a minimum of 1 year before the interview.
The principal investigator and research assistants conducted in-depth interviews lasting 45–60 min. Most interviews were conducted by phone to ensure inclusivity among participants residing in different communities (rural or urban). The interview questions covered the topics of personal substance use and recovery experience, the journey to become a substance use counsellor or work in an equivalent position, the experiences in the workplace, and the perceived needs for supervision and support. All interviews were transcribed verbatim and then analyzed in NVivo 14.0 to identify themes and patterns in data (Braun & Clarke, 2006; Flick, 2018). The process of thematic analysis included the following stages: (1) immersing in the interview transcripts by reading and rereading them; (2) generating initial codes that represented meaningful clusters of information related to the research questions; (3) organizing and collating the coded data into themes; (4) discussing and reviewing the themes among the researchers; (5) identifying the relationships between the themes; and (6) writing a narrative summary of the themes for member checking with research participants. Recruitment of participants was deemed complete when the team determined that data saturation had occurred and that no new themes emerged. The University REB approved the study, and the participants had the opportunity to discuss confidentiality issues or aspects of informed consent forms before the interviews commenced.
Results
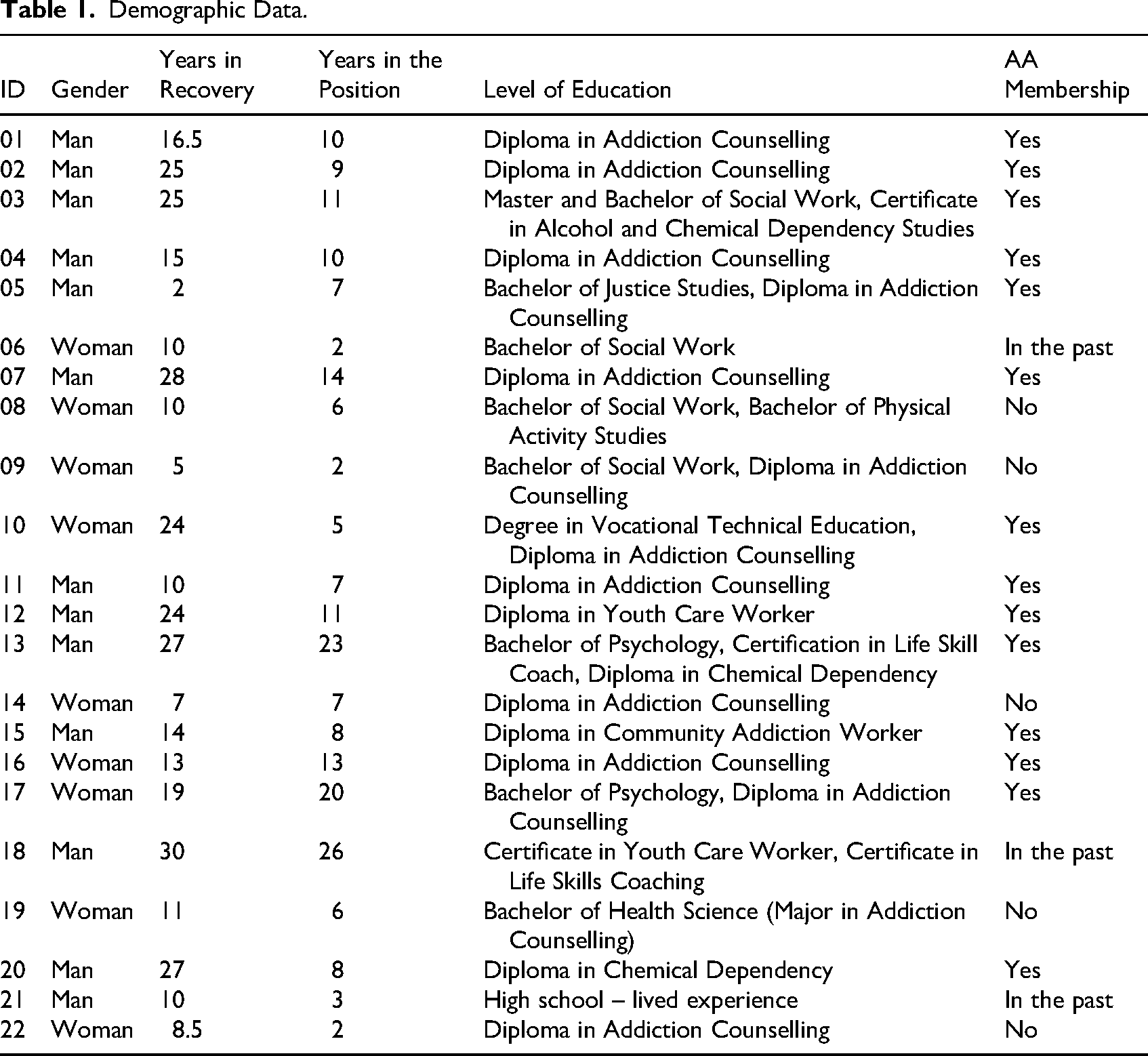
Twenty-two interviews were conducted; 13 men and nine women were given numerical ID numbers that denote their self-identified gender (M/W), active membership in Alcoholics Anonymous (AA) groups (AA), membership in the past (P-AA), or no affiliation with AA or any other mutual group (-) to ensure the confidentiality and relevance of personal attributes to the findings. Most participants who identified as men were in recovery for at least 10 years or longer; only one participant had been in recovery for 2 years at the time of the interview. Women participants’ recovery experience ranged from 5 to 24 years. Participants’ ages ranged between 30 and 60 years. The number of years in their current job ranged from 2 to 26.
Additionally, 14 out of 22 participants reported being active members of AA during the time the study interviews were conducted, and three participants had some experience with either AA or Narcotics Anonymous (NA) at some point in their recovery. Participants were invited to provide any identifiers they considered important; the demographic information collected included age range, number of years in recovery, type of recovery (abstinence based or medication assisted), whether they received treatment, gender identity, and professional training information. One participant shared information about their Indigenous ancestry. Only publicly funded service providers participated in the study. Most participants (15 out of 22) had a diploma or certificate in addiction or chemical dependency counselling; seven had a bachelor's degree, one had a master's degree, and one had graduated from high school. The typical trajectory towards becoming a substance use counsellor was having a personal lived experience of substance use and recovery and then obtaining training, typically a diploma, with some obtaining undergraduate or graduate degrees, and then working in the addiction field. Detailed demographic information is provided in Table 1.
Demographic Data.
Findings
The interviews provided ample data detailing the perspectives of substance use professionals with lived experience on their well-being and professional growth. Findings are organized around four interconnected themes. First, participants described their professional growth as a process, highlighting the importance of judiciously sharing their lived experiences. Second, they reported that stigma and burnout posed significant challenges, contributed to emotional strain, vulnerability to relapse, and compromised well-being, especially in smaller communities where seeking their personal recovery supports risked compromising confidentiality. Third, self-care and self-sufficiency were seen as primary strategies for managing stress amid limited organizational supports. Lastly, participants viewed their lived experience as a valuable source of insight, informing client-centered practice as a key professional strength that complemented evidence-based approaches in their work.
Professional Maturation and Self-Disclosure of Lived Experience
All participants reported having gone or going through self-discovery and personal and professional maturation, whether they adhered to abstinence or understood recovery as a continuum of enhancing their health and well-being by adhering to medication assisted treatment protocols (methadone, buprenorphine, or moderation based). Professional growth was connected to the openness to learning about themselves, with the relationship with learning as a dynamic and continuous process: I think, initially, we think we know a lot. At least I, you know, I felt like I knew a lot. Then, when I started to work more in the field around mental health and substance use, I realized I did not know as much as I thought I did. And then there were periods where I felt I knew a little more, and now I think I'm back to the idea of I don't know as much as the person sitting across from me. (17-W-AA) I probably used more self-disclosure in the early days than I do now. Because I think that I just did not have as much experience or skills. I think that's kind of all I had to fall back on then. (12-M-AA) I don't think I rely as heavily on sharing my personal recovery as I did in my earlier days. I feel a little more confident with my skill set. I mean, like when I first got into it, I was naive, right? Like, I mean, I was going to change the world, and you know, I've lived through it and so on. (05-M-AA) I’ve been very grateful to be put up very healthy boundaries between my personal recovery and my career in the field. Ah, from the very beginning, I’ve been taught that my recovery is mine, right? (01-M-AA) Depending on who the person is, depending on how. I don’t hide my past, but like, I don't get on a pedestal either. So, it's kind of a “need to know” [basis], and if it's important that I share my personal information with people, I will. But if I don't think it's important, I won't. (07-M-AA) Sometimes I use it when I find that a group is struggling to open up, but I don’t always feel that it's necessary. I think that it is an easy way. I think if you want to build a rapport with a client really quickly, you can use it. But I also [think] there is a part of me that thinks it is a cheap way to do it. The client needs to get over their own judgment of you. So sometimes it just takes a little bit longer. But for me personally, I don't use it a lot. (09-W-)
One participant likened self-disclosure to a “# MeToo effect”; they wanted to capture the clients’ attention and reduce stigma so that they would feel comfortable discussing their experiences more openly. Another participant noted that self-disclosure often changes group counselling dynamics as clients become “much more receptive to the information being brought to them” (06-W-PAA).
The professional trajectories towards counsellor positions began for many participants with volunteer work at community treatment centers or detox facilities. Subsequently, as they received employment offers, they pursued their addiction or chemical dependency diplomas from a local college. The lived experience was often used as a source of knowledge and information, particularly in the early days of their professional careers. Although many of the attributes of their professionalism have been related to their history of substance use and how they experienced recovery, with more years in their professional roles, the lived experience became less important. More time spent in the substance use treatment sector also positively affected their sense of what represents healthy professional boundaries.
Stigma, Confidentiality, and Recovery Support
The participants of this study acknowledged that substance use treatment services are an environment that is often fast-paced and underfunded. Along with a lack of support during high stress, suboptimal work conditions can undermine their own recovery efforts: There's a huge rate of relapse, right? Especially like burnout is a f…g bitch. Like, I heard about it, but once I went through it, I was just like, Wow! Right? I just actually came off of like eight months of burnout through the pandemic because we have to work, we have to be here, we're essential. (21-M-P-AA) Like, there's lots of stuff that goes on with the kids that I work with that I can go back and remember and by using myself as an example, it happens all the time. But if we don’t have the recovery, like if I don’t have the sponsor that I can call right after, or go to a meeting with that evening, right? I’m pooched. Because then I dwell, and then my thinking goes back to the way it was when I was using, and all of a sudden, I’m in the stinking thinking phase, and that's the first step to relapse, right? So, if I’m not careful with that, it goes…. (01-M-AA) When I got into the field of addictions [pause] I worked, I was clean for about seven months, and then I relapsed and at my last relapse I ended up getting alcohol poisoning and it was a real reality check for me. It was like I can't work in this field and tell people that... like ask people to be clean if I'm not going to do the same thing. So, it was, it was it had a profound effect on me. And I didn't want to be a hypocrite. I want to work in this field and be with integrity. So, I went back to AA, and I took it seriously. I got a sponsor, and I started doing the emotional work. (05-M-AA) I can be a very open person, but I can be a very closed person. And so, I don't trust a lot of people on my team. I feel judged as I am [in recovery] [pause]. Yes, it's interesting. Still such a huge stigma. (08-W-) Well, so part of it, I think, is societal. So, there is still [pause] you know negative stereotypes, negative connotations about having an addiction and mental health issues [and] what that means. (06-M-AA) In the beginning, it was Alcoholics Anonymous. I ah, I was in a small community with a lot of stigma and a lot of, um, negativity attached to addictions. So, the last thing I wanted to do was to be called an addict. Uhm, I didn’t really see any options in treatment. Those were really never offered to me in inpatient treatment facilities and stuff. Uhm, I did hear of detox before, but didn’t have any knowledge of what it was. So, what happened was … is … I knew some community members that went to AA, and they invited me to a meeting. (01-M-AA) Because it became more difficult in the community in which I work; we have AA-based groups (…) Because of the anonymity and where I work and the people I am seeing, who I know. It's difficult to have that same relationship with those groups. One has to find different ways. (16-W-AA) I have other coworkers, so we created another support group with [pause] for professionals, but we all talk the same language, and we have a really excellent employee family assistance plan. And I utilized that more than anything. (16-W-AA) In case I do run into someone, you know, I don't want to turn into like a counselling situation. I try not to take any clients that are actively attending AA…. Some of the steps, you know, in terms of really being conscious about my own personal boundaries and just being aware of that. I think it helped me a lot considerably. (03-M-AA)
Self-Care and Self-Sufficiency
Most participants indicated that their attitudes towards recovery have shifted as they engaged in more professional reflection, especially after experiencing setbacks in their recovery journey. Since two-thirds of the research participants were involved in abstinence-based 12-step programs at the time of the study, they shared personal insights and realizations related to the support they received in their mutual aid groups. These participants described becoming more aware of their needs and experiencing inner growth, which one of them referred to as self-actualization: Recovery is really about learning about oneself and practicing new skills and techniques, and kind of almost constant quest for (…). I don't know, self-actualization is kind of a big term, but you know, really to be at our best selves. (17-W-AA) I felt a spiritual path and a lot of other things at work. I have a lot of faith in prayer. And, I think, that a shared intergenerational experience and then trying to hang on to some traditional ways of spiritual healing and self-acceptance … those things, I think, help a person. (16-W-AA) So, it was more about I did the things that I like to do without drinking. But it wasn't necessarily still fulfilling some of the spiritual or emotional needs that I needed. I was still doing like … the mental stuff and still the physical stuff, but not the spiritual and the emotional. I believe when they are not all aligned, then that's not what is healthiest. (08-W-)
Participants attributed their self-awareness and the need to take care of themselves to their recovery status and made deliberate efforts to find a balanced life. The concept of self-care, understood and expressed quite broadly, was associated with perceived personal and professional growth: Everyone preaches self-care, right? But that word is used loosely … The level of self-care really has to be defined, and yeah, I know it's different for every person, but just like anything else, it can be, it can be worked on it, right? And it can be used as a tool to help a person not only grow professionally but grow personally, too. (01-M-AA) Uhm with addiction recovery [pause] it's … well … I am gonna be blunt because it's sort of how I am. It's an individual's responsibility for self-care regardless of whether they are in recovery or not. Especially in the social work or addictions field. (16-W-AA) I try to do activities that make me happy. I switched my work schedule so that I wasn’t at work all the time. I go on a lot of vacations. I spend time with friends. I read. I go to school. I like movies. I think I just make sure that outside of my work life is happy and balanced. (09-W-) People are attracted to these fields because they have been damaged, or they’ve been hurt, or they had a family member struggle with something, or they grew up in an abusive household, or they struggled with addiction. That's great, but if you don’t heal your own wounds and you come into this field thinking that you’re going to help somebody else heal when you haven’t dealt with your own stuff, you’re only going to cause more issues.. […] Like, I mean, me working in this field doesn’t mean that this is my recovery. I still need to do things for myself to maintain my own mental and emotional sobriety. (05-M-AA)
Perceived Efficiency and Counsellor–Client Relationships
Participants shared experiences that highlighted challenges in integrating their recovery and professional experiences; however, they remained primarily positive about their work with clients. Most considered themselves client focused and, without judgment or expectations, strove to respect clients’ right to self-determination and individual journey: “you got to meet them where they are at, not where you think they should be at” (18-M-PAA). Acceptance of different recovery paths of their clients came with more professional training and experience and openness to more possibilities in substance use treatment. Although many of the participants reported positive experiences with the 12-step mutual-aid groups in their recovery journey, most of them asserted that instead of advocating for a particular approach to recovery, they remain focused on clients’ specific situations: “I don’t want to be the one who is like, yeah, you need to go to NA and do this and do that, because that's not going to be everybody's path” (21-M-PAA). It was important for some participants to focus on clients’ autonomy and the understanding of the limitations of their own role in the process of individualized treatment plans and interventions for their clients: I mean, I can advocate for abstinence, but at the same time, this is about being client focused. So, I mean, ultimately, at the end of the day, it's their choice on what they want to do, right? I mean, I'm not going to do that recovery for them. I'm going to be here to support them. You know, at the end of the day, if that's the choice they want to make, well, then we'll work with that. (05-M-AA) The person sitting across from me really has a better idea of what they want their recovery to look like. I need to honour what they would like to work on. How do they see it? (…) They need to come to those conclusions, hopefully with my assistance, right? … over time. And that it's not up to me to try to convince some of that. My recovery is my recovery, and their recovery is their recovery. (17-W-AA) It is part of therapy, right? Because that's the piece I don’t have to really study for, right? And when you talk about that emotional and spiritual connection that you have with your clients when you're working with them at a higher level of empathy, you know, you can’t get much higher. It is a huge asset to be able to, especially with the youth, to be able to use the empathy that comes from my background to enhance treatment. (01-M-AA) I kind of believe in the disease concept. So, I mean, I don't believe you have to have had cancer to work with cancer patients, right? So, umm, but I do believe my ability … not necessarily to relate to clients but my ability to engage clients, I think it's been my biggest asset. (12-M-AA) I think I take a blend of my education, what I’ve been mentored, and my own experiences as a youth and now in recovery. I think I kind of mix that all together and come up with a way to connect with these young people with addiction issues. (18-M-PAA) I think that the formal education brings a number of things. I think anybody can provide some degree of support, but I think that we know the formal education just provides so much better road map or understanding of one's own self and of the other person … and you know you figure everything right from their environment to physical health and such. (03-M-AA) You kind of get to a point where you realize that there's more to a skill set than just a personal experience, right? There is a lot of people who work in our field who don't have any recovery experience who can be just as effective. (05-M-AA)
Participants’ comments indicated that their training as substance use counsellors changed their perspectives and made them more flexible in accommodating different approaches in their clinical practice. However, a couple of participants, despite working in harm-reduction-oriented programs, considered abstinence an ultimate goal for substance use issues: Well, in my opinion, for me, recovery is abstinence. And then it's ongoing […]. I don't sugarcoat drinking or drug use. I have a hard time getting my head around that somebody could be a social IV drug user […] Now, maybe it's possible. I don't know. But I have a hard time with that one. So, what can you do if they don't want to quit using drugs or drinking what can you do? So, you're not safe if you're getting it from your parents, maybe you shouldn't drive, or maybe you shouldn't drink, one of the two. You can't do both. If you're getting Hep C and HIV from using dirty needles, maybe you shouldn't use dirty needles, or maybe you should not use them because your liver is going to blow up, maybe you need to think about not using at all. (07-M-AA)
More than half of the participants named several evidence-based treatment methods they use in their counselling approaches, such as motivational interviewing, assessment and prevention of suicides, crisis interventions, cognitive–behavioral therapy (CBT), dialectical behavioral therapy (DBT), social skills training, refusal skills, or trigger-exposure practices: I have a best practice Bible that I follow for drug treatment, right? Like, I mean, that is what we follow most. You know, like I mean, best practices help develop a framework to work within, and then, I think, as professionals, we use our expertise to navigate that and then make sure we are meeting best practices. I firmly believe that you know the best practices are there for a reason, and we should be following them. (05-M-AA)
Discussion
The study contributed to knowledge about how substance use counsellors’ personal recovery management contributes to their transformations at both personal and professional levels. The four themes identified in the findings, specifically, professional maturation and judicial self-disclosure, navigation of stigma and confidentiality when seeking support, self-care as self-responsibility accepted as a first-line strategy, and a positive view of themselves in integrating empathy with evidence-informed practice, together illustrate how substance use professionals with lived experience negotiate personal recovery, professional identity, and the structural demands of the current treatment environment.
Participants’ accounts demonstrated experiencing recovery as a positive process of social identity transformation (Best et al., 2016). However, it is important to note that not all individuals with a stigmatized identity of a person with substance use experience empowerment. Our findings highlight the need for the substance use treatment field to reconsider the support and advocacy for all its professionals (Doukas & Cullen, 2011, 2010). Despite the overall positive changes in participants’ social functioning, some had to reconcile their personal experiences, training, and professional roles, similar to what McGrath and DeDiego (2023) described as managing “narrative tensions” in counsellor trainees with substance use recovery experience. These narrative tensions in our participants were evident as they navigated a sense of pride in their recovery accomplishments while, at the same time, establishing themselves as substance use professionals by becoming more intentional about sharing their personal recovery experiences in their clinical practice to maintain professional boundaries. Some participants were more cautious about relying on personal recovery stories for a variety of reasons that included gaining more insights and training into counselling processes, tailoring the interventions to client needs, and fearing the stigma or emphasis on credentials and professional knowledge. Within the neoliberal context of health care, counsellors’ lived experience is often instrumentalized to signal organizational inclusivity, while simultaneously being devalued and still stigmatized as insufficiently professional (Bell et al., 2025).
Some participants in this study benefited from structured, formal treatment programs as they embarked on their own recovery journey. However, similarly to what other research posited, there were a few who embraced change in their substance use through mutual-help groups only, notably AA or NA, due to a lack of specialized substance use services in their communities (Miller et al., 2024). Two-thirds of the participants reported actively partaking in a 12-step program at the time of the interview, either as a pathway to or as support for continued recovery. This tradition aligns with early research supporting the integration of an AA fellowship and counsellors’ training, leading to increased emotional stability and improvements in overall functioning, well-being, and quality of life (Curtis & Eby, 2010; Kelly et al., 2009; Morgenstern et al., 1997; Polcin & Zemore, 2004; White et al., 2003; Zemore & Kaskutas, 2004). Active involvement with AA also indicates the proliferation of abstinence-based recovery and mutual-help groups , which is viewed as a more desirable outcome aligned with the neoliberal perspective on managing one's well-being through individual actions and responsibility (Carton, 2018; Fry et al., 2023; Oberleitner et al., 2021).
All participants commented on burnout and stigma at their workplace associated with their recovery experiences or substance use. These experiences are aligned with research on stigma associated with substance use disorder and recovery of various groups, including substance use treatment workers. Notably, the work of Eaton et al. (2015), and Zwick et al. (2020) showed significant consequences of self-stigma on treatment access in general, as well as psychological well-being and, consequently, job satisfaction and sense of fulfillment in professional roles of substance use counsellors in recovery. Furthermore, the professionals who adhere to MAR feel that there is more skepticism towards their well-being and professionalism due to ongoing myths and misconceptions about MAR as substituting one drug for another or being considered a temporary measure that should lead to total abstinence and “redemption”. Challenging stigmatizing language and assumptions about recovery is among the strategies considered pivotal for addressing stigma and related negative consequences (Aronowitz et al., 2022; Volkow et al., 2021).
To continue supporting themselves in the absence of broader organizational and system changes, mutual-help groups remained the primary source of support. Given the province's geographic nature, participating in mutual-help groups involved sharing resources with clients, as the two largest cities in the province have approximately 200,000 residents. Therefore, to maintain professional boundaries and the confidentiality of their personal recovery journeys, creating mutual-help groups for professionals or communities of practice could be one way to address the realities of living in smaller communities or of sharing recovery resources with clients.
Our findings also illuminate self-care practices among substance use counsellors in recovery, which they see as both a professional obligation and a personal responsibility for maintaining the quality of their services (Vilardaga et al., 2011). Generally, participants viewed their well-being and professionalism as their own responsibility to prevent relapse and manage stress. Although a few mentioned health benefits and access to counselling through EAP, self-care was regarded as one of the most vital individual-level buffers against stress and burnout. Challenges in maintaining work–life balance were readily accepted as a primary cause of relapse or difficulties in their professional roles. These perspectives align with the neoliberal environment of high-income countries, where public funding for mental health and substance use services continues to decline, placing the responsibility for quality care on individual counsellors (Ross et al., 2022). Furthermore, the rise of the “self-care” narrative in neoliberal society claims that everyone should strive to perform at their best to keep up with the ideal of high efficiency and productivity, even in emotionally demanding professions like substance use or addiction counselling, social work, or other helping professions (Badr, 2022). Participants in this study fully embraced these narratives, highlighting techniques such as mindfulness, physical activity, and personal hobbies as lifestyle choices that could serve as countermeasures to a lack of support, training, or acknowledgment of structural inequalities in substance use treatment systems. While many adopted self-care practices aligned with mainstream wellness approaches, such as mindfulness or exercise (Badr, 2022), a few relied on holistic or community-centered forms of care. One participant linked recovery and well-being to Indigenous cultural traditions and collective belonging, emphasizing the importance of culturally grounded self-care methods. This approach echoes the call for a more radical self-care model that emerged in the 1960s (Wyatt & Ampadu, 2022), emphasizing community care that prioritizes mutual responsibility and collective well-being over individual indulgence or market-driven wellness pursuits. The contemporary idea of self-care has been criticized for drifting away from its original meaning, which was rooted in strategies for marginalized groups to resist discrimination and reclaim autonomy over their health and well-being (Badr, 2022; Wyatt & Ampadu, 2022). The modern “wellness industry” has largely co-opted self-care into a neoliberal framework that focuses on consumerism, individual optimization, and productivity, rather than understanding self-care as a collective practice aimed at survival, solidarity, and social justice. The reasons for the higher number of male participants and AA members in this and other studies remain unclear (Ellis et al., 2024; Shaari, 2022). Though the participants in this study did not explicitly elaborate on their social locations, from their shared experiences, many came from small rural areas or towns that did not necessarily have many substance use treatments. One participant who identified as Indigenous commented on their involvement with their community as a form of belonging and healing. Though aware of the risk of cultural misappropriation of the lived experiences of some ethnic and cultural groups, we argue for the practice of radical self-care by members of all underserved communities, practiced collectively and with respect for their cultural values. Badr (2022), in their analysis of the self-care concept, co-opted by the neoliberal wellness industry, also called for a holistic and community-based approach to productivity and wellness within a social system that would reduce inequities and profit-making across different traditions within a business model of health and well-being.
Besides the importance of a relationship with oneself, many participants viewed counsellor–client therapeutic relationships as empathetic, with counsellors’ personal recovery deepening their understanding of clients’ experiences (McAuliffe, 2002; Pietkiewicz & Skowrońska-Włoch, 2017; Rácz et al., 2015). Participants felt confident about weighing the benefits and risks of self-disclosure, and the need to rely on their recovery experience in clinical work diminished with more training and professional experience. Nevertheless, the lived experience of substance use and recovery was seen as essential to their professional work, which aligns with research suggesting that the professional self does not mean the disappearance of the recovering self (Rácz et al., 2015). Combining knowledge from training, techniques, personal beliefs, and life experience is a key feature of professional counselling practice (Rønnestad & Skovholt, 2003, 2012). Nevertheless, Dixon and Chiang (2019) warned that one's effectiveness as a counsellor could become a professional liability if such assumptions lead to overconfidence or a lack of reflexivity.
Part of the participants’ professional development was the reported use of counselling approaches considered evidence informed in the substance use treatment field, namely, motivational interviewing, CBT, or DBT. This finding contrasts with earlier studies that reported that substance use counsellors in recovery were less likely to use evidence-based practices if they were incongruent with their own abstinence-based recovery model (Burke & Clapp, 1997; Culbreth, 2000; Hoffman & Bevacqua, 2010; Thombs & Osborn, 2001; Toriello & Benshoff, 2003; Toriello & Leierer, 2005) or their own recovery-based experiences (Jack et al., 2011; Novotna, Dobbins, Henderson, et al., 2015; Novotna, Dobbins, Sword, et al., 2015). Greater awareness and acceptance of evidence-informed practices may be related to increased training and counsellor certification requirements (Canadian Centre on Substance Use and Addiction, 2021).
Study Limitations and Delimitations
This study has some limitations. First, this research explored the lived experiences of substance use disorder or addiction and recovery of counsellors within the context of one province—SK, Canada. The Prairies have historically had a higher percentage of substance use counsellors in recovery working in addiction services (Ogborne & Graves, 2005), likely due to the province's geographic attributes. Many rural areas rely on AA mutual-self-help groups to fill the void in providing publicly funded addiction treatment services. The research team had difficulties recruiting participants in medication-assisted recovery (i.e., Opioid Agonist Therapies or controlled drinking), likely due to harm-reduction-informed services still trying to find their place in the landscape of substance use intervention in some jurisdictions. Therefore, the study does not account for a greater diversity of recovery experiences. Additionally, the study presents information on how substance use counsellors perceived themselves, but it does not provide additional data to corroborate their perceptions and observations. Nonetheless, the research project has provided important insights that can inform further research and practice development in the field, as well as education and training for this population of service providers, with consideration for different communities and geographic jurisdictions.
Conclusion
The findings of this project emphasize that professional development of substance use counsellors as individuals is embedded in the process of personal transformation. The presence of substance use counsellors in recovery can benefit the substance use treatment field in connecting clients who often feel disenfranchised and stigmatized, even within the very treatment sector that is supposed to support them in achieving a better quality of life. However, more research is needed to bring forward the concept of recovery as a continuum of increased well-being rather than a simple abstinence/addiction dyad.
Footnotes
Acknowledgements
The authors would like to acknowledge the help of student research assistant Markus Beveridge, who contributed to data analysis in the initial stage of the project. The contribution, while important, did not meet the criteria for authorship.
Ethical Considerations
The project received approval from the University of Regina Research Ethics Board, # BEH 2018-051. All participants provided informed consent to participate in the study and to have their findings published in peer-reviewed journals and at conferences.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Saskatchewan Health Research Foundation (SHRF) (#4109 Establishment Grant).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author, G.N. The publicly available data could compromise the privacy of research participants, and additionally, participants did not give consent for data sharing in an open data repository.
AI Transparency Statement
The authors used Grammarly to support grammar and style editing. All intellectual content is solely the authors’ own.